
Abstract
Background:
Alefacept blocks T-cell activation and induces apoptosis of memory T cells. It improves psoriasis vulgaris and may induce prolonged remissions. Experience with alefacept in palmar plantar pustulosis (PPP) is limited.
Objective:
The objective of the study was to observe the effectiveness and safety of alefacept in the treatment of PPP.
Methods:
Alefacept was administered weekly for 16 weeks by intramuscular (IM) injection of 15 mg to 15 patients with moderate to very severe PPP. Patients were followed for an additional 12 weeks.
Results:
Four weeks after 16 weeks of treatment, there was a 49.6% reduction in the Palmoplantar Pustulosis Psoriasis Area and Severity Index (PPPASI) and a 38.6% and a 64.5% reduction in total and fresh pustules, respectively. Eight weeks after dosing, 53.3% achieved PPPASI 50, 26.7% achieved PPPASI 75, and one patient was clear. The mean percent reduction in total pustules and fresh pustules was 46.1% and 61.2%, respectively; 73% had no pain, 53% had no itching, and 80% had no functional impairment. The palms responded better than the soles.
Conclusions:
This pilot showed that 16 weeks of once-weekly alefacept 15 mg IM was safe, led to improvement in PPP in all 15 treated patients, and induced a remission in one patient. Larger double-blind studies are warranted.
PALMAR PLANTAR PUSTULOSIS is a chronic, disabling, recalcitrant skin condition that affects approximately 0.05% of the population. 1 It is more common in women than in men and in smokers than in nonsmokers. Its onset is typically between ages 40 and 60 years. 2 Clinically, it is manifested as erythema, scaling (often with fissures), and sterile pustules on the palms and soles. Fresh pustules that are yellow to white become brown, dry up, and peel off. The associated burning, itching, and cutaneous changes can cause significant morbidity and functional impairment. Some clinicians view palmar plantar pustulosis (PPP) as a variant of pustular psoriasis. Up to 24.4% of patients have psoriasis vulgaris elsewhere on the body, and there is also a strong association with psoriasis in first-degree relatives. 3
PPP is often refractory to treatment. In those who respond, it frequently relapses shortly after treatment is discontinued. Potent topical corticosteroid and calcipotriol are often the initial treatments, but topical treatment is often not sufficient. 4 Acitretin, methotrexate, cyclosporine, and psoralen ultraviolet A (PUVA) have been used 4 ; however, their toxicities limit their long-term use as therapeutic agents.
PPP is characterized histopathologically by intraepidermal pustules containing neutrophils, 2 intercellular expression of interleukin-8 in the epidermis, 5 and lymphocyte infiltration in the papillary dermis, particularly below pustules. 2 This suggests a role for the lymphocyte-dependent immune response in the pathogenesis.
The interaction of lymphocyte function–associated molecule 3 (LFA-3) with CD2 plays a significant role in T-lymphocyte activation. Memory T lymphocytes have higher CD2 surface expression levels than naive T cells. 6 Alefacept blocks the LFA-3–CD2 interaction both in vitro and in vivo, resulting in interference with T-lymphocyte activation. Alefacept has been shown to improve psoriasis vulgaris and induce prolonged remissions. 7
There is limited experience with the use of alefacept in PPP. Given that alefacept is useful for psoriasis vulgaris and may induce prolonged remissions, it might be a useful therapeutic agent for PPP, a chronic, disabling, refractory condition that usually quickly relapses on cessation of therapy. This pilot trial was conducted to provide additional information concerning the use of alefacept in PPP.
Methods
This was a single-center, open-label study in which alefacept was administered 15 mg intramuscularly weekly for 16 weeks to 15 patients with moderate to very severe PPP. Patients were given the option of home injection on alternate weeks and were followed for 12 weeks after dosing. Ethics approval was obtained prior to study commencement. Efficacy assessments included the Palmoplantar Pustulosis Psoriasis Area and Severity Index (PPPASI), Physician Global Assessment, and total and fresh pustule counts. The PPPASI is a scoring system similar to the Psoriasis Area and Severity Index (PASI) except that total pustules are assessed in lieu of thickness. 8 Erythema, scaling, and total pustules are assessed on a 0- to 4-point scale and area on a 0- to 6-point scale. Each palm contributes 20% of the total and each sole 30%. In common with the PASI, the maximum PPPASI score is 72. A subanalysis of the PPPASI for patients who had baseline palm involvement was done using the same formula, with the exception that each palm contributed to 50% of the total and the soles 0%. Similarly, a PPPASI subanalysis for soles was undertaken with each sole contributing 50% to the total and the palms 0%. Patients assessed pain, itching, and functional impairment compared with baseline. Safety assessments included a review of adverse events, serious adverse events, and CD4 counts.
