
Abstract
Background:
Bazex syndrome (acrokeratosis paraneoplastica) is a rare paraneoplastic syndrome that usually occurs in males over 40 years old and is particularly associated with squamous cell carcinoma of the upper aerodigestive tract and adenopathy above the diaphragm.
Objective:
The objectives of our article are (1) to describe a unique case of acrokeratosis paraneoplastica and (2) to review the current literature regarding skin findings, commonly associated neoplasms, and treatment options relative to this condition.
Patient:
We describe a 68-year-old female with lobular breast carcinoma, complicated by local and distant recurrences, who presented with a 1-year history of prominent acral skin and nail changes.
Results:
Our patient's clinical skin findings improved significantly following treatment and partial remission of her underlying malignancy.
Conclusions:
Our patient represents one of few females described with this syndrome, which is especially rare in association with lobular breast carcinoma. Further, the patient's presentation is unique as she was discovered to demonstrate laboratory findings consistent with coexistent porphyria cutanea tarda and relative zinc deficiency.
BAZEX SYNDROME (ACROKERATOSIS PARANEOPLASTICA) is a rare cutaneous syndrome comprising acral psoriasiform skin changes and nail dystrophy that is almost invariably associated with a malignancy of the aerodigestive tract. 1 It was first described by Gougerot and Grupper in 1922 and then further expanded by Bazex and colleagues in 1965. 2 This syndrome should not be confused with the Bazex-Dupré-Christol syndrome (BDCS) described by Bazex and colleagues in 1966. 3 BDCS is characterized by follicular atrophoderma, hypotrichosis, multiple genetically induced epitheliomas, and disorders of sweating, such as anhidrosis.4,5 It is an important distinction because BDCS is an inherited genodermatosis without paraneoplastic associations. 6
Bazex syndrome has been reported mainly in Caucasian males over the age of 40 years.4,7,8 The essential components of this syndrome are (1) an underlying internal malignancy and (2) one or more of the following cutaneous signs: (a) acral papulosquamous lesions, (b) hyperpigmentation, (c) keratoderma, (d) paronychia, and (e) nail dystrophy. 9 The clinical course begins with lesions on the hands, feet, ears, and nose that extend progressively to the arms, legs, and trunk as the malignancy itself evolves. 2 Recognition of this condition is important as the characteristic skin lesions are often the first clinical sign of a malignancy. A review of 113 cases (105 men and 8 females) reported that acrokeratosis paraneoplastica preceded the diagnosis of an underlying malignancy in 67% of cases. 9
We describe a case of Bazex syndrome associated with lobular breast carcinoma; the condition improved to near-complete resolution as the malignancy went into partial remission.
Case Report
A 68-year-old Caucasian female was evaluated by our dermatology service during a hospital admission in October 2002 for dyspnea, dehydration, anemia, and abdominal cramps associated with bright red rectal bleeding. She had an associated eruption on her hands and face that had been present for 1 year and had become more prominent over the last 3 months. The patient also described a previously undiagnosed 7-year history of photosensitivity of the face and hands expressed as erythema, occasional blisters, and altered facial pigmentation. However, she had been restricted to the indoors over the previous 6 months and denied any episodes of sun-related eruptions over that time.
Dermatologic examination showed hyperkeratotic plaques with fissures and ulceration affecting the dorsum of both hands, most prominently over the joints (Figure 1). Nail dystrophy affected multiple nails of the fingers and toes. Fissured, eroded, scaly plaques and papules also affected the periorbital skin, nose, forehead, chin, and ears (Figure 2). Hypo- and hyperpigmentation were also evident on the face. Skin of the face, forehead, and temples (see Figure 2) and, to a lesser extent, that of the hands was firm and bound down. No blisters or milia were noted on the dorsum of the hands.

Clinical photographs of the hands and toes of the left foot show erythematous to violaceous psoriasiform plaques, fissuring, onycholysis, and nail dystrophy. The inset (lower left panel) shows a closer view of the left index finger.

