
Abstract
Background:
Drug use patterns and serious bloodborne infections commonly have dermatologic manifestations among illicit injection-drug users (IDUs).
Objective:
To assess how self-reported skin conditions of IDUs may correlate with underlying infectious diseases after adjustment for drug use patterns.
Methods:
Prospective analysis of factors associated with self-reports of skin rashes, cellulitis, oral lesions, and lymphadenopathy obtained from 1,065 IDUs enrolled in a large cohort study. Variables potentially associated with each outcome were evaluated using multivariate generalized estimating equations.
Results:
In multivariate analyses, drug use patterns were associated with cellulitis, whereas human immunodeficiency virus (HIV) infection and hepatitis C (HCV) were not. HCV infection was independently associated with skin rashes (odds ratio [OR] 1.85; 95% Cl 1.17–2.94). HIV infection was independently associated with lymphadenopathy (OR 2.00; 95% CI 1.52–2.63), skin rash (OR 2.12; 95% CI 1.57–2.86), and oral lesions (OR 14.95; 95% CI 9.41–23.76).
Conclusions:
Self-reports of IDUs, which could easily be obtained as part of a functional inquiry in a clinical setting, correlate with specific drug use patterns and underlying bloodborne infections.
ILLICIT INJECTION-DRUG USE is associated with a wide array of health and social problems.1,2 Among the largest concerns is human immunodeficiency virus (HIV) infection, which creates a number of public health challenges since injection-drug users (IDUs) are commonly unaware of their HIV status. 3 This has implications for HIV transmission behaviors (eg, used syringe lending) but also for HIV treatment efficacy, with recent studies showing that the effectiveness of antiretroviral therapy is severely limited when introduced late in the course of HIV infection.4,5 An additional concern is hepatitis C virus (HCV) infection, which, owing to its greater infectiousness than HIV, is much more prevalent in IDUs.6,7
The above chronic bloodborne infections may periodically manifest with dermatologic conditions that may provide the only indication of the presence of bloodborne infection. For instance, HCV infection has been shown to be most closely associated with porphyria cutanea tarda, lichen planus, lymphocytic sialadenitis, and polyarteritis nodosa.8,9 Of the diverse viral, bacterial, fungal, and noninfectious cutaneous findings in HIV, several are almost exclusively seen in HIV-infected individuals, including Kaposi sarcoma, bacillary angiomatosis, and oral hairy leukoplakia.10–12 However, cutaneous manifestations are often transient and may not be present during the clinical encounter.8–12 Furthermore, IDUs may have only transitory contact with the health care system.13–15
A further challenge to the clinician is the fact that IDUs commonly display cutaneous stigmata of drug use that are totally independent of bloodborne infections.16,–18 The general practitioner may have difficulty distinguishing signs of systemic infection from these stigmata or may presume that all cutaneous findings are simply consistent with illicit drug injection.
Unfortunately, to date, little has been done to determine the independent effect of drug use behaviors and underlying infections on common dermatologic conditions in illicit drug users. Given that dermatologic conditions are commonly only transient,8–12 an advantage of obtaining self-reports of active or recent skin conditions may be an increased likelihood of diagnosing an underlying infection. Therefore, the present study was undertaken to evaluate how self-reported recent dermatologic conditions, obtained during a standardized functional inquiry, were associated with underlying infectious diseases independent of drug use and related behaviors. 19
Methods
Beginning in December 1, 2003, IDUs were randomly recruited to participate in a prospective cohort study called Scientific Evaluation of Supervised Injecting (SEOSI), which has been described in detail previously.20,21 Briefly, the SEOSI cohort is based on a random sample of IDUs recruited from within a harm reduction program in Vancouver, British Columbia. Random recruitment involves using random number generation to select blocks of time during the hours that the program is open (between 10:00 am and 4:00 am). During these times, users of the program are invited to enrol in the SEOSI study, and a nominal financial incentive ($20 CDN) is offered. Among individuals who wish to enrol, and provide informed consent, a venous blood sample is drawn for HIV and HCV serology, and individuals are asked at baseline if they are aware of their HIV and HCV status. Pre- and post-test counseling is provided as part of the study. In addition, a detailed interviewer-administered questionnaire is conducted to determine drug use and related behaviors. The SEOSI cohort has been ethically approved by the University of British Columbia/ Providence Healthcare Research Ethics Board.
