
Abstract
Background:
Oral lichenoid lesions (OLLs) resemble oral lichen planus (OLP) but develop secondary to various underlying causes. The role of contact allergy in precipitating and/or perpetuating OLL is well documented but remains controversial.
Objective:
To help elucidate the association of contact allergy and OLL, we reviewed patch-test readings in patients diagnosed with OLP-like lesions.
Methods:
We retrospectively reviewed patients diagnosed with OLP-like lesions who had patch tests performed between January 1, 2006, and December 31, 2007.
Results:
Patch tests were performed on 24 patients with a histopathologic and/or clinical diagnosis of OLP. Of these, 16 (67%) had positive patch-test readings. At least eight (50%) of these patients had clinically relevant reactions. Ten of the 16 patients (63%) had reactions to metals. In most of these patients, troublesome areas tended to localize adjacent to metallic dental restorations. Of the nine patients (56%) who had reactions to fragrances, flavorings, gallates, and/or diallyl disulfide, the majority improved after avoiding these allergens.
Conclusion:
Our findings support the notion that contact allergy may underlie the pathogenesis of OLL and that allergen avoidance may result in amelioration of disease.
ORAL LICHEN PLANUS (OLP) is an idiopathic autoimmune inflammatory condition affecting 0.5 to 2% of the population. It is more common in women, usually affecting those in their fifth to sixth decades of life.1,,–4 There are three main clinical forms of OLP: reticular (Figure 1), atrophic/erythematous, and erosive/ulcerative. Lesions are often bilateral, affecting the buccal mucosae, tongue (mainly dorsum), and/or gingivae.2,4,–6 Erosive and ulcerative lesions are often painful and, over time, may transform into squamous cell carcinoma. 7 The risk of malignant transformation varies between 0.4 and 5% over periods of observation ranging from 0.5 to 20 years.4,8

Reticular lichen planus on buccal mucosa.
The term oral lichenoid lesion (OLL) is used to describe lesions that resemble OLP clinically and histologically but develop secondary to various underlying causes. Some believe that there is an increased propensity of OLL to be unilateral4,9 and erosive 4,10 Histologic examination may show increased numbers of colloid bodies with a more diffuse lymphocytic infiltrate admixed with eosinophils and plasma cells compared with classic lichen planus. 4
Numerous underlying causes of OLL have been reported. The most common causes of drug-induced OLL include angiotensin-converting enzyme inhibitors and nonsteroidal anti-inflammatory medications.10,11 Infectious causes include viral hepatitis B and C,3,12,13 chronic candidiasis, and various other fungal and bacterial organisms. 14 OLLs are also more common in patients with various autoimmune diseases, including graft-versus-host disease, thymomas, lupus erythematosus, and alopecia areata.13,14 Other systemic associations include diabetes mellitus and hypertension.13,14 Trauma from ill-fitting dentures and emotional stress are also implicated.13,14 More recently, polymorphisms in various proinflammatory cytokines, such as interleukin-18, 15 interferon-γ, and tumor necrosis factor α, 16 have been hypothesized to influence the pathogenesis of OLL.
The role of contact allergy in precipitating and/or perpetuating OLL is also well documented but remains controversial.4,13,17,,,,,,,,,,,,,,,,–34 In the following study, we retrospectively reviewed patch-test reactions in patients with OLP-like lesions to help elucidate this association.
Methods
A chart review of patients who were diagnosed with OLP-like lesions and who underwent patch testing between January 1, 2006, and December 31, 2007, was performed. The diagnosis was established clinically by both the referring dentist and the staff dermatologist. Methylene blue staining was performed to help exclude dysplastic lesions. Punch biopsies (2 mm) of oral mucosal lesions were obtained in patients with atypical or nonspecific clinical findings. Only those patients with histopathologic findings consistent with OLP/OLL or those with classic clinical findings were included in this study. All patients had bloodwork taken to exclude other secondary causes of oral ulceration or stomatitis. This included a complete blood count and differential, serum vitamin B12, red blood cell folate, and ferritin. An autoimmune screen was also performed. Serum was sent to the laboratory, and titers were obtained for antinuclear antibody, extractable nuclear antigens, and rheumatoid factor. Lastly, hepatitis B and C serology was obtained to rule out active infection. In addition, all patients were treated with therapeutic doses of oral fluconazole once weekly to treat or prevent candidiasis.
