
Abstract
Background:
Cryotherapy is the standard of care for clinically apparent (target) actinic keratoses (AKs). Topical imiquimod may reduce initially inapparent or subclinical AKs.
Objective:
We evaluated the potential of topical imiquimod to decrease subclinical AKs after cryotherapy of target AKs.
Methods:
A randomized trial of imiquimod or vehicle twice weekly for 8 weeks following 3- to 5-second cryotherapy of target AKs within a 50 cm2 field at the face or scalp was conducted. Efficacy outcomes included clearance of target, subclinical, and total AKs and proportions clear of AKs. Subjects with residual AKs were offered cryotherapy and open-label imiquimod twice weekly for 8 weeks.
Results:
Sixty-three subjects completed the randomized phase. At 12 weeks, target AK clearance was similar for imiquimod and vehicle (79% vs 76%), but fewer total AKs were noted for imiquimod (78 vs 116). This was due to a progressive reduction in subclinical AKs with imiquimod compared with a progressive increase with vehicle. More subjects treated with imiquimod achieved clearance of subclinical (58% vs 34%; p = .06) and total (23% vs 9%; p = .21) AKs.
Conclusion:
Imiquimod postcryotherapy may increase clearance of subclinical and total AKs and proportions of subjects clear at 3 months. These findings require confirmation in larger controlled trials powered for statistical significance.
ACTINIC KERATOSES (AKs) are considered premalignant precursors and the early stage of a biologic continuum culminating in squamous cell carcinoma (SCC). The majority of SCCs have been demonstrated to arise in contiguity with an AK. 1 Although the presence of AKs identifies those most predisposed to the development of an SCC, there is no current method to predict which lesions will so progress. 2 Accordingly, lesional destruction is the current standard of care for AKs. Cryosurgery and curettage are the most commonly used therapies in the treatment of AKs, with cryosurgery considered the standard of care. Topical therapies such as 5-fluorouracil and imiquimod have also been shown to be effective agents but are rarely used as monotherapy. 3 Although locally destructive therapies such as cryotherapy and curettage focus on clinically apparent lesions or target AKs, the concept of field cancerization in epidermal tumors has increased recognition of the need to also treat clinically inapparent or subclinical AKs. 4 Imiquimod, recently approved for the treatment of AKs, is believed to stimulate immunologic memory and may result in a long-term reduction in AKs in the epithelial field. Recognizing that cryotherapy is considered the standard of care for target AKs, this pilot study was initiated to evaluate the potential of imiquimod to eliminate subclinical AKs and to reduce the total burden of AKs following cryotherapy.
Methods
This study was approved by a central ethics review board and conducted according to the Declaration of Helsinki protocol. After informed consent was obtained, subjects 18 years and older with four or more discreet AKs on the face or balding scalp within an area not exceeding 50 cm2 were recruited. Participants were excluded if they had a known hypersensitivity to imiquimod cream; had previous treatment with imiquimod in the prescribed area within the past 5 months or cryosurgery in the same area within the past 4 weeks; had previous use of interferon or interferon inducers, immunomodulators, immunosuppressants, cytotoxic drugs, or investigational drugs for conditions other than AK less than 4 weeks before the start of the trial; had a bacterial or viral infection less than 2 weeks before study start; or were pregnant or breast-feeding. Additional exclusion criteria included concomitant medical conditions, which, in the investigator's opinion, may have confounded clinical evaluations or interfered with study assessments or outcomes; subjects unwilling to comply with photoprotection throughout the study duration; or the presence of basal or squamous cell carcinomas in the prescribed treatment area.
This study was composed of two phases after cryotherapy of preexisting (target) AKs comprising a 3-to 5-second freeze cycle with liquid nitrogen. The initial randomized double-blind phase in which subjects were allocated to either vehicle or imiquimod 5% cream twice weekly for 8 weeks was followed by an optional open-label phase in which subjects with residual AKs at week 22 were offered the choice of either repeat cryotherapy followed by imiquimod cream twice weekly for 8 weeks or no treatment (Figure 1). This frequency and duration of dosing were selected to reduce the potential for local intolerance and to improve subject acceptability compared with thrice-weekly applications. Subsequently, subjects attended a follow-up visit at 34 weeks and a final visit at 62 weeks after their initial cryotherapy treatment.