Clinical facial photographs show involvement of the ears, forehead, and chin and illustrate crusted and eroded plaques around the eyes and scaly plaques affecting the nose (at arrow, lower panel).
The patient provided a history of invasive lobular carcinoma of the left breast diagnosed in 1987 and treated with a combination of mastectomy and radiation. Chest wall recurrences were surgically excised in 1991 and 1995, and metastatic infiltration of the lungs, bones (cervical spine, femur, pelvis), and mediastinal lymph nodes was diagnosed in August 2002 both radiologically (radiographs, computed tomographic scan) and by nucleotide bone studies. Metastatic spread coincided with the onset and worsening of the skin eruption. She was treated with weekly docetaxel (Taxotere, 30 mg/m2/wk), a member of the taxoid family of antineoplastic agents, for a 6-week course between August 19 and September 27, 2002. She had also been receiving epoetin alpha (Eprex). The patient reported a 14-pack-year smoking history.
The dermatologic differential diagnosis included acrokeratosis paraneoplastica associated with the metastatic breast carcinoma, psoriasis, disorders of nutritional deficiency, and drug reaction. This latter possibility was unlikely related to docetaxel given that the onset of skin symptoms preceded the initiation of chemotherapy. The history of photosensitivy and sclerodermoid changes affecting sun-exposed areas suggested coexisting porphyria cutanea tarda. Cultures of periorbital eroded plaques for herpes simplex virus and bacteria were negative. A biopsy from a hyperkeratotic plaque on the dorsum of the right hand showed changes at the level of the superficial dermis and epidermis (Figure 3). The dermis appeared to be mildly fibrotic, with a mild perivascular lymphocytic infiltrate. The epidermis was thickened with mild parakeratosis and contained scattered necrotic keratinocytes and patchy vacuolar degeneration, and the keratinocytic cytoplasm showed eosinophilic hyalinization, giving the epidermis a glassy appearance. These clinical and biopsy findings are most consistent with acrokeratosis paraneoplastica, as discussed below.
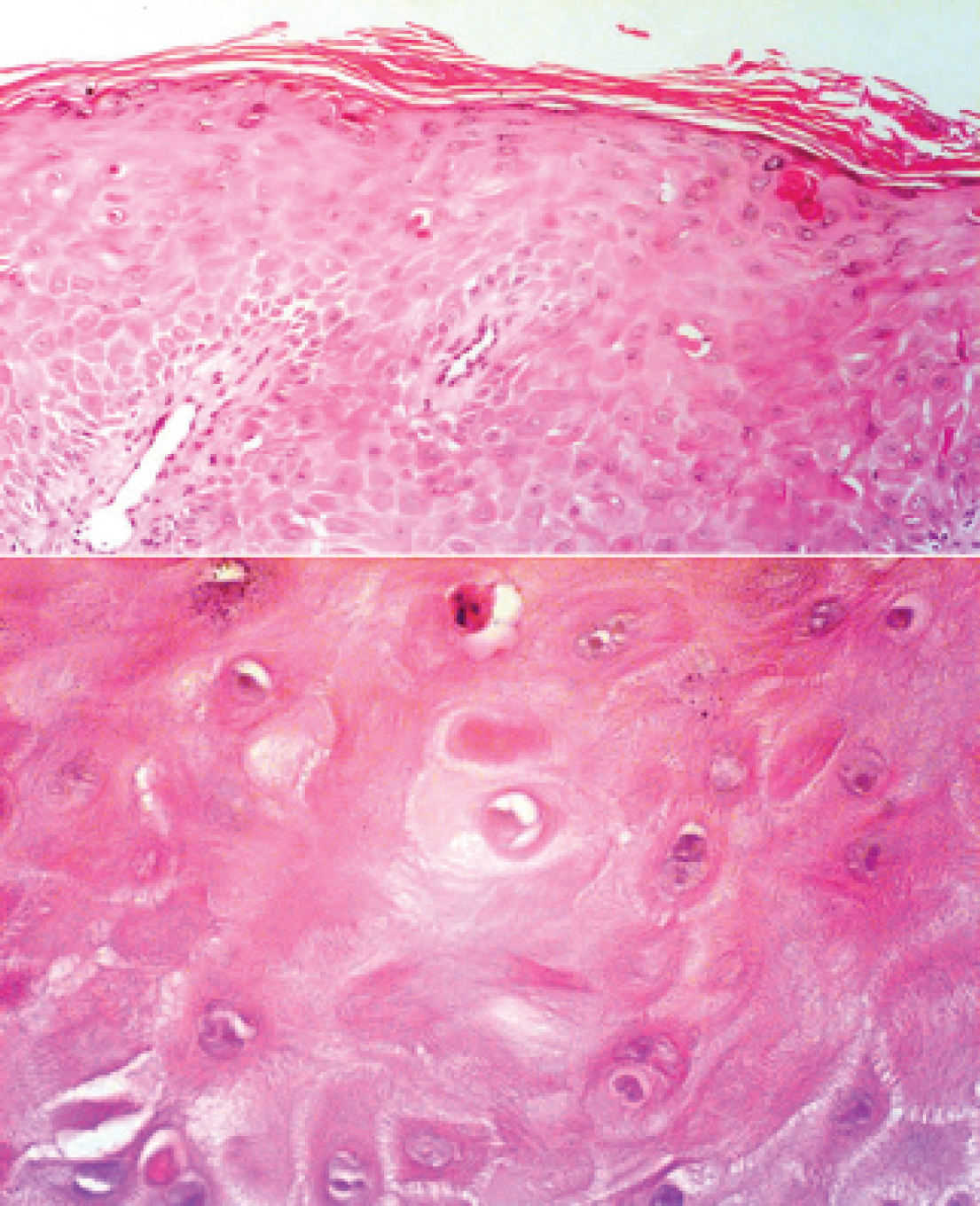
