
Abstract
Background:
Physicians frequently prescribe short-term corticosteroids (CSs) to treat acute and self-limiting diseases. Standard texts and articles do not usually discuss the possible, although infrequent, risks of short-term CSs.
Objective:
To demonstrate that side effects, although uncommon, can occur with short-term CSs and that these can occasionally be serious.
Methods:
Medline peer review literature in English (1985–2006) was searched to identify the potential risks of CSs. Standard textbooks of dermatology, gastroenterology, ophthalmology, pharmacology, respirology, and rheumatology were reviewed. Because the results showed some factual discordance and a dearth of precise data, the results for each body system were reviewed with two relevant clinical specialists at North York General Hospital (with at least 20 years' experience). Further information was obtained from a questionnaire of 200 physicians in North York General Hospital and by feedback from an additional 100 physicians during a presentation of this material at the American Academy of Dermatology.
Results:
Short-term CSs are generally safe, but there have been numerous reports of associated avascular necrosis and a few cases of fatal varicella-zoster in immunocompetent patients. Severe mood changes and psychotic reactions rarely occur unpredictably with short-term CSs. These events are rare, and most treatments with short-term CSs are problem free.
Conclusions:
Problems are infrequent, but patients must be informed of all material risks and treatment options. Thorough chart documentation is required, and patient consent must be given. CS doses should be as low as possible, and CS courses should be as infrequent and as short as possible. The literature reviewed in this article clearly indicates that a short course of CS of 1 week, in the absence of specific contraindications, is unlikely to be harmful (psychotic or prepsychotic episodes possibly excepted).
SHORT-TERM CORTICOSTEROIDS (CSs) are commonly recommended for the treatment of severe and acute self-limiting inflammatory conditions such as drug reactions, contact dermatitis, severe eczema, severe urticaria, asthma, allergies, bowel disorders, arthritis, and numerous other conditions without concerns being expressed about potentially significant side effects.1–10 Short-term CSs are also used (perhaps ill-advisedly) if a patient is not getting better or if a diagnosis is not precise. By common usage, short-term CS refers to the standard starting dose of 40 to 60 mg of prednisone or equivalent (Table 1), tapered or level, over a few days to 3 weeks. The total cumulative dose is up to 600 mg, with most being 400 mg or less. The minimal amount of systemic CS and duration of administration sufficient to cause problems are not well defined.1–10
Prednisone Dose Equivalents
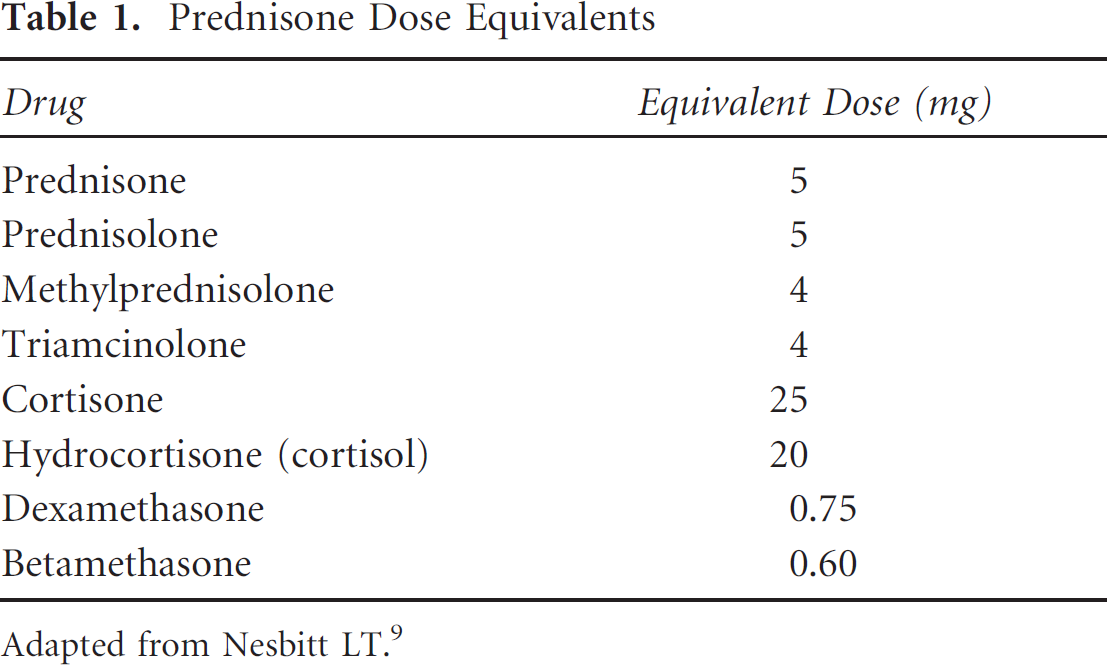
Adapted from Nesbitt LT. 9
CSs affect every body system, and their long-term use is associated with a myriad of well-established side effects.1–10 In contrast, short-term CSs are generally considered to be safe. Nevertheless, serious side effects can occur, and physicians should be aware of the possible medical and legal implications of short-term prednisone (STP).
Methods