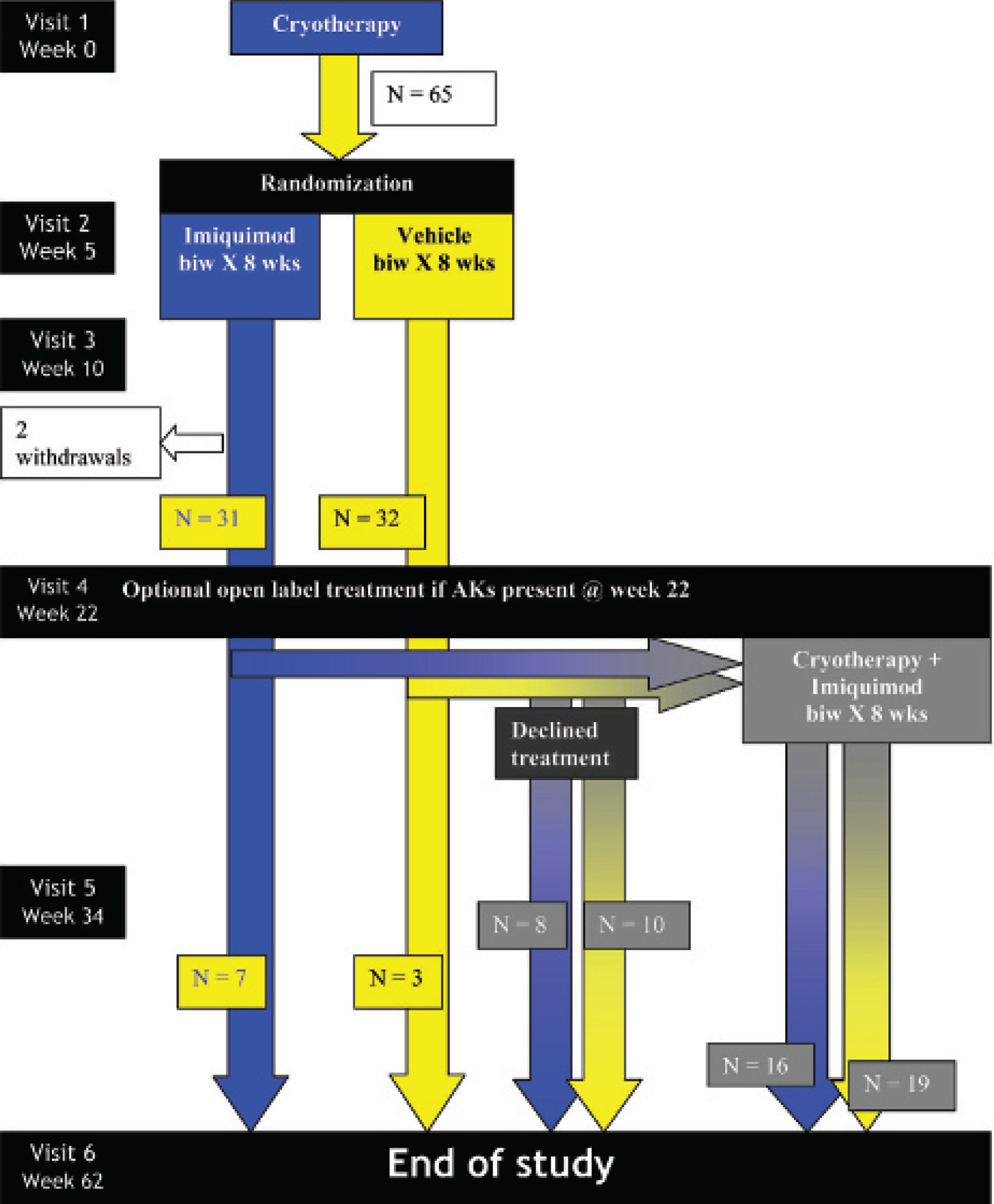
Protocol schematic and subject distribution. AK = actinic keratosis.
The primary analysis was to determine the efficacy of cryotherapy followed by either imiquimod cream versus vehicle twice weekly for 8 weeks on the clearance of target and subclinical AKs in the predefined treatment field. The secondary efficacy outcome was the proportion of subjects clear of AKs.
The open-label phase provided the opportunity for exploratory analysis of the efficacy of a second course of imiquimod following cryotherapy and of the long-term efficacy of a single course of treatment.