In the present study, we sought to determine how self-reports of common skin conditions were associated with illicit drug use behaviors as well as HIV and HCV serostatus. We used language that was accessible to IDUs, and the questionnaire queried for any reports of rashes, cellulitis, white patches in the mouth, and swollen lymph nodes in the 6 months prior to the interview. Interviewers were trained to explain these terms if an IDU reported or appeared not to understand. In each case, we fit separate statistical models to determine factors independently associated with each of the above four outcomes during semiannual interviews conducted during the period between December 1, 2003, and November 30, 2005.
Given that analyses of factors associated with each outcome (cellulitis, white patches in the mouth, rash, and swollen glands) within the last 6 months included serial measures for each subject, we used generalized estimating equations for binary outcomes with logit link for the analysis of correlated data to determine which factors were independently associated with the relevant outcome for each model. These methods provided standard errors adjusted by multiple observations per person using an exchangeable correlation structure.
Variables considered in each of the four analyses included gender, age (per 10 years older), ethnicity (Aboriginal vs other), hepatitis C positivity (yes vs no), HIV positivity (yes vs no), daily crack smoking (yes vs no), daily cocaine injection (yes vs no), daily heroin injection (yes vs no), daily methamphetamine use (yes vs no), and involvement in the sex trade (yes vs no). Unless otherwise noted, all behaviors refer to activities in the previous 6 months and all variable definitions have been used extensively and were identical to earlier reports.20,21
The multivariate model for each outcome was fit using the a priori defined model-building protocol of adjusting for all variables that were statistically significant at the p < .05 level in bivariate analyses, and all univariately significant variables are shown in the tables. All statistical analyses were performed using SAS software version 8.0 (SAS, Cary, NC). All p values are two sided.
Results
Between December 1, 2003, and November 30, 2005, 1,065 IDUs were enrolled into the SEOSI cohort. Overall, the median age was 38.5 (interquartile range [IQR] 32.7–44.3), 312 were women, and 206 were Aboriginal. The median number of follow-up visits during the study period was 1 (IQR 1–2).
The multivariate analysis of factors associated with cellulitis is shown in Table 1. As shown here, factors independently associated with cellulitis included daily cocaine injection (odds ratio [OR] 1.43; 95% confidence interval [CI] 1.10–1.85), daily heroin injection (OR 1.29; 95% CI 1.01–1.64), daily methamphetamine injection (OR 2.32; 95% CI 1.34–4.00), and daily crack cocaine smoking (OR 1.34; 95% CI 1.03–1.72). Gender, sex trade involvement, age, ethnicity, HCV positivity, and HIV positivity were not found to be associated with cellulitis at the p < .05 level.