Medline peer review literature in English (1985–2006) was searched to identify the potential risks of STP. Standard textbooks of dermatology, gastroenterology, ophthalmology, pharmacology, respirology, and rheumatology were reviewed. Because the results showed some factual discordance and a dearth of precise data, the results for each body system were reviewed with two relevant clinical specialists at North York General Hospital (with at least 20 years' experience). Further information was obtained from a questionnaire of 200 physicians at North York General Hospital and by feedback from an additional 100 physicians during a presentation of this material at the American Academy of Dermatology.
Results
STP is best taken as a single dose with breakfast, and it can be stopped at any time without withdrawal symptoms. 1 Minor infrequent complaints include sleeplessness, mood swings, anxiety, a sense of well-being, a sense of fullness, weight gain, and stomach upset.1–10
Severe mood changes and psychotic reactions rarely occur with STP. Studies suggest that patients receiving daily doses of 40 mg of prednisone or greater are at higher risk for developing problems. Symptoms can occur during the first days of treatment, and the patient's previous mental health is not an accurate predictor. Patients on lower doses have little risk for the development of severe psychiatric illness. Management is usually a reduction in prednisone and treatment with phenothiazines.11–14
STP can raise blood pressure, but this is not ordinarily of clinical significance. Patients with severe cardiac disease and/or heart failure require close monitoring to avoid problems owing to fluid and salt retention. Serum potassium, which can be lowered with STP, should be monitored in patients on digoxin. 15
Sporadic case reports have suggested that oral CS therapy can result in ocular hypertension and open-angle glaucoma, but few studies have considered the effects of oral STP on ocular pressure. Problems with topical steroid “steroid responders” are well documented, but this has not been reported with oral steroids.16,17 There have been no published case reports of glaucoma resulting from STP, but, nevertheless, because of this theoretical possibility, patients with glaucoma should inform their ophthmalogist of their prednisone therapy and receive pressure monitoring if the ophthmalogist deems it relevant. Herpes simplex is known to be aggravated by topical ocular steroids, but this has not been reported with oral STP. Nevertheless, vigilance should be maintained and oral antiviral agents should be considered in relevant patients (no hard data).18,19
CSs can raise blood sugar, and diabetics must monitor their blood sugar and adjust their insulin as required. Experienced diabetics are normally able to make these adjustments themselves. 20
Minor gastrointestinal upset is common with oral CS therapy, but taking the CS concurrently with food can minimize this. There is little evidence that STP has a significant effect on peptic ulcers, and most of the original reported cases were probably due to concomitant non-steroidal anti-inflammatory agents. 21 Hard data are not available, and it is controversial, but if a patient does have a proven history of peptic ulcer and has not been treated for Helicobacter pylori, then, according to two gastrointestinal specialists at North York General Hospital, there is anecdotal evidence that the patient should be protected with a proton pump inhibitor.