Safety
Safety was monitored at every study visit. The frequency and duration of adverse events (local and systemic) and discontinuations owing to adverse events were tabulated by treatment group.
Statistical Analysis
Target AKs were defined as those within a designated 50 cm2 treatment field established at baseline and identified on a transparent overlay map for future reference.
Subclinical AKs were those within the designated treatment field inapparent at baseline. Total AKs represent the sum of target and subclinical AKs.
Primary efficacy analysis compared the outcome parameters of (1) the clearance rate of target, subclinical, and total AKs and (2) the proportion of subjects completely clear of AKs at visit 4 (week 22) between the two treatment groups in the randomized controlled phase.
Exploratory analysis of long-term efficacy was based on evaluation of outcome parameters at week 62 for the three different cohort pairs following the randomized phase: those with residual AKs at week 22 who proceeded into open-label treatment with cryotherapy and imiquimod twice weekly for 8 weeks; those with residual AKs who declined open-label treatment; and those without residual AKs (see Figure 1). Owing to the two phases of the study, the following were potential treatment cohorts:
Cryotherapy + no imiquimod/0: vehicle group in course 1; no residual AKs at week 22; no retreatment in course 2
Cryotherapy + 1 imiquimod/0: active treatment group in course 1; no residual AKs at week 22; no retreatment in course 2
Cryotherapy + no imiquimod/R: vehicle group in course 1; residual AKs, but declined retreatment in course 2
Cryotherapy + 1 imiquimod/R: active treatment group in course 1; residual AKs, but declined retreatment in course 2
Cryotherapy + 1 imiquimod: vehicle group in course 1; residual AKs and retreatment in course 2
Cryotherapy + 2 imiquimod: active group in course 1; residual AKs and retreatment in course 2
Comparisons between treatment groups were made with the use of a Mann-Whitney-Wilcoxon test for continuous end points and the Pearson chi-square test (the Fisher exact test was substituted if more appropriate) for binary end points. This pilot study was not powered for statistical significance.
Results
Of 65 subjects randomized, two subjects from the imiquimod arm were withdrawn (one for noncompliance, the other for death owing to an unrelated cause: heart disease).
Thus, 63 completed the entire trial. Data for visit 5 and 6 were unavailable for one subject. Accordingly, the analyses at these visits were based on 62 subjects.
The demographics of subjects randomized to the two treatment groups at baseline were similar for age, gender, and target AKs (Table 1).
Demographics of Subjects at Baseline

AK = actinic keratosis.
The frequency distributions of target, subclinical, and total AKs between groups in treatment course 1 are shown in Figure 2. Following initial cryotherapy, the clearance rate of target AKs at visit 4 (week 22) for the group randomized to imiquimod (79.3%) was not significantly different from that in the group receiving vehicle (76.0%). One hundred twenty-eight subclinical AKs were detected with imiquimod and 120 with vehicle. However, the time course of appearance differed with imiquimod treatment, resulting in earlier uncovering of subclinical AKs and subsequent progressive clearance in contrast with vehicle in which subclinical AKs progressively increased in number. At week 22, the number of total AKs was 78 in the imiquimod group compared with 116 in the vehicle group (p = .147).