Inclusion criteria included males and nonpregnant, nonlactating females using adequate contraception, at least 18 years of age, with stable, moderate, severe, or very severe PPP and a minimum of three pustules on one sole or palm. Patients were required to give written informed consent and be in general good health, with no other skin disease, disease state, or physical condition that would impair evaluation of PPP or that would increase their health risk by participation in the study. Exclusion criteria included previous treatment with alefacept, allergy to alefacept or any components of the study medication, known malignancy within 5 years (except adequately treated basal cell carcinoma or in situ squamous cell carcinoma of skin), serious local or systemic infection within 3 months, known human immunodeficiency virus (HIV), hepatitis B or hepatitis C seropositivity, tuberculosis, CD4 count less than the lower limit of normal, significant abnormal blood chemistry, or participation in another clinical trial within 28 days. Required washouts were 1 week for topicals, 2 weeks for ultraviolet B phototherapy, and 4 weeks for PUVA, oral steroids, retinoids, immunosuppressants, and biologics.
Results
Fifteen of the 16 patients who gave consent and were screened were treated with alefacept. One patient was not treated as she did not meet the inclusion criteria. Eighty percent were female, with an average age of 54 years. All but one patient had a history of smoking, with 53% still smoking at the time of screening. Thyroid disease was present in 26.6%; 20% had a history of psoriasis vulgaris. The mean duration of PPP was 7.5 years. Sixty percent of patients had PPP on the palms and soles, 33% on the soles alone, and 7% on the palms alone. All patients had been previously treated with topical agents (eg, topical steroids, calcipotriol, betamethasone diproprionate and calcipotriol hydrate [Dovobet], tazarotene, tars, and/or anthralin), two with ultraviolet B phototherapy, two with PUVA, three with methotrexate, and one with prednisone. None of the patients had been previously treated with biologics. The mean baseline PPPASI was 13.89, the mean total number of pustules was 191.7, and the mean number of fresh pustules was 58.7. Four patients (26.7%) chose to self-inject at home. Fourteen of the 15 patients completed the 16-week dosing period and 13 of the 14 completed the 12-week follow-up phase. One patient terminated the study at week 10 owing to dermatitis, which was thought to be possibly related to study medication. The data values from this patient's last visit were carried forward to the end of the study for analysis purposes.
Four weeks after 16 weeks of treatment, there was a 49.6% reduction in the PPPASI (Figure 1), a 38.6% reduction in total pustules (Figure 2), and a 64.5% reduction in fresh pustules (Figure 3). The palms responded better than the soles, with a reduction in PPPASI of 66.6% 4 weeks after dosing and 74.4% 8 weeks after dosing. PPPASI 50 was obtained by 53.3% and PPPASI 75 by 26.7% 8 weeks after dosing (Table 1). One patient had clearing of his PPP and psoriasis vulgaris at week 15 and remained clear during the 12-week follow-up period. Eight weeks after dosing, the mean percent reduction in total pustules and fresh pustules was 46.1% and 61.2%, respectively; 26.7% had no pustules (see Table 1), 46.7% no fresh pustules (see Table 1), 73% no pain, 53% no itching, and 80% no functional impairment.