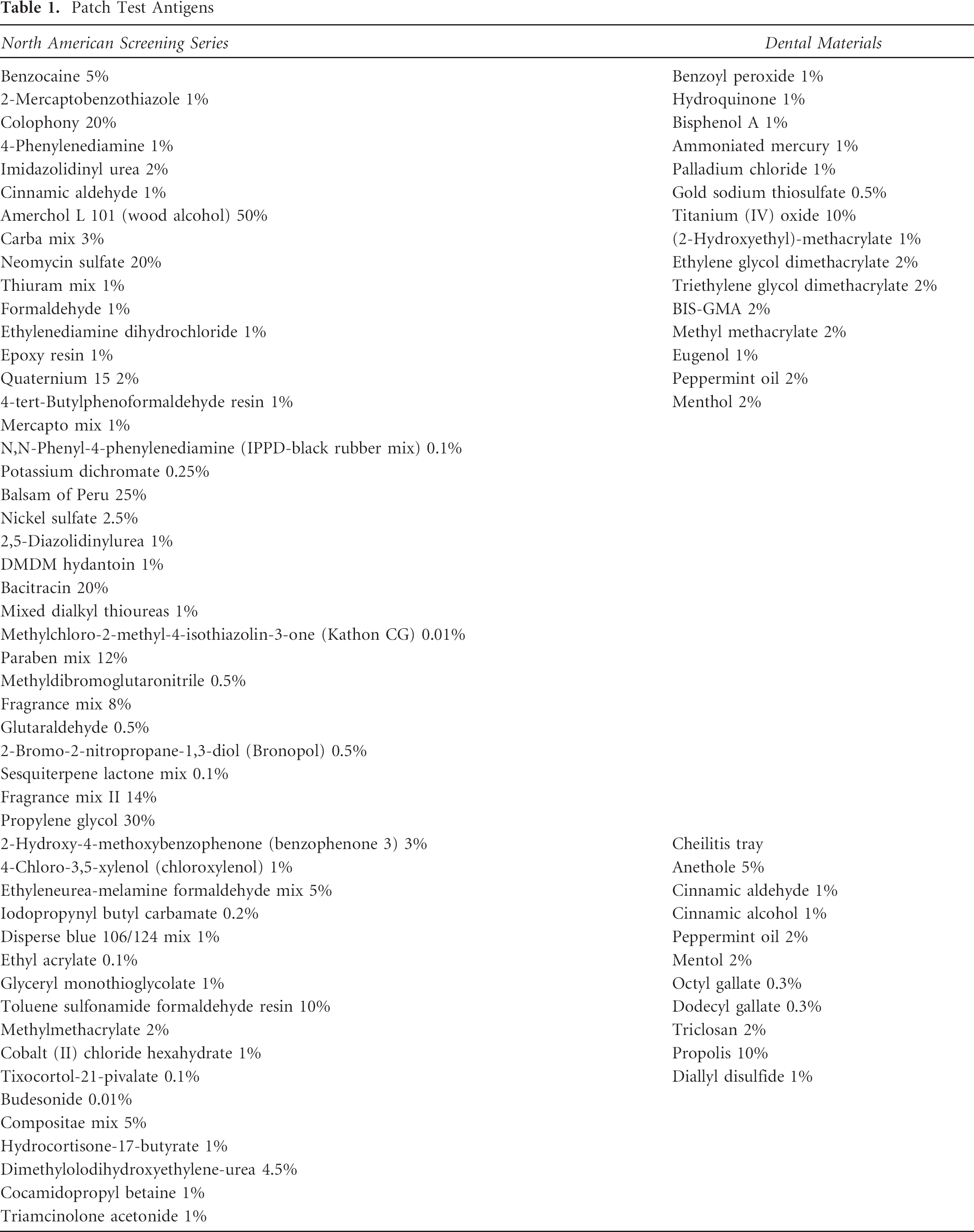
All study patients were patch-tested using our North American Standard dental and cheilitis trays (Table 1). Using standard methods, 35 antigens were placed on the back and occluded using Finn chambers (Finn Chamber, Epitest Ltd, Tuusula, Finland) and Scanpor tape (Alpharma AS, Norway). Subsequent readings were performed approximately 48 and 144 hours after initial application of the antigens. The North American Contact Dermatitis Group scoring system 35 was used. Reactions of ≥ 1+ with a “crescendo response pattern” (ie, more marked between the first and second readings) were considered positive. For example, a score of 1+ was given if the reaction was erythematous and palpable but nonvesicular, 2+ in edematous or vesicular reactions, and 3+ in spreading, bullous, or ulcerative reactions.