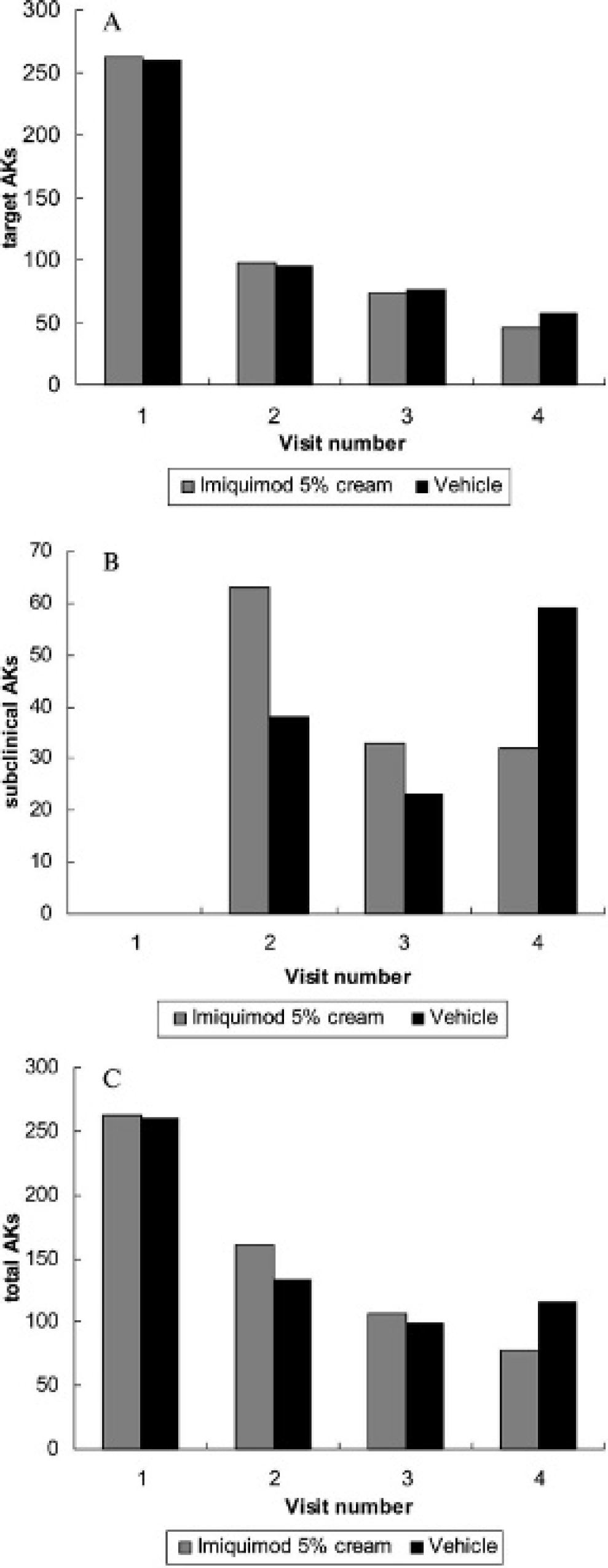
A, Target actinic keratoses (AKs) in the randomized treatment phase. B, Subclinical AKs in the randomized treatment phase. C, Total AKs in the randomized treatment phase.
The proportions of subjects completely clear of target AKs at week 22 were not significantly different between the imiquimod (41.9%) and vehicle (37.5%) groups. However, a higher proportion of subjects in the imiquimod-treated group achieved clearance of subclinical AKs (58.1%) compared with vehicle (34.4%), but the difference was just beyond the threshold for significance (p = .059). A greater proportion of patients was completely clear of AKs on imiquimod compared with vehicle, but the difference was not significant (22.6% vs 9.4%; p = .211).
At visit 4, 35 subjects with residual AKs in the treatment zone chose a further course of treatment with cryotherapy followed 2 weeks later by imiquimod twice weekly for 8 weeks (16 subjects from the imiquimod treatment arm and 19 subjects treated with vehicle). Ten subjects without residual AKs (7 subjects from the imiquimod treatment arm and 3 subjects treated with vehicle) were entered into the observation arm for re-evaluation at weeks 34 (visit 5) and 62 (visit 6). Eighteen subjects with residual AKs declined open-label treatment and were allocated into the observation arm (8 subjects from the imiquimod treatment arm and 10 subjects treated with vehicle).
The long-term efficacy (at week 62) of a single course of imiquimod twice weekly for 8 weeks as an adjunct to cryotherapy alone was evaluated by comparing the outcomes of the cohort pair who had no residual AKs at week 22 and those with residual AKs who declined open-label treatment (Table 2). In the former pair, subjects treated with imiquimod had fewer target and total AKs. The difference in the target AKs was significant (p = .023). A higher proportion of subjects from the imiquimod group achieved complete clearance (71.4%) compared with vehicle (33.3%); however, this difference was not significant (p = .261). In the pair with residual AKs declining further treatment, efficacy outcomes were not significantly different between the imiquimod and vehicle groups.
Actinic Keratosis Counts at the End of Study for Subject Groups Treated with Only One Course of Cryoimmunotherapy

AK = actinic keratosis; Cryo = cryotherapy; Imiq = imiquimod. Values are mean (SD).