Percentage of Patients with Palmoplantar Pustulosis Psoriasis Area and Severity Index 50 and 75, No Pustules, and No Fresh Pustules
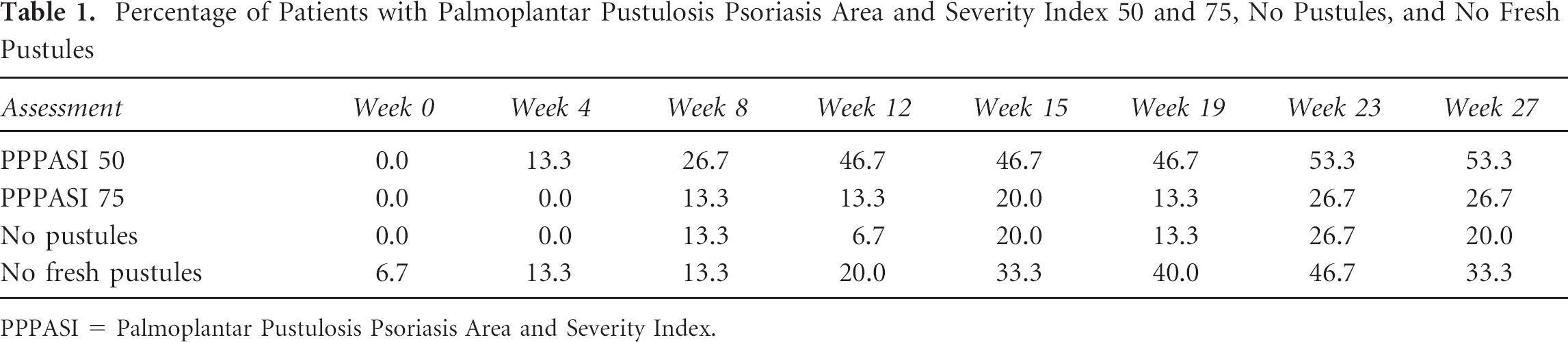
PPPASI = Palmoplantar Pustulosis Psoriasis Area and Severity Index.
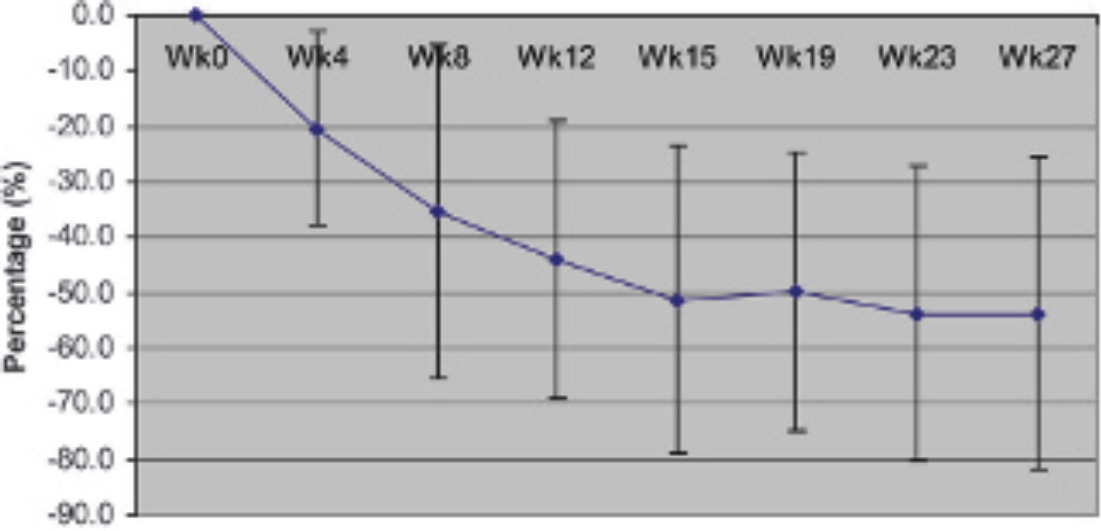
Mean percent change in Palmoplantar Pustulosis Psoriasis Area and Severity Index from baseline.
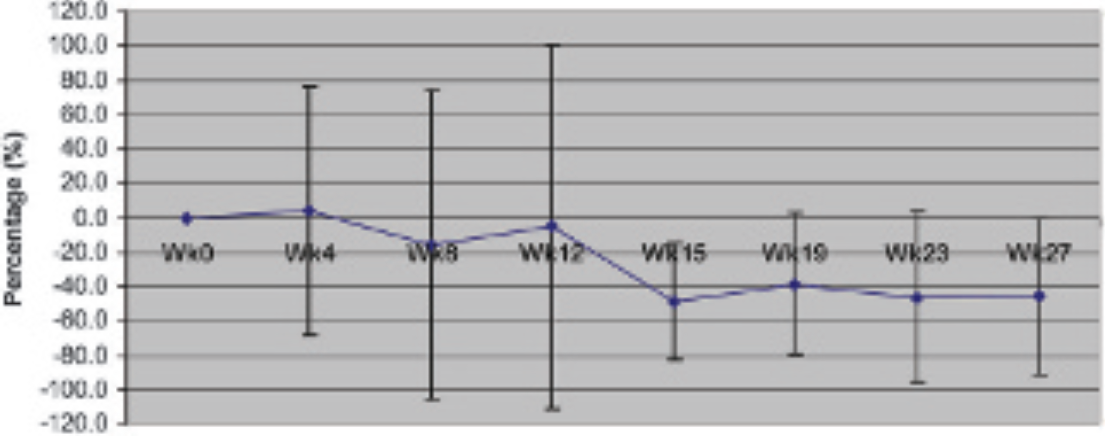
Mean percent change in total pustules from baseline.