Patch Test Antigens
Results
Patch tests were performed in 24 patients diagnosed with OLP-like lesions. In 12 of these patients, biopsies were done to help confirm the diagnosis. We were unable to make a distinction on histopathology between OLP and OLL.
Of the 24 patients, 16 (67%) had positive patch-test readings. After a discussion of the test results, patients were given information sheets describing each allergen along with measures that could be taken to avoid further exposure. For example, patients with fragrance mix and/or balsam of Peru allergy were asked to avoid citrus, cola beverages, vermouth, clove, cassia, curry, and cinnamon- and vanilla-flavored chewing gum, candy, lozenges, and toothpaste.
To help determine the clinical relevance of these positive test results, 6 of the 16 patients were seen in follow-up clinics and 8 were contacted by telephone (2 were lost in follow-up). Allergens were labeled as being “clinically relevant” if their avoidance was correlated with improvement in or resolution of the disease. Based on these criteria, at least 8 (≥ 50%) of the 16 patients demonstrated positive reactions that were likely clinically relevant (2 patients were lost in follow-up). In total, at least 8 of 24 (≥ 33%) patients diagnosed with OLP-like lesions had disease, which seemed to improve significantly with avoidance of allergens identified using patch testing.
Of the 24 patients patch-tested, 8 (33%) had entirely negative readings. Four of these patients were lost in follow-up. One of these patients opted to seek advice from a naturopath, whereas the others were controlling their disease with local application of clobetasol ointment once daily when needed for flares.
Table 2 summarizes the demographics, past medical history, relevant medication use, results of blood tests, autoimmune screening, hepatitis serology, contact allergens, and results of allergen avoidance in the 16 patients with positive patch-test readings. Briefly, within this cohort, there were 15 females and 1 male. The mean age at presentation was 63 years (range 19–76 years). The duration of disease spanned from 6 months to 25 years (mean 4.9 years). Of the 16 patients, 14 had exclusively oral involvement and 2 had concomitant cutaneous plaques of (biopsy-proven) lichen planus. None of the patients had evidence of autoimmune disease, active viral hepatitis infection, or deficiencies of iron, folic acid, or vitamin B12. With the exception of four patients, none were taking medications implicated in OLL.10,11 In two patients who were taking NSAIDS, both improved with allergen avoidance, despite continuing to take the drug. One patient in our study was taking an ACE inhibitor, however, she was lost in follow-up. Another was taking NSAIDs regularly; however, her patch-test result was considered irrelevant, and the cause of her long-standing disease remains obscure. In our subjects, there was no identifiable correlation between a diagnosis of hypertension or diabetes and OLL.