Multivariate Generalized Estimating Equation Analysis of Factors Associated with Cellulitis in the Last 6 Months
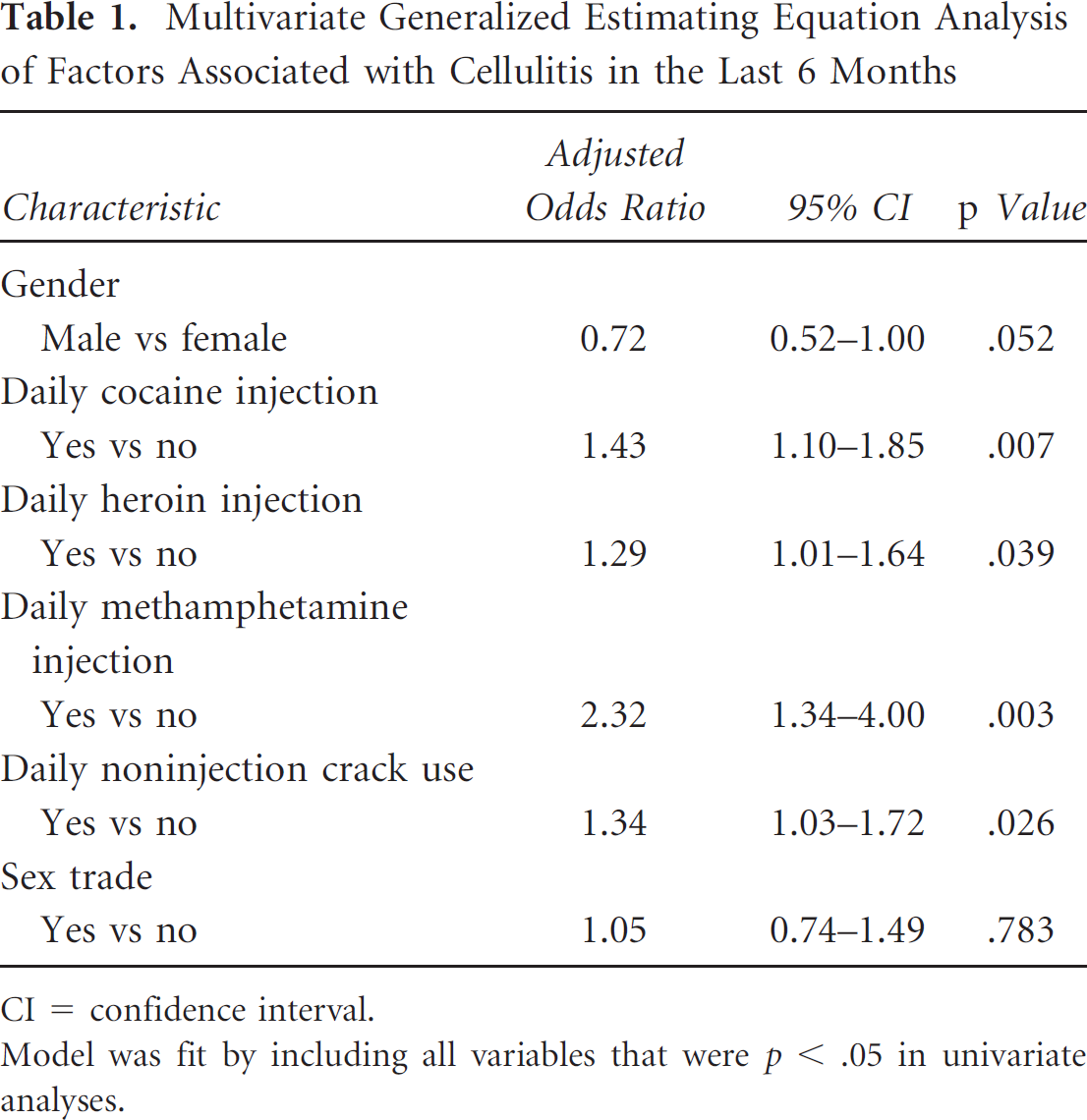
CI = confidence interval.
Model was fit by including all variables that were p < .05 in univariate analyses.
The multivariate analysis of factors independently associated with lymphadenopathy is shown in Table 2. As shown here, these factors included an inverse association with male gender (OR 0.61; 95% CI 0.46–0.82) and positive associations with HIV positivity (OR 2.00; 95% CI 1.52–2.63), daily cocaine injection (OR 1.50; 95% CI 1.20–1.87), and history of sex trade involvement (OR 1.40; 95% CI 1.04–1.90). Age, ethnicity, HCV positivity, daily crack smoking, daily heroin injection, and daily methamphetamine use were not found to be associated with lymphadenopathy at the p < .05 level.
