
Abstract
Background:
Desmoplastic squamous cell carcinoma (DSCC) is a variant of squamous cell carcinoma (SCC) with aggressive histologic and clinical features. DSCC has a 6 to 10 times higher rate of both local recurrence and metastatic spread compared with well-differentiated SCC. Clinical estimation of tumor margins can grossly underestimate both the depth and the peripheral extent of the tumor. Surgery with intraoperative margin control has been recommended. In many cases, postoperative radiotherapy or prophylactic lymph node dissection may be required.
Case Presentation:
A 71-year-old man with a biopsy positive for DSCC involving the left postauricular area was treated with nine-stage Mohs micrographic surgery before the tumor margins were negative.
Conclusion:
There are minimal reports in the literature pertaining to the presentation and treatment of DSCC; therefore, definitive conclusions are difficult. The depth of tumor penetration and peripheral spread of the DSCC presented in this case, however, supports the need for aggressive surgical excision, preferably with intraoperative margin control. To maximize the chance of cure, physicians must be aware of the distinct clinical and histologic features of DSCC and the aggressive treatment required.
SQUAMOUS CELL CARCINOMA (SCC) is the second most common type of skin cancer and has previously been reported to cause approximately 2,500 deaths in the United States per year secondary to metastatic spread. 1 Extrapolating from this, we would estimate that there are approximately 300 deaths in Canada per year secondary to metastatic spread of SCC. Importantly, the incidence rate of SCC is increasing in both the United States and Canada, as well as other parts of the world.2-4 Several histologic subtypes of SCC have been described, with differing prognostic implications. 5 Most clinicians believe that SCC that demonstrates desmoplastic histology exhibits more aggressive biologic behavior and consequently has a higher risk for local recurrence and metastasis. 6
Desmoplastic squamous cell carcinoma (DSCC) was first described in 1989 as having a histologic pattern demonstrating fine branches of tumor cells at the periphery with a surrounding desmoplastic stromal reaction. 7 Later studies confirmed this histologic appearance.6,8 In addition, perineural and perivascular involvement is frequently present.5,8
Clinically, DSCC commonly looks like other malignant epithelial tumors of the skin. 9 It occurs commonly in sun-exposed areas of the head and neck, much like other forms of SCC; however, DSCC appears to have a predilection for the ear and appears less frequently on the vermilion surface.5,6,8 There does not appear to be a significant difference in age or gender distribution when comparing desmoplastic and nondesmoplastic SCC. 5 DSCC has been reported to metastasize more frequently than typical SCC of comparable tumor thickness. 8
We report a case of DSCC involving the postauricular sulcus and ear, with invasion deeper than clinically suspected. The presented case and supporting literature review highlight the clinical features and treatment recommendations needed to maximize patient care.
Methods and Results
A 71-year-old, nonsmoking male presented with a 1-year history of a slow-growing ulcerated plaque behind his left ear. Initially, the area was erythematous, scaling, thickened, and intermittently pruritic. Occasionally, the area would bleed with mild trauma. The patient was initially assessed in the community after 6 months of symptoms and prescribed an ointment in an attempt to alleviate the pruritus. With no improvement, a biopsy was taken.
The suspected clinical diagnosis was basal cell carcinoma. Pathologic review of the biopsy, however, demonstrated invasive nests and cords of malignant epithelial cells showing squamous differentiation and a markedly desmoplastic stroma. A histologic diagnosis of DSCC was given. The patient was expediently booked for Mohs micrographic surgery (MMS).
At the time of the MMS, the ulceration, induration, and crusting in the left retroauricular area, measured 5.2 × 2.3 cm. No adenopathy was present. MMS was performed in the standard fashion using hematoxlin-eosin staining (Figure 1). Histology revealed very small, well-differentiated tumor islands of SCC cells within a markedly desmoplastic stroma (Figure 2). Nine stages of Mohs levels were required until adequate margins were obtained, leaving a defect of 8.3 × 5.1 cm, with maximal depth to the periosteum over the tympanic portion of the external auditory meatus and mastoid. Reconstruction involved multiple local flaps, as well as a full-thickness skin graft harvested from the left supraclavicular region. Recommendations for postoperative radiotherapy were discussed with the patient.