Characteristics of 16 Patients with Oral Lichenoid Lesion and Positive Patch-Test Results
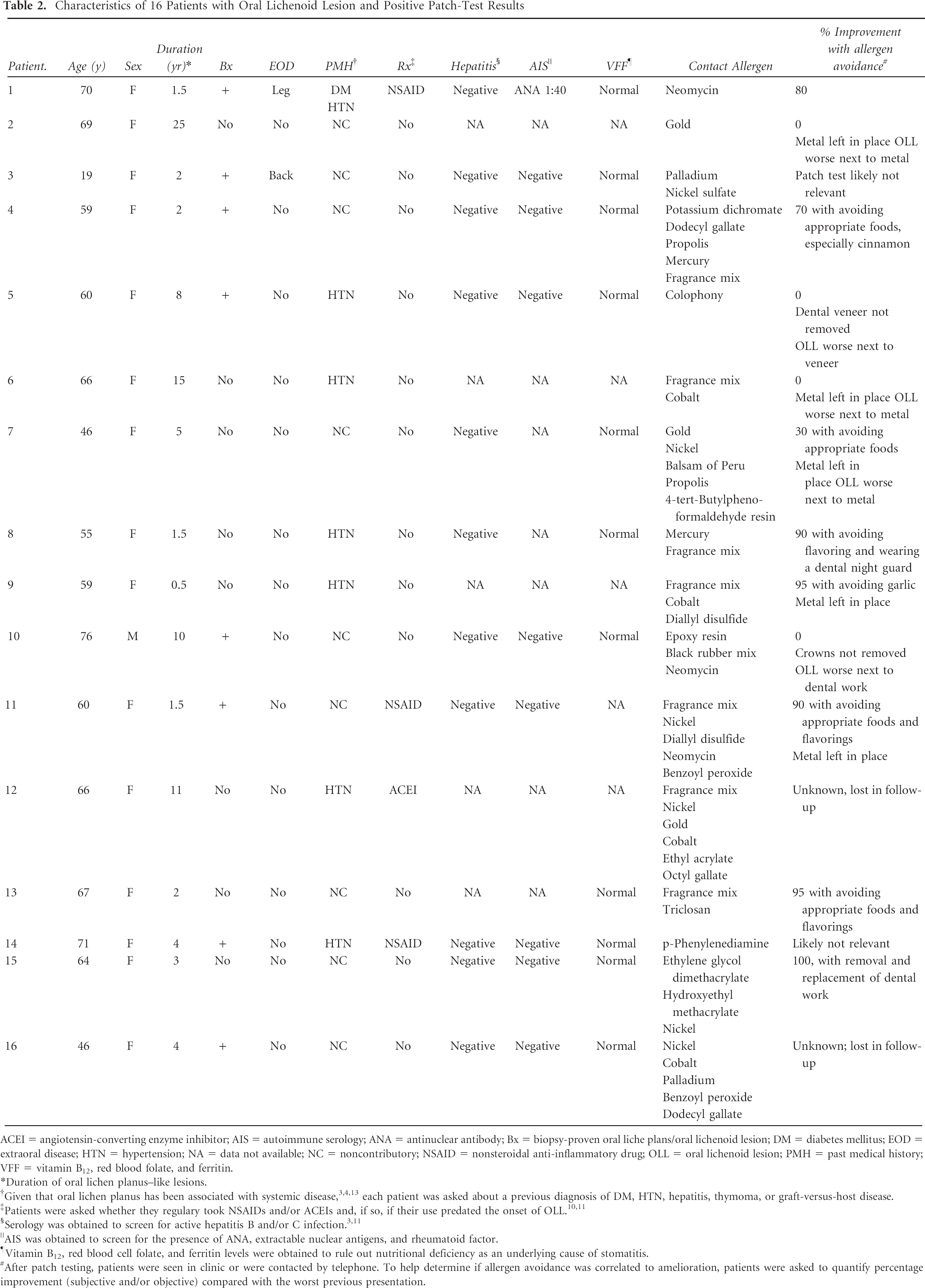
ACEI = angiotensin-converting enzyme inhibitor; AIS = autoimmune serology; ANA = antinuclear antibody; Bx = biopsy-proven oral liche plans/oral lichenoid lesion; DM = diabetes mellitus; EOD = extraoral disease; HTN = hypertension; NA = data not available; NC = noncontributory; NSAID = nonsteroidal anti-inflammatory drug; OLL = oral lichenoid lesion; PMH = past medical history; VFF = vitamin B12, red blood folate, and ferritin.