Histopathology slide stained with hematoxylin and eosin and viewed at low (upper panel) and higher (lower panel, epidermis) magnification shows acanthosis with mild parakeratosis, dyskeratotic keratinocytes, cytoplasmic eosinophilic hyalinization of enlarged keratinocytes, patchy vacuolar degeneration of the basal layer, and a mild perivascular lymphocytic infiltrate (upper panel, × 40 original magnification; lower panel, × 400 original magnification).
Serum albumin was 24 g/L (35–50 g/L) and serum zinc was 5.8 μmol/L (8.0–20.0 μmol/L). Serum ferritin was greatly elevated at 966 μg/L (12–300 μg/L). A urine porphyrin screen was positive, and a 24-hour urinary uroporphyrin quantitation showed an elevated excretion of 408 nmol/24 h (normal < 51 nmol/24 h). Urine coproporphyrin and erythrocyte protoporphyrin were within normal limits, suggesting porphyria cutanea tarda. No therapeutic intervention has been necessary in this respect other than sun avoidance.
During admission, sigmoidoscopy with mucosal biopsies showed colitis, likely of infectious etiology. This was treated with levofloxacin with good results. Dyspnea was associated with anemia (blood transfusion provided) and bilateral malignant pleural effusions. Management of the skin lesions was conservative, using topical fusidic acid ointment to open areas. The patient's general and cutaneous condition improved during the 8-day admission as the colitis, dehydration, pleural effusion, and nutritional status were effectively managed. Within 2 months of the initial encounter, skin lesions were significantly improved, and follow-up after 5 months showed marked improvement: lesions on the face and on the dorsum of the hands were almost clear (Figure 4). Dystrophic nail changes, however, persisted despite treatment of her underlying medical conditions (see Figure 4). Serum zinc levels returned to the normal range (13.7 μmol/L) within 2 months with oral zinc sulfate administration. Therefore, the improvement in the acral psoriasiform plaques coincided with partial remission of the metastatic breast carcinoma, providing further evidence of acrokeratosis paraneoplastica. In August 2004, the patient remained in partial remission regarding the breast carcinoma, with persisting evidence of asymptomatic bone metastases but without visceral disease. She has been treated with letrozole since January 2003.

