
Abstract
Background:
Since the advent of biologic therapies for psoriasis, reports of efficacy in nail psoriasis have appeared in the literature and at international conferences with increasing frequency.
Objective:
This article aims to review the existing literature on the use of biologics in the treatment of nail psoriasis.
Methods:
An extensive literature review was conducted using OVID Medline. Studies examining the efficacy of biologics in the treatment of nail psoriasis were documented.
Results:
A literature review revealed few clinical trials specifically concentrating on nail psoriasis; however, nails have been assessed in larger clinical trials for cutaneous psoriasis. A large, multicenter, phase III, double-blind, placebo-controlled study of infliximab administered as a brief induction regimen at weeks 0, 2, and 6 followed by a single infusion every 8 weeks revealed statistically significant mean percent improvement in the Nail Psoriasis Severity Index (NAPSI) score over placebo at both week 10 (26.8% vs −7.7%, respectively; p < .001) and week 24 (57.2% vs −4.1%, respectively; p < .001). For other biologics, evidence has thus far been largely anecdotal, appearing as either case studies or extracted secondarily from open-label prospective trials in plaque psoriasis or psoriatic arthritis.
Conclusion:
Infliximab appears to be the most effective treatment for nail psoriasis to date.
PSORIASIS is a chronic, immune-mediated disorder affecting approximately 3% of the world population.1,2 Although it is estimated that between 10 and 50% of psoriasis patients will develop nail involvement, the incidence of nail psoriasis in patients with psoriatic arthritis is reportedly higher than in those patients with psoriasis alone.3–7 Furthermore, nail lesions are positively correlated with both longer duration and greater involvement of psoriasis.3,8 Nail changes associated with psoriasis typically include pitting, oil spots, subungual hyperkeratosis, distal onycholysis, leukonychia, focal onycholysis, thin nails, erythema of the lunula, salmon patches, and splinter hemorrhages. 9 Pain and difficulty with daily activities are commonly reported in patients with nail psoriasis.10,11
To date, treatment of nail psoriasis has been challenging. Currently, management of nail psoriasis involves topical, intralesional, and systemic therapies. 12 With the increasing use of biologic therapies to treat psoriasis, studies conducted with regard to treating the nail manifestations of psoriasis are starting to emerge. Although most of these studies are still largely anecdotal or derived from open-label prospective studies, the efficacy of infliximab, an anti–tumor necrosis factor α (TNF-α) agent, in the treatment of nail psoriasis has recently been documented in a large, multicenter, double-blind, placebo-controlled study. 3
Methods
An extensive literature review was conducted using OVID Medline. Studies examining the efficacy of biologics in the treatment of nail psoriasis were documented. The Nail Psoriasis Severity Index (NAPSI) served as a marker of nail improvement. This grading system divides each nail into quadrants with imaginary horizontal and longitudinal lines. Each nail is given a score out of 4 for both nail matrix (pitting, leukonychia red spots in the lunula, and nail plate crumbling) and nail bed features (oil drop discoloration, onycholysis, nail bed hyperkeratosis, and splinter hemorrhage). Each nail receives a NAPSI score out of 8, and the sum of all the nails is the total NAPSI score (Figure 1). 11