Patients who are taking CSs for prolonged periods of time may be at risk for either the acquisition of primary tuberculosis or the reactivation of latent tuberculosis. The specific thresholds of dose and duration for this complication are unknown. Prednisolone given at a dose of more than 15 mg daily for 2 to 4 weeks suppresses tuberculin activity; therefore, theoretically, patients with latent tuberculosis could experience reactivation. 22 If there is any concern of latent tuberculosis, then isoniazid (INH) can be concurrently used. The Mantoux test is not usually required for STP as clinical observation or concomitant INH is more relevant.22,23
Stuck and colleagues examined the association between CS therapy and subsequent infectious disease by pooling data from controlled clinical trials. 24 Their analysis revealed no increased risk of infectious complications in patients given less than a cumulative dose of 700 mg of prednisone. They stated that it would be erroneous to conclude that prescriptions of lower doses of prednisone are absolutely safe because the patients considered were only partly representative of patients treated in clinical practice. The effect of STP therapy on viral, fungal, opportunistic, and parasitic infections is unclear. Numerous case reports, especially of seriously ill patients, recount adverse outcomes, but no increased incidence of these diseases has been reported in larger studies. However, the presentation of infection may be masked by the therapeutic effects of the glucocorticoid. 4 Any sick patients, including patients with human immunodeficiency virus (HIV), should be monitored carefully as opportunistic infections can possibly be more prevalent and severe if associated with concomitant steroids. 5
Disseminated varicella with a sometimes fatal outcome has been reported as a complication of STP.25–27 For several years, it was believed that this increase in morbidity and mortality was a result of immunocompromise secondary to the patient's underlying disease. However, Kasper and Howe reviewed fatal cases of asthma in immunocompetent children on STP who developed varicella and died. 26 They concluded that patients who developed varicella after recent treatment with large doses of CSs should be considered to be at risk of dissemination and recommended that these patients be treated with acyclovir at the onset of the varicella exanthem rather than waiting for signs of dissemination. 26 Benz and colleagues reported two cases of progressive outer retinal necrosis resulting in blindness from varicella-zoster infection occurring in two immunocompetent individuals after treatment with STP for presumed optic neuropathy. 28
There have been occasional reports of seizures (no hard data) occurring in epileptics on STP, so patients should be warned of this possibility and antiepilepsy medication should be carefully monitored and alcohol intake moderated or avoided. 2
Patients with severe hepatic disease are unable to metabolize prednisone; therefore, the active form, prednisolone (which does not require liver metabolism), should be administered. 3
Long-term CS is known to be associated with the development of avascular necrosis (AVN) (synonyms: osteonecrosis, ischemic necrosis, or aseptic necrosis).29–32 A number of authors have also noted the relationship between AVN and short-term CS use,33–35 and McKee and colleagues in 2001 reported 15 cases of AVN following short-term CS therapy, with the lowest cumulative dose being 290 mg. 33 (I spoke with Dr. McKee in December 2006, and they have now seen over 100 cases.) Osteoporosis has not been reported to be a problem with short-term CS, but patients should continue with their normal preventive measures, such as calcium, vitamin D, and bisphosphonates, if relevant.36,37 A search for AVN on the Internet will lead to commercial pages prepared for lawyers outlining the relationship between AVN and CS and giving appropriate references and supplies relevant to initiating lawsuits.