Multivariate Generalized Estimating Equation Analysis of Factors Associated with Swollen Glands in the Last 6 Months
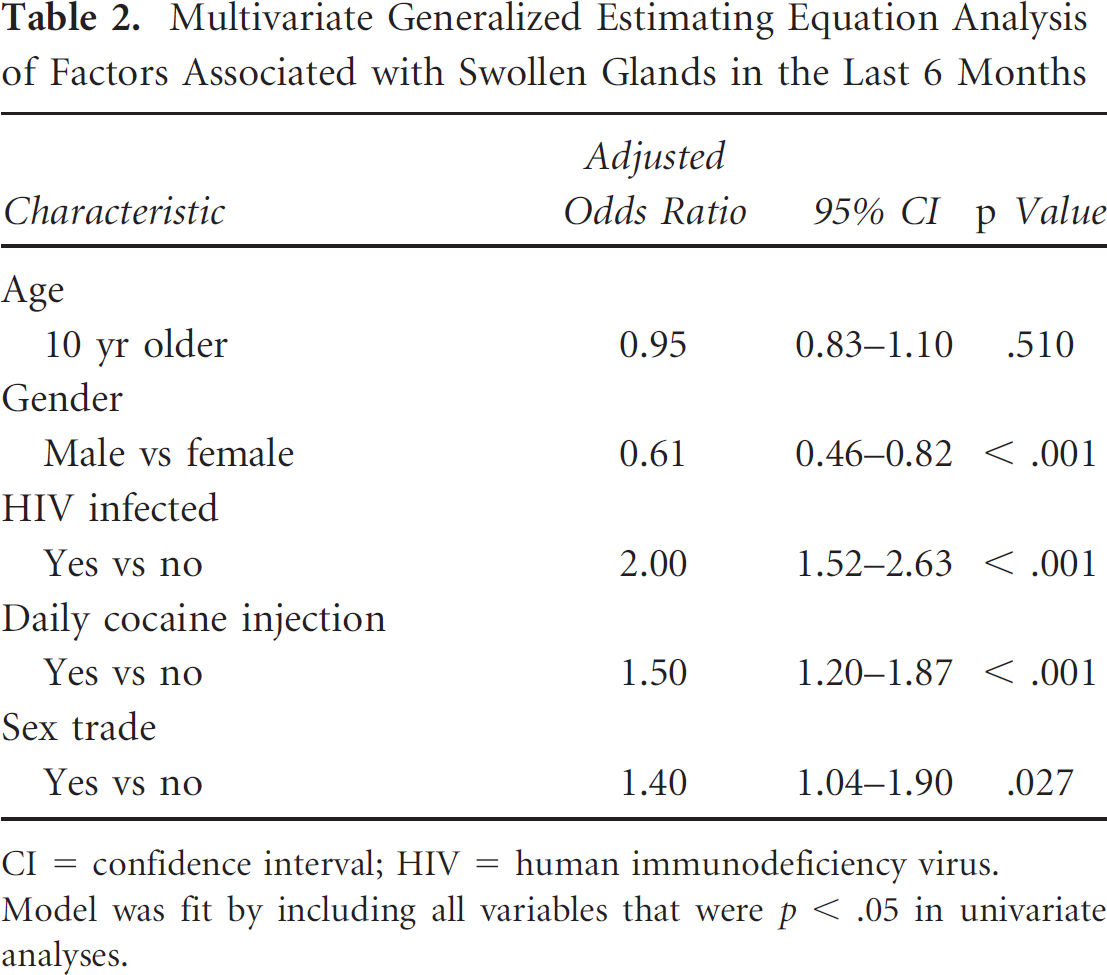
CI = confidence interval;
HIV = human immunodeficiency virus.
Model was fit by including all variables that were p < .05 in univariate analyses.
The multivariate analysis of factors associated with skin rashes in the last 6 months is shown in Table 3. As shown here, factors associated included HIV positivity (OR 2.12; 95% CI 1.57–2.86), HCV positivity (OR 1.85; 95% CI 1.17–2.94), and history of involvement in the sex trade during the last 6 months (OR 1.66; 95% CI 1.17–2.35). Gender, age, ethnicity, daily crack smoking, daily cocaine injection, daily heroin injection, and daily methamphetamine use were not associated with skin rashes at the p < .05 level.