Clinical photographs of the patient's face and fingers of the left hand taken 5 months after the initial presentation. The face shows near-complete resolution of clinical findings, whereas the nails are destroyed, testament to the very destructive nature of the pathologic process when affecting the fingers.
Discussion
Bazex described acrokeratosis paraneoplastica as a cutaneous syndrome that evolves in three distinct stages.7,10 First, there is a symmetric eruption of erythematous scaly lesions on the fingers and toes, followed by involvement of the ear helices and bridge of the nose. The lesions are typically described as erythematous to violaceous in color with an associated scale. Less frequently, patients develop erosions, crusting, bullae, and/or vesicles. 11 Nail changes include dystrophy (thickening, curling of the nails, ridging, yellow discoloration), 8 subungual hyperkeratosis, onycholysis, and destruction of the nail plate.7,12 Second, the skin lesions progress centrally as the neoplasm becomes detectable, often coincidentally with metastases to cervical lymph nodes. Third, there is involvement of the extremities and trunk as the malignancy continues to evolve.
Sarkar and colleagues found that the most common malignancy associated with Bazex syndrome is squamous cell carcinoma of the oral-pharyngeal-laryngeal regions, with 40% of individuals having this presentation. 13 Other primary sites of malignancy commonly associated with Bazex syndrome include the lungs (19% of cases), unknown primary tumors (16%), and the esophagus (13%). 13 Other authors describe cases in association with bladder carcinoma, 14 metastatic neuroendocrine tumors, 15 adenocarcinoma of the colon, 16 Hodgkin's lymphoma, 17 and carcinoma of the liver, prostate, stomach, thymus, uterus, and vulva. 2 There has been only one other case report of Bazex syndrome associated with carcinoma of the breast. 18 Four cases of Bazex syndrome have been associated with porphyria cutanea tarda.11,13
Histopathologic changes are nonspecific 19 but allow exclusion of other eruptions that may appear clinically similar to acrokeratosis paraneoplastica. 6 The most common findings reported by Bolognia, from a review of 61 biopsies from 45 patients, were hyperkeratosis, acanthosis, parakeratosis, dyskeratotic keratinocytes, and perivascular lymphocytic infiltrate. 12 Vacuolar degeneration and incontinent melanin were seen in several specimens. 12 Other authors noted eosinophilic hyalinization of cytoplasm of individual spinous cells and fibrinoid degeneration of the vessels in association with lymphocytic infiltration resembling vasculitis.19,20
The pathogenesis of this syndrome is not fully understood. Since the majority of associated tumors have been squamous cell carcinomas, there may be an antibody response to a tumor antigen that cross-reacts with a basement membrane zone antigen of the skin (as has been described for tumor-associated bullous pemphigoid). 12 This antibody-antigen complex at the dermal-epidermal junction is postulated to evoke an immune reaction mediated by complement, which could further stimulate epidermal or immunocompetent cells to be activated and produce the clinical findings. 20 Squamous cell carcinoma cell lines have been shown to secrete transforming growth factor α (TGF-α) and insulin-like growth factor, both of which act as growth factors for human keratinocytes. 12 There are also reports of benign keratinocytic hyperplasia secondary to overexpression of TGF-α in nude mice. 12
However, not all individuals with Bazex syndrome have squamous cell carcinoma, and the majority of patients with squamous cell carcinoma do not develop Bazex syndrome. Based on the zinc deficiency seen in our patient, we advance the hypothesis that zinc deficiency alone or in combination with other nutritional deficiencies could play a role in the evolution of this disease. Zinc is critical to protein, carbohydrate, and vitamin A metabolism; cell proliferation; and healing and tissue repair. 21 Zinc deficiency is known to cause acrodermatitis enteropathica (AE), an autosomal recessive disorder characterized by acral dermatitis, alopecia, and diarrhea. Some cutaneous manifestations of this disease, that is, the acrally located erythematous, scaly, crusted, psoriasiform lesions, are similar to those seen in Bazex syndrome. AE is also similar to Bazex syndrome histologically, with diffuse parakeratosis and psoriasiform epidermal hyperkeratosis and the presence of large, pale, hazy keratinocytes with loss of normal basophilia and dyskeratotic cells. 