For the cohort pair with residual AKs at week 22 proceeding onto open-label treatment with cryotherapy and imiquimod (Table 3), subjects treated with two courses of cryotherapy and imiquimod demonstrated significantly lower subclinical (p = 0.039) and total (p = .015) AK counts and a higher proportion of complete clearance (60% vs 10.5%; p = .003) than those receiving two courses of cryotherapy but only one course of imiquimod.
Actinic Keratosis Counts at the End of the Study for the Cohort Pair Treated in the Open-Label Phase
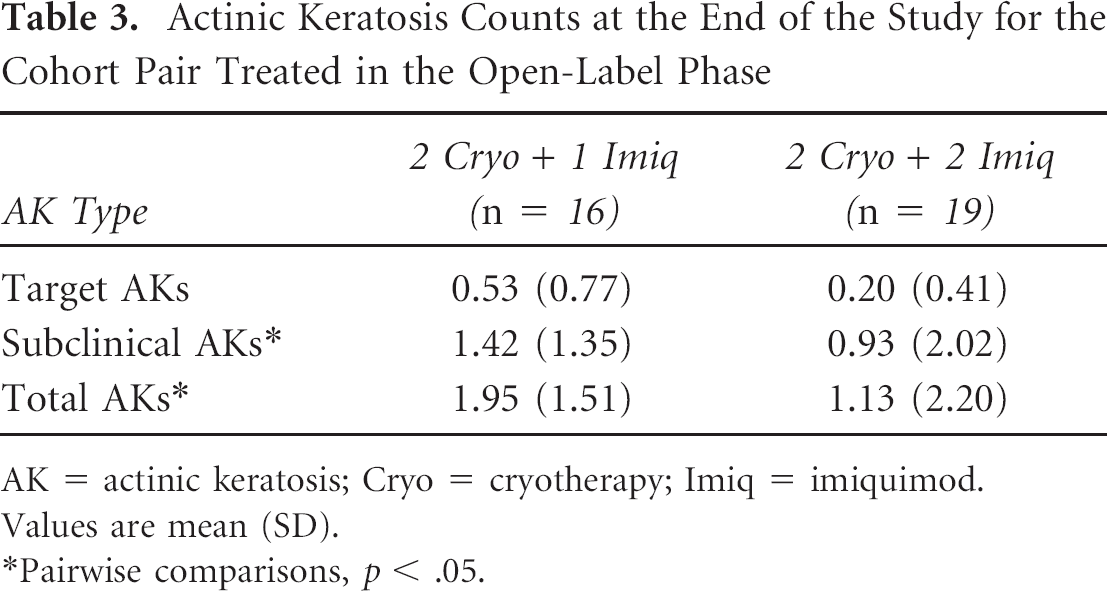
AK = actinic keratosis; Cryo = cryotherapy; Imiq = imiquimod. Values are mean (SD).
Pairwise comparisons, p < .05.
Local irritation attributed to the study drug was reported in 10 subjects (6 for imiquimod, 4 for vehicle). Resolution was reported in all cases, and none were discontinued owing to this adverse event. One case of local skin infection, attributed to cryotherapy, was reported and resolved with topical antibiotic therapy. One case of conjunctivitis was considered by the investigator to be possibly related to the study drug (imiquimod). One serious adverse event was reported (death owing to cardiac disorder), considered to be unrelated to study treatments.
Discussion
Although the efficacy of imiquimod as monotherapy in the treatment of actinic keratoses is well documented in phase III trials,5,6 the role of this agent in routine dermatologic practice is less clearly defined. Given that cryotherapy is considered to be the standard of care for AKs, 3 we designed this study to simulate clinical practice by incorporating the use of imiquimod as an adjunct to cryotherapy. The rationale for this approach is based on visually directed destruction of clinically apparent AKs with cryotherapy followed by field treatment with imiquimod to treat subclinical lesions. The uncovering and eradication of subclinical AKs with imiquimod have been observed in studies using this agent as monotherapy5–7 and are in keeping with its immunologic mechanism of action. This approach incorporates the concept of field cancerization for epithelial cancers whereby chronic ultraviolet exposure induces mutations in proto-oncogenes, leading to the development of an expanding preneoplastic field. The clinical consequence of this concept implies that diagnosis and treatment of epithelial cancers should be focused not only on the tumor but also on the field from which it arose.