Multivariate Generalized Estimating Equation Analysis of Factors Associated with Rash in the Last 6 Months
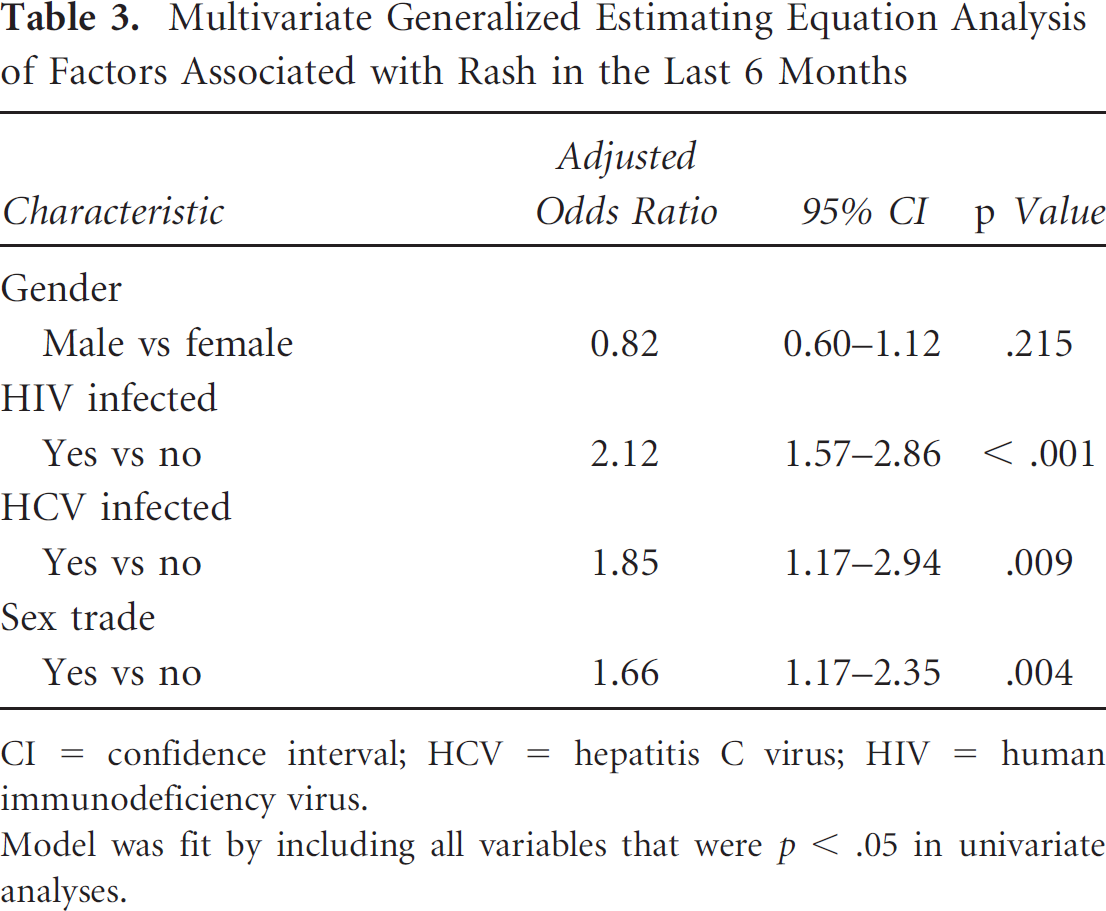
CI = confidence interval;
HCV = hepatitis C virus;
HIV = human immunodeficiency virus.
Model was fit by including all variables that were p < .05 in univariate analyses.
The multivariate analysis of factors associated with white patches in the mouth in the last 6 months is shown in Table 4. As shown here, the factors associated with white patches in the mouth included HIV positivity (OR 14.95; 95% CI 9.41–23.76) and an inverse association with male gender (OR 0.52; 95% CI 0.32–0.83). Age, ethnicity, HCV positivity, daily crack smoking, daily cocaine injection, daily heroin injection, daily methamphetamine use, and sex trade involvement were not associated with this outcome at the p < .05 level.