Some large epidemiologic studies have associated the use of CS in the first trimester with nonsyndromic orofacial clefts (a small statistical risk).38,39 However, Gur and colleagues did not find any teratogenic risks in humans in a prospective study of 311 pregnancies. 40 Prednisone is classified as risk D in the first trimester and risk C after the first trimester as problems have not been observed in later pregnancy. Large doses near the time of delivery may produce fetal hypothalamic-pituitary axis suppression, which is not usually clinically significant.2,38,39 Prednisone has less effect than other CSs on the fetus because only minimal amounts reach the fetus in an active form as the placenta is rich in an enzyme (11β-hydroxysteroid dehydrogenase) that inactivates prednisolone. Fluorinated CSs, such as dexamethasone and betamethasone, are minimally altered by this enzyme, so higher concentrations reach the fetus. 5 Prednisone is secreted in small amounts into the breast milk, but this is not felt to pose a problem for the infant, and the American Academy of Pediatrics has determined that prednisone is compatible with breast-feeding. 41
Relatively few drug interactions have been reported with STP. Antagonism of the anticoagulant activity of coumadin has been reported; therefore, international normalized ratio clotting times should be monitored. The half-life of prednisone is decreased and its clearance rate is increased by phenytoin, phenobarbital, and rifampicin. This is not usually clinically significant with the use of STP.3,4,42
Normal antibody response to immunization or allergy procedures occurs in patients receiving less than approximately 20 mg per day of prednisone. Nevertheless, it is best in most cases to delay procedures until their CS dosage is complete because larger doses can alter results.5,42 The American Academy of Paediatrics recommends that the administration of live vaccines be avoided while an infant is receiving CS as there are concerns about the varying degrees of immunosuppression leading to increased side effects. 43
Erdmann and colleagues reviewed anaphylaxis induced by CS and reported a case of a 22-year-old woman with atopic dermatitis who had an anaphylactic reaction after oral administration of prednisone. 44 Subsequent skin-prick testing showed immediate-type hypersensitivity to prednisolone, prednisone, and betamethasone but not to methylprednisolone or dexamethasone. Patch testing in this same patient showed delayed-type hypersensitivity to prednisolone, amcinonide, and clobetasol propionate. They noted that clinicians should be aware that allergic reactions to glucocorticoids can occur and that worsening of symptoms does not always mean treatment failure. 44
A review of the surgical and dermatologic literature did not reveal any association between STP and delayed wound healing.
Conclusions and Preventions
Patients given STP must be informed of all material risks and treatment options, and thorough chart documentation is required. The indications for CS use and dosage levels must be sound, and the record should clearly document the severity of the illness and the weighing of treatment alternatives. Patients should be asked about (and warned about) the hazards of receiving additional CSs from other physicians. Repeated courses on STP may have a cumulative effect, 32 so a record should be made of the patient's total CS intake. Attention should be paid to the patient's previous medical problems and current medications. There is no hard evidence to indicate that other routes of administration are safer than the oral route. AVN has been reported with high-dose intravenous CSs. 32 Nasser and Ewan reported a case of AVN developing in a 42-year-old man who had received annual injections of intramuscular CS for 11 years for severe hay fever. 45 The lower number of reported cases associating CS with AVN is probably a reflection of the lower use of intramuscular CS compared with oral CS than a true physiologic difference. There is little hard science available comparing intramuscular CS with oral CS. Serious side effects are well documented with long-term intramuscular CS. 46 Dasgupta and colleagues found fewer side effects with intramuscular CS than with oral prednisolone in a 96-week trial in 60 patients with polymyalgia rheumatica. 47 However, more studies with larger numbers and different diseases are required to establish if there is any true difference between intramuscular CS and oral CS.
The literature reviewed in this article clearly indicates that a short course of STP of 1 week, in the absence of specific contraindications, is unlikely to be harmful (psychotic or prepsychotic episodes possibly excepted).
There are several avenues to informed consent, but the most appropriate is a dialogue between the physician and the patient with physician documentation of the discussion in the patient's chart. A consent form does not replace this process, but some physicians feel it serves as a memory jog for the patient and the physician. If a consent form is used, the patient's signed copy should be in the chart and the other copy given to the patient.
Footnotes
Acknowledgments
The research excellence of the librarians of the North York General Hospital in Toronto, Gaby Fernandes and Maureen Pakosh, enabled me to obtain the information required for this article. Typing was done by Linda Thoms and Lora Naccarato.