The initial double-blind phase of our study demonstrated that cryotherapy alone was effective in clearing 76% of target AKs at 6 months. This outcome is identical to the 76% clearance rate with cryotherapy reported in a randomized, half-face study of 119 subjects with AKs of the face or scalp comparing treatment with topical methyl aminolevulinate–photodynamic therapy against double freeze-thaw cryotherapy. 8 A previous randomized controlled trial using cryotherapy reported a lower clearance rate (46%) at 6 months. 9 The discrepancy between these results may be due to our differentiating between target (identified at baseline) and subclinical (those that developed during the course of the study) AKs. Our target clearance rate is also higher than that of a prospective study of a single liquid nitrogen freeze-thaw cycle for treatment of AKs in which a clearance rate of 67.2% at 3 months was reported. In that study, complete response rates varied with freeze times: 39% for times less than 5 seconds, 69% for freeze times greater than 5 seconds, and 83% for freeze times greater than 20 seconds. 10 The difference in response may be due to methodologic differences as we established the start of the 3- to 5-second freeze cycle from the time of complete ice ball formation of the entire AK.
Although no significant advantage to clearance of target AKs with adjunctive use of imiquimod was observed, the latter did result in an increase in subclinical AKs within the first 3 weeks of treatment, with a subsequent progressive reduction thereafter. In contrast, subjects treated with cryotherapy alone demonstrated a progressive increase in subclinical AKs during this period (see Figure 2B). This discordance in subclinical AK development between imiquimod- and vehicle-treated cohorts is compatible with the field cancerization concept and the role of imiquimod in ameliorating subclinical emerging AKs. This effect was also manifested by a higher proportion of subjects treated with adjunctive imiquimod achieving clearance (58.1%) of subclinical AKs compared with vehicle (34.4%). Although the difference was just beyond the threshold for significance (p = .059), this finding may be particularly relevant as this pilot study was not adequately powered for statistical significance. Previous studies have also demonstrated an increase in AKs during imiquimod treatment and subsequent decline, representing uncovering and eradication of incipient or subclinical lesions.5–7 However, those studies did not use a lesion map at baseline to differentiate target from subclinical AKs—a tool that enabled us to differentiate the effects of cryotherapy on target lesions and the subsequent effect of imiquimod on target and subclinical AKs.
The complete AK clearance rate of 23% after one course of imiquimod in our study was less than that observed in previous studies of imiquimod alone in which rates of 45 to 48% were reported.5,6 These differences are likely due to the longer duration and higher frequency of application in those studies in which 16 weeks of thrice- or twice-weekly applications was used. In our study, a shorter duration and frequency of treatment with imiquimod (twice weekly for 8 weeks) were selected to increase patient tolerance and acceptability.
We explored the long-term efficacy with one course of cryoimmunotherapy by comparison of cohort pairs who did not receive additional therapy beyond the double-blind phase. For those presenting without AKs at 3 months, a single course of adjunctive imiquimod resulted in significantly fewer target and total AKs at the 1-year follow-up. Furthermore, 71% of these subjects maintained complete clearance 1 year after initial treatment. These results compare favorably with a complete clearance rate of 76% at 1 year reported in a small study of 25 patients in which imiquimod was initially applied three times/week for 12 weeks. 11 Our findings are also in agreement with a larger cohort study of 146 patients from phase III trials who were completely clear of AKs at 8 weeks post-imiquimod and followed for up to 16 months. Complete clearance rates of 75% and 57% were observed for subjects treated for 16 weeks with imiquimod thrice and twice weekly, respectively. 12 The higher rate of complete clearance in our study, despite the shorter duration of imiquimod therapy, may be due to the additional effect of cryotherapy on target lesions.
In this study, we were also able to explore the effect of a second course of imiquimod as subjects with residual AKs were offered optional open-label treatment. An additional course resulted in significant improvement in subclinical and total AK counts and a higher proportion of subjects achieving complete clearance (60%). These findings are in agreement with those of an open-label study using cyclical therapy (imiquimod thrice weekly for 4 weeks followed by a 4-week rest period, to a maximum of three cycles) in which rates of complete clearance were 46% after one cycle and 82% after two cycles. 7
The limitations of our study include inadequate power for statistical significance in the randomized double-blind phase and a subsequent optional open-label phase that was neither randomized nor blinded. However, we did maintain blinding of the initial phase of the study until the end of the study. Our findings should be considered preliminary and will require larger adequately powered randomized controlled trials for confirmation.