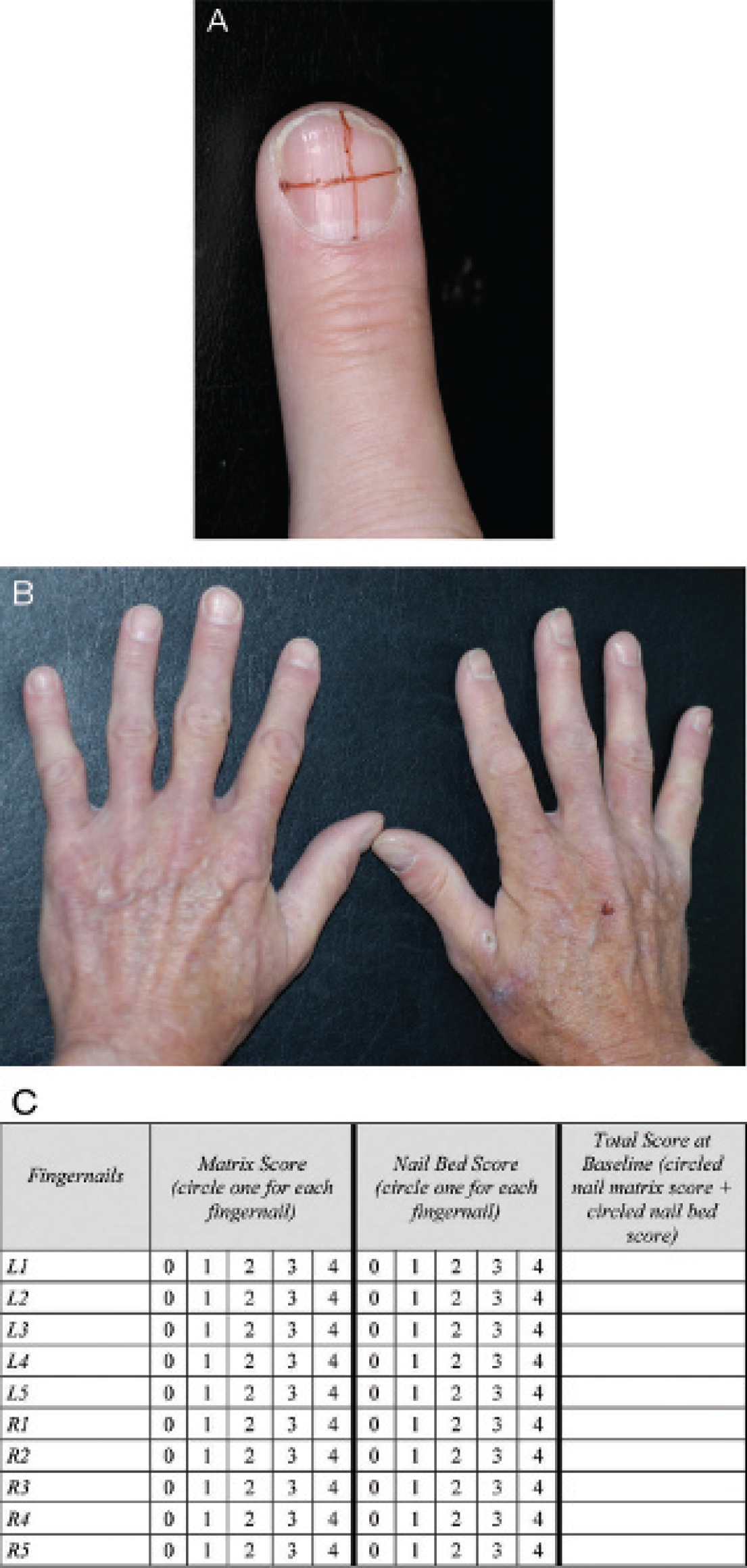
Determining the Nail Psoriasis Severity Index (NAPSI) score. A, Nail matrix psoriasis consists of any of the following: pitting, leukonychia, red spots in the lunula, and nail plate crumbling. Nail bed psoriasis is the presence or absence of any of the following: onycholysis, splinter hemorrhages, oil drop (salmon patch) discoloration, and nail bed hyperkeratosis. Score for matrix psoriasis or nail bed psoriasis (0−4): 0 = none; 1 = present in one-quarter of the nail; 2 = present in two-quarters of the nail; 3 = present in three-quarters of the nail; 4 = present in all of the nail. B and C, Ten fingernails on the hand will be evaluated for nail matrix psoriasis and nail bed psoriasis. The sum of these two scores is the total score for each fingernail.
Results
Infliximab
In a large, multicenter, phase III, randomized, double-blind, placebo-controlled trial (EXPRESS trial) designed to evaluate the efficacy and safety of induction and maintenance infliximab in patients with moderate-to-severe psoriasis, 5 mg/kg was administered as a brief induction regimen at weeks 0, 2, and 6 followed by a single infusion every 8 weeks. 13 The data were subsequently analyzed by Rich and colleagues, and a statistically significant mean percent improvement in the NAPSI was seen over placebo at both week 10 (26.8% vs −7.7%, respectively; p < .001) and week 24 (57.2% vs −4.1%, respectively; p < .001). 3 Of those patients with baseline nail psoriasis, 6.9%, 26.2%, and 44.7% in the infliximab group had clearance of their nail involvement at weeks 10, 24, and 50, respectively, compared with 5.1% in the placebo group at week 24. Over two-thirds of the patients demonstrated resolution of some of the nail bed and nail matrix manifestations by week 10. The most rapid improvement among nail matrix features was for lunular red spots, whereas for nail bed features, splinter hemorrhages improved the most quickly. The most commonly and severely affected nail was the right thumbnail.
A small, open-label, not placebo-controlled, prospective study by Bianchi and colleagues evaluated the effectiveness of infliximab therapy in nail psoriasis for 25 patients with either plaque-type psoriasis or psoriatic arthritis. 14 Intravenous doses of infliximab (5 mg/kg) were given at weeks 0, 6, 14, and 22. At week 22, the mean NAPSI was 0 for all patients.
Etanercept
In an ongoing, randomized, open-label study by de Rie and colleagues, patients with moderate-to-severe plaque-type psoriasis received etanercept either continuously or intermittently over the first 12 weeks. 15 At baseline, 519 of 708 patients had nail psoriasis. The mean NAPSI score was 4.6 at baseline and 3.3 at week 12, representing a mean 28.2% reduction in the severity of nail psoriasis.
In another large, 12-week, double-blind, randomized, multicenter, clinical trial, patients received either 50 mg etanercept twice weekly subcutaneously or placebo. 16 At week 12, photographic documentation of the nails of 31 etanercept-treated patients suggested that they experienced a mean improvement in NAPSI score from baseline compared with a mean worsening in the placebo group (−3.0 vs 8.6; p = .0515).