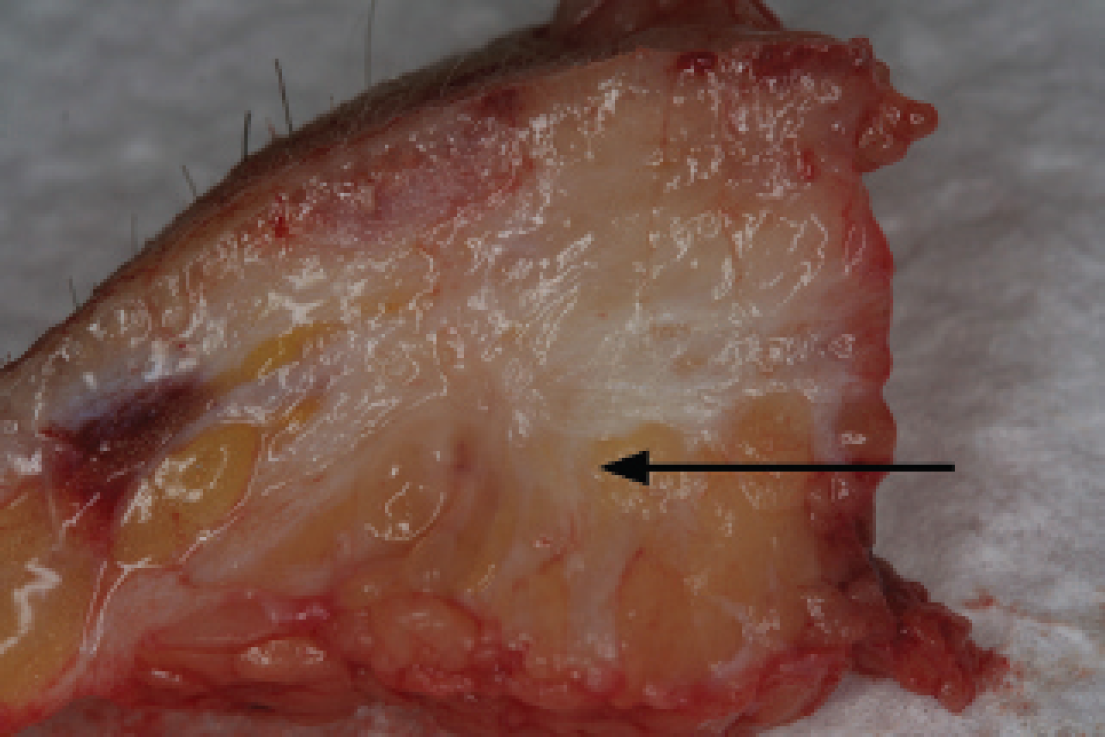
Gross pathology of desmoplastic squamous cell carcinoma showing infiltrating tumor strands.

Histology of desmoplastic squamous cell carcinoma showing small tumor islands with desmoplastic stroma (hematoxylin eosin stain; ×40 original magnification).
Conclusion
DSCC occurs commonly in sun-exposed areas of the head and neck, much like common SCC, and has been shown to represent approximately 7 to 10% of all cutaneous SCCs. 8 DSCC appears to have a greater predilection for the ear.6,8 This was demonstrated by Breuninger and colleagues, who reported that 20.4% of the 44 DSCCs in their study were located on the ear, compared with 9.8% for common SCC. 8 Evidence in the literature generally suggests separating DSCC from other SCC subtypes owing to the higher rate of local recurrence and metastatic spread. 5 This is important as disease-free survival rates significantly drop when desmoplasia is present. 10 DSCCs with a tumor thickness greater than 5 mm are believed to display the most aggressive biologic behavior. 8
The overall rate of recurrence and metastasis for SCC is relatively low at 2 to 3% and 3 to 5%, respectively.5,8 In 1997, Breuninger and colleagues performed the first comprehensive assessment of the histomorphology and biologic behavior of DSCC in a prospective study of 594 SCCs from 509 patients. 8 In that population, 44 DSCCs were identified by light microscopy (7.4% of total SCCs in the study). All of the SCCs were treated with standard micrographic surgery and had a median follow-up of 5 years. DSCC was found to metastasize 6 times more often (22.7% vs 3.8%) and had 10 times more local recurrences (27.3% vs 2.6%). All local recurrence and metastatic spread (occurring first in the regional lymph nodes in all cases) were reported to have occurred within the first 4 years of follow-up.
Increased recurrence and metastasis rates for DSCC are likely due to the greater difficulty in clinically and histologically detecting peripheral tumor compared with standard SCC. 8 The relative paucity of tumor cells at the tumor periphery makes judging the clinical end point of the tumor difficult and can lead to inadequate surgical margins. The difficulty in assessing clinical margins is demonstrated in our case, in which nine MMS layers were required before tumor clearance was achieved. The initial tumor size was estimated as 5.2 × 2.3 cm; however, the final defect size was 8.3 × 5.1 cm. More importantly, the tumor was significantly deeper than clinically evident, invading to the mastoid periosteum. For similar reasons, histologic determination of completeness of excision is demanding in both paraffin-embedded and frozen-section preparations. This can lead to a false-negative pathology report regarding the completeness of tumor excision. In addition, DSCCs may have an intrinsically more aggressive cell biology,8,11 increasing the ease of single-cell survival and tumor infiltration into surrounding tissues.
Several recommendations have been made in the literature for the treatment of DSCC.6,8,9 Wide surgical margins are required, with the minimum recommendation of 6 to 10 mm circumferentially. In the case we presented, a 10 mm margin would have been grossly inadequate. If available, MMS, with its exact margin control, is the surgical treatment of choice. The need for postoperative radiotherapy remains controversial. Consideration for postoperative radiotherapy should be made on a case-by-case basis according to the surgeon's confidence in the adequacy of excision, anatomic location, age, and patient health status. Prophylactic lymph node dissection should be considered for tumors with a thickness of 5 mm or greater.6,8 Close clinical follow-up is mandatory.5,6,8,9 There is currently no accepted standardized follow-up protocol for treated DSCC; however, review of the patient every 3 to 6 months for the first 4 years is suitable.
The presented case illustrates and supports the literature on the aggressive clinical presentation of DSCC. Physicians involved in cutaneous oncology must be aware of this histologic variant of SCC and understand the treatment modifications required if acceptable cure rates are to be obtained.