22 Although hereditary AE occurs primarily in infants, zinc deficiency can cause an acquired variant of AE in adults related to, for example, intestinal malabsorption, inflammatory bowel disease, and malignancies. 21 Although our patient's zinc levels were not depleted to an extent that would be expected to cause acquired AE, we suggest that a relative deficiency with an inability to use zinc effectively could be a contributing factor to the etiology of Bazex syndrome in general and our patient in particular. The patient's elevated tissue stores of iron, as documented by the greatly increased serum ferritin and likely related to porphyria cutanea tarda, could interfere with zinc availability in skin. For example, iron could compete effectively with zinc for the zinc-iron regulated transporter-like (ZIRTL) gene product, a member of the family of divalent metal ion transporters shown to be present in epidermis. 23 Further, in squamous cell carcinoma of the head and neck, serum ferritin has been positively correlated with tumor load 24 and zinc levels were decreased only in male patients 25 and were inversely related to tumor burden. 26 These findings could explain the male predominance of acrokeratosis paraneoplastica and its association with upper body solid tumors, based on relative zinc and iron bioavailability. To our knowledge, no previous reports relate zinc deficiency to the pathogenesis of Bazex syndrome, although vitamin A deficiency has been reported as a possible etiologic factor. 11
The recognition of cutaneous manifestations of Bazex syndrome provides clinicians with an opportunity to investigate, diagnose, and treat associated neoplasms at an earlier stage. In one series, skin lesions preceded diagnosis of the neoplasm by an average of 11 months in 63%, coincided with the diagnosis in 21%, and followed the diagnosis of a neoplasm in 16% of patients. 12 The cutaneous lesions often evolve as a function of the status of the underlying malignancy; this was shown in 93% (81 of 87) of patients in whom skin lesions improved significantly when the underlying malignancy was effectively treated or remained unchanged when the malignancy persisted. 9 Recurrence of tumors (primary or metastases to cervical lymph nodes) has also been reported following the recurrence of the cutaneous eruption. 9 Persistence of residual nail changes is common despite the resolution of other cutaneous findings following successful treatment of the malignancy. 19
Symptomatic treatment of acrokeratosis paraneoplastica may result in slight improvement, but lesions will usually not clear until the underlying neoplasia is successfully treated. 27 In the present case, improvement of cutaneous findings coincided with remission of the underlying malignancy. Reported examples of unsuccessful cutaneous treatments include topical keratolytics, corticosteroids, tar, antifungals, and antibiotics. 12 Oral etretinate has been reported to be effective therapy for the psoriasiform eruption in cases of this syndrome in which the underlying malignancy was not resectable and/or was resistant to treatment. 28 Improvement in skin findings has also been anecdotally reported after treatments with oral prednisone, topical salicylic acid, and topical vitamin D2. 9 Two reports have shown psoralen plus ultraviolet A to be an effective treatment for acral hyperkeratosis.1,8
Conclusion
This case of Bazex syndrome is intriguing owing to the unique presentation of our patient: a female with coexistent porphyria cutanea tarda and metastatic breast carcinoma. In a 1998 review by Sarkar and colleagues of 112 cases of Bazex syndrome, only 7 of the patients were female and only 1 female patient had coexistent documented porphyria cutanea tarda. 13 Further, there has been only one other report documenting a case associated with breast cancer. 18 We also describe a relative zinc deficiency state in our patient and hypothesize that it alone or in combination with other nutritional deficiencies could be etiologically related to the acral hyperkeratosis. As previously reported, marked improvement in the cutaneous lesions occurred only when the patient's metastatic disease was successfully treated to a state of partial remission.