Multivariate Generalized Estimating Equation Analysis of Factors Associated with White Patches in Mouth in the Last 6 Months
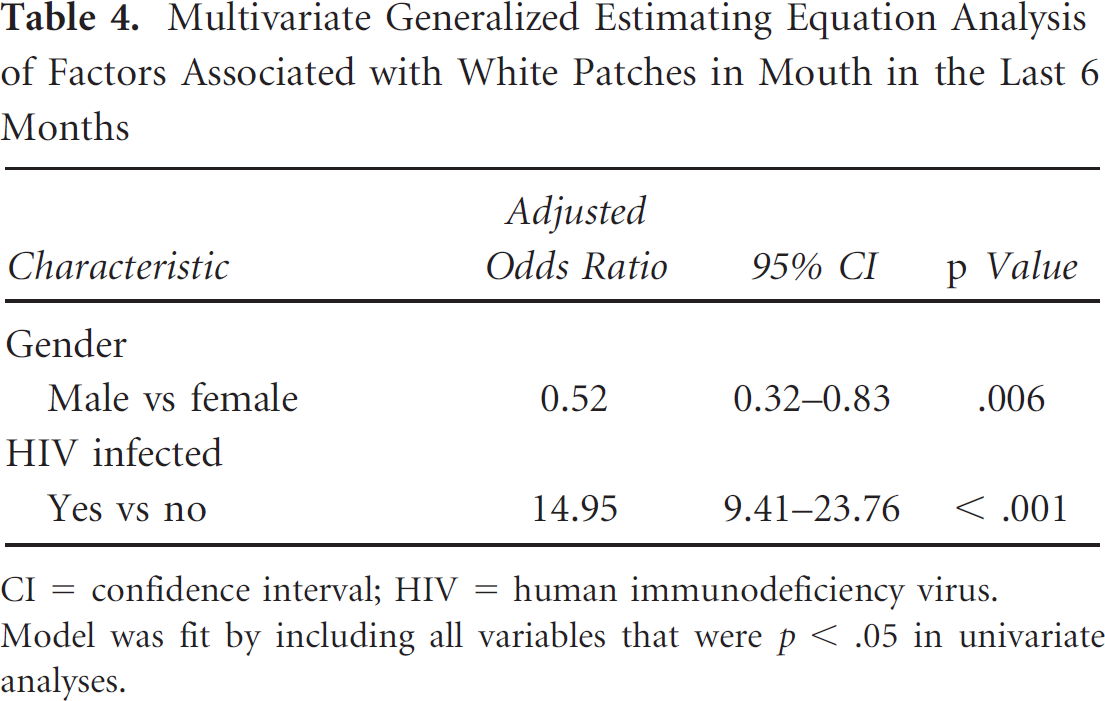
CI = confidence interval;
HIV = human immunodeficiency virus.
Model was fit by including all variables that were p < .05 in univariate analyses.
In an effort to examine the utility of the above findings, we evaluated the number of participants who were unaware of their HCV or HIV infection status on recruitment into the study and the number of these individuals who reported one of the dermatologic conditions that was independently associated with these infections. Interestingly, among the 108 individuals who were unaware of their HCV infection, 15 (13.9%) reported a skin rash in the previous 6 months. Among the 17 individuals who were unaware of their HIV infection, 5 (29.4%) reported at least one of the dermatologic conditions that was independently associated with HIV infection.
Discussion
The present study demonstrates how illicit drug use behaviors and HCV and HIV infection may be associated with common dermatologic conditions observed among a large cohort of IDUs. Interestingly, neither HIV nor HCV was independently associated with cellulitis. However, among individuals who reported lymphadenopathy or skin rash, the likelihood of underlying HIV infection was approximately twofold in multivariate analysis and underlying HIV infection was almost 15 times more likely among individuals who reported white patches in the mouth in the previous 6 months. HCV was independently associated with skin rashes only.