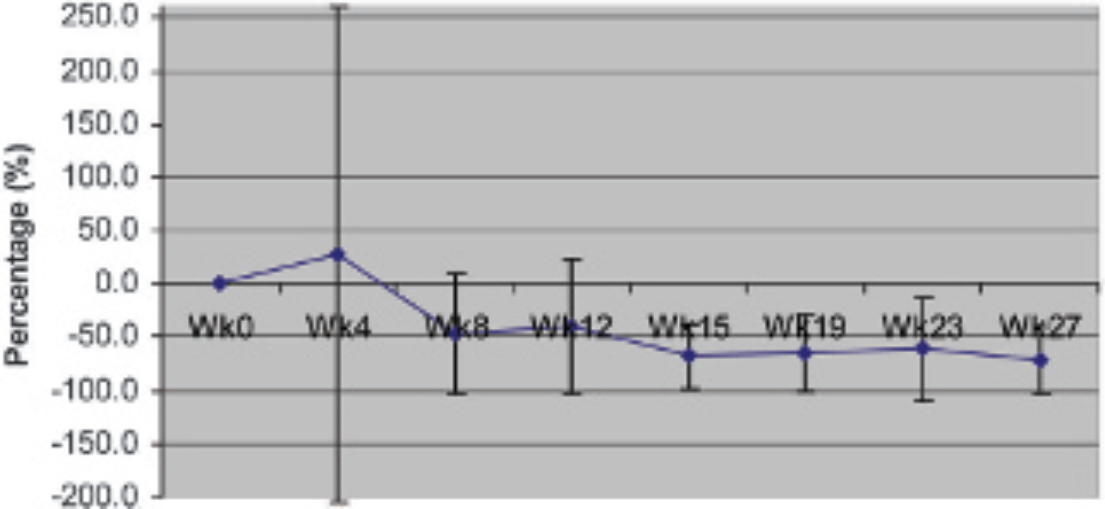
Mean percent change in fresh pustules.
Adverse events attributed to alefacept included two injection-site reactions (one mild bruise after week 12 office injection, one mild erythema and induration after week 9 home injection), mild headaches (n = 1), and severe and moderate dermatitis (n = 1 each), which flared after injection but may have been induced by soap. Infections included six episodes of mild to moderate upper respiratory tract infection in five patients, two cases of mild pharyngitis, one case of mild sinusitis, and one wart. There were no opportunistic infections or serious adverse events. All patients maintained their CD4 count over 250 cells/mm3.
Discussion
There are limited data on the use of biologics in the treatment of nonplaque variants of psoriasis, including PPP. There is one reported case of dramatic improvement of PPP in one patient treated with alefacept 9 and a couple of reports of two to three cases treated successfully with efalizumab.10,11 The current study involving 15 patients appears to be the largest reported case series to date. Sixteen weeks of treatment was chosen since in psoriasis vulgaris, 16 weeks appears to be superior to the currently approved 12-week dosing period. 12 In common with studies in psoriasis vulgaris, maximal improvement was noted after discontinuation of alefacept. 7 In the current trial, maximal improvement was noted 8 to 16 weeks after dosing. In contrast to plaque psoriasis, in which it has been my experience that a subset of patients do not appear to respond to alefacept, all patients in this PPP study had improvement, although only one patient (who also had clearing of his plaque psoriasis) had complete clearing. Given that PPP appears to be phenotypically and genetically distinct from psoriasis vulgaris, it is not surprising that the response to treatment might be different. Psoriasis vulgaris and guttate psoriasis have been strongly linked to human leukocyte antigen (HLA)-Cw6, single nucleotide polymorphism (SNP)-7, and SNP-9, whereas such an association has not been found for PPP. 13 The strong association of plaque psoriasis and PPP suggests that these two conditions may share common, yet to be discovered pathogenetic features regulating disease expression. No safety concerns appeared in this pilot study. Larger placebo-controlled studies are warranted.