Efalizumab
Efalizumab, administered at 1 mg/kg/week subcutaneously, was used as therapy for nail involvement in four psoriasis patients. All four patients responded favorably to treatment, one of whom showed complete resolution of her nail psoriasis in 19 weeks. Pits, oil spots, subungual hyperkeratosis, distal onycholysis, leukonychia, and splinter hemorrhages disappeared with treatment. 9
In a multicenter, open-label study, treatment with efalizumab resulted in improvement of nail psoriasis. Patients were given a single conditioning dose of 0.7 mg/kg subcutaneously, followed by 1 mg/kg/wk subcutaneously for 23 weeks and then 12 weeks of observation. By week 12, nearly half of all patients (43%) achieved ≥ 50% improvement in their NAPSI score. 17
Efalizumab has also demonstrated favorable efficacy in a 24-week, multicenter, open-label, single-arm, phase IIIb/IV study in patients with moderate-to-severe plaque psoriasis in Latin America. One hundred eighty-nine patients received weekly subcutaneous doses of efalizumab (0.7 mg/kg at day 0 and 1.0 mg/kg/wk during weeks 1–23). At baseline, 112 patients (59.2%) had nail psoriasis, with a median NAPSI score of 14. At week 24, approximately 31% of patients achieved at least 50% improvement in NAPSI score and 17% improved by at least 75%. 18
Adalimumab
In a large, open-label, prospective study, adalimumab (40 mg) was administered subcutaneously every other week for 12 weeks to adults with active psoriatic arthritis. Clinically significant NAPSI improvements were seen as early as week 12, with a mean absolute change in NAPSI score of −9.5 in those patients whose psoriatic arthritis also responded favorably to treatment and −6 in those patients whose psoriatic arthritis did not respond. 10
Alefacept
In an open-label, multicenter study by Cassety and colleagues, a retrospective analysis of six patients with nail psoriasis was conducted.19,20 Three patients treated with alefacept, which was administered through 15 mg intramuscular injections once weekly for 12 weeks, showed ≥ 30% improvement in their NAPSI score 6 weeks after the last dose. Of the nail features observed, pitting was the most refractory to treatment.19,20
In a prospective, open-label, pilot study by Parrish and colleagues, a 39% mean reduction in modified target NAPSI score from baseline was observed at week 24, following 12 weeks of therapy with alefacept. Patients received 15 mg intramuscular injections of alefacept weekly for 12 weeks. At week 24, 13 of 15 patients demonstrated improvement in nail psoriasis, with 5 of 15 patients achieving ≥ 50% improvement from baseline in total NAPSI score. 21
Discussion
Nail psoriasis, which occurs in the majority of patients with psoriasis, is one of the lesser studied disorders in the field of dermatology. 12 With between 10 and 50% of patients presenting with nail-associated symptoms at some point, this greatly impacts quality of life.3,4
Nail involvement has typically been refractory to the traditional modalities of treatment, including topical, intralesional, and systemic therapies. The current treatment modalities are also often difficult to administer and are associated with short-lived remissions. Moreover, the various therapies tend to show different efficacies for the assorted nail dystrophies. 12
Increasing knowledge of the underlying mechanisms of psoriasis has led to the advent of biologic treatments, which are designed to interfere with and modify crucial mechanisms in the pathogenesis of psoriasis, including T-cell activation and cytokine release.22,23 Several biologic therapies have been approved for the treatment of psoriasis. Three anti-TNF-α agents are available, infliximab, etanercept, and adalimumab, as well as efalizumab, an anti-CD11a antibody, and alefacept, a fusion protein containing a portion of the lymphocyte function–associated antigen-3 receptor linked to human IgG. 22
With the increasing use of biologics for the treatment of psoriasis, studies regarding their efficacy in nail involvement are starting to be carried out. Although the majority of these studies are still largely anecdotal, the recent clinical trial by Rich and colleagues suggests that infliximab is effective in both an induction and a maintenance regimen for the treatment of moderate-to-severe psoriasis, as well as for nail involvement. 14 It appears that the most rapid and complete improvement associated with infliximab treatment is for lunular red spots and splinter hemorrhages. 3 The observational study of infliximab also provides promising results for the use of this anti-TNF-α agent for the treatment of nail psoriasis. 14 The most commonly reported side effect associated with infliximab therapy is infusion reactions, most of which are considered mild. 23
For the other biologics, evidence has thus far been largely anecdotal, appearing as either case studies or extracted secondarily from open-label prospective trials in plaque psoriasis or psoriatic arthritis. Readers should exert caution when dissecting the results of these studies as the numbers may be unreliable.
Conclusion
Infliximab, an anti-TNF-α agent, appears to be the most effective treatment for nail psoriasis. As evidence for other biologics has thus far been anecdotal, conclusions regarding their efficacy in the treatment of nail psoriasis are currently incomplete.