We demonstrate that specific drug use patterns are independently associated with cellulitis, whereas HIV and HCV are not more common among IDUs presenting with this condition. In fact, a small study of community-recruited IDUs in San Francisco identified 54 of the 169 IDUs investigated as having cutaneous infections and that frequent unsafe injection practices were the strongest predictor of these infections. A further 115 of the 169 IDUs involved (68%) reported having cutaneous injection-site infections in the past. Unfortunately, this earlier study did not investigate the role of underlying HIV or HCV infection. Although an association between lymphocytic sialadenitis and HCV has been shown previously, in the current study, HCV patients did not report an increased incidence of swollen glands. This may be due to the low rate of HCV seroconversion among this population and the fact that the majority of individuals have been infected for many years. 22 Overall, with the exception of cellulitis, HIV infection was much more strongly associated with the dermatologic conditions we examined than was HCV infection.
The present study also demonstrates the utility of including any instance of dermatologic conditions in the recent past (eg, last 6 months) in the medical interview of an IDU. For instance, even after adjustment for all relevant demographics and drug use behaviors, reporting white patches in the mouth was associated with an almost 15-fold greater chance of being HIV infected. The association between leukoplakia and HIV infection is well recognized in the literature, with many studies having identified oral hairy leukoplakia and, to a lesser extent, oral candidiasis as being suggestive of underlying HIV infection. It is noteworthy that the questions used in the present study could have been used to identify 14% of individuals who were unaware of their HCV infection and 29% of individuals who were unaware of their HIV infection. By including such simple questioning as part of the initial functional inquiry, physicians in contact with IDUs should be prompted to suspect HCV or HIV infection based on a positive response. Knowledge of the association between the dermatologic conditions investigated in this study and HCV and HIV infection should be helpful to all physicians involved in the care of IDUs, especially considering that the ability of nonspecialist physicians to recognize the physical findings associated with these infections is limited. In a study that assessed the ability of primary care physicians to recognize skin conditions associated with HIV, only 22 of 97 (23%) and 23 of 89 (26%) physicians involved were able to correctly diagnose the findings of oral hairy leukoplakia and Kaposi sarcoma, respectively. 19
The present study has two significant limitations. First, although self-reports of IDUs appear to represent an effective means of obtaining information regarding recent dermatologic afflictions, such retrospective reporting is vulnerable to social desirability and memory biases. 23 However, self-report can be viewed as a strength in the present study given that the questions could be asked by research nurses, and the above biases are likely relevant to any clinical setting. The use of self-report also by necessity results in the use of the large, relatively nonspecific category of “rashes.” We assume that this category includes such diseases as psoriasis and seborrheic dermatitis exacerbated by HIV infection, HIV-associated eosinophilic folliculitis, the exaggerated responses to insect bites and infestations seen in the HIV-infected, staphylococcal folliculitis and extensive molluscum contagiosum associated with immunosuppression, HCV-associated cryoglobulinemic vasculitis, HCV-induced porphyria cutanea tarda, HCV-associated lichen planus, excoriations owing to the pruritus associated with HCV and HIV infections, secondary syphilis, and perhaps Kaposi sarcoma. However, in spite of the nonspecific nature of this category, its self-reported presence remains predictive of HCV or HIV infection in this population. Second, although we undertook extensive efforts to obtain a representative sample, 20 it is not known how generalizable our findings can be to other populations of IDUs. However, it is unlikely that our cohort is so demographically distinct that the safe application of the results of this study to other similar IDU populations would be threatened.
In summary, the present study provides estimates from a large cohort study of IDUs that define the relationship between illicit drug use behaviors, HCV and HIV infection, and common dermatologic conditions. Specifically, self-report of cellulitis demonstrates a relationship to patterns of drug use, but not to underlying HIV or HCV infection, self-report of rashes, white patches in the mouth, or swollen glands, is associated with underlying HIV infection; self-report of rashes is also associated with underlying HCV infection. Our results should be valuable to clinicians who may have frequent contact with illicit drug users and to specialists who may be asked to consult on dermatologic manifestations of disease in these individuals. Given the poor access to health care among IDUs and the clinical and public health implications of untreated and undiagnosed HIV and HCV infection, clinicians must remain vigilant in their efforts to screen for and diagnose these conditions.