Duration of oral lichen planus–like lesions.
Given that oral lichen planus has been associated with systemic disease,3,4,13 each patient was asked about a previous diagnosis of DM, HTN, hepatitis, thymoma, or graft-versus-host disease.
Patients were asked whether they regulary took NSAIDs and/or ACEIs and, if so, if their use predated the onset of OLL.10,11
AIS was obtained to screen for the presence of ANA, extractable nuclear antigens, and rheumatoid factor.
Vitamin B12, red blood cell folate, and ferritin levels were obtained to rule out nutritional deficiency as an underlying cause of stomatitis.
After patch testing, patients were seen in clinic or were contacted by telephone. To help determine if allergen avoidance was correlated to amelioration, patients were asked to quantify percentage improvement (subjective and/or objective) compared with the worst previous presentation.
Most patients had several positive findings on patch testing (see Table 2). Eleven patients had positive reactions to metals such as gold, nickel, cobalt, mercury, palladium, and potassium dichromate. Interestingly, the next most common allergens were those found in fragrance mix and balsam of Peru (eight patients). Components of fragrance mix include cinnamic aldehyde, cinnamic alcohol, eugenol, isoeugenol, hydroxycitronellal, oak moss absolute, geraniol, α-amyl cinnamic alcohol, and benzyl alcohol. We also tested other fragrances, including lyral, citral, farnesol, and coumarin. Balsam of Peru contains benzyl cinnamate, benzyl benzoate, and vanillin. Other allergens that were detected included gallates (used to prevent oxidation of fatty acids into rancid by-products in various foods, medicaments, and cosmetics), diallyl disulfide (found in garlic), and acrylates (monomers that combine to form plastics that are used in dental restorations).
Discussion
The role of allergy in the pathogenesis of OLL has been supported by research done by others yet remains controversial.4,13,17,,,,,,,,,,,,,,,,–34 This controversy likely exists because of intrinsic limitations associated with patch testing (eg, false-positive/irritant reactions and false-negative results) along with the challenges associated with ascribing clinical relevance to positive test readings.
Of the 24 patients who were tested, 16 (67%) had 1 or more contact allergens detected. Eight of these patients were deemed to have clinically relevant reactions. Therefore, 33% (8 of 24) of patients diagnosed with OLP-like lesions were identified as having a contact hypersensitivity that exacerbated and/or caused the disease. These results compare favorably with those previously published by Yiannias and colleagues. 13 We noted a high percentage of positive reactions to metals and other materials used in dental restorations. Unfortunately, cost precluded most of these patients from replacing their dental amalgams, and as such, ascribing clinical relevance to these allergens with any degree of certainty was not possible. Nevertheless, the hypersensitivity reactions were likely relevant because disease was generally more pronounced adjacent to the corresponding restoration. This belief is supported by previous publications13,17 and our experience with patient 15, who had complete, rapid, and sustained resolution of disease following replacement of her dental work. This particular patient not only tested positive to the acrylates on our standard tray but also cross-reacted to the samples provided by her dentist.
Interestingly, as documented by Yiannias and colleagues, a large proportion of our patients had sensitivities to fragrances/flavoring agents, which, when avoided, led to amelioration. 13
The results in this study need to be interpreted with caution. Several limitations of this study include lack of controls and randomization, along with bias and confounding inherent in retrospective studies. In our 24-patient study, only 12 (50%) had biopsies to confirm a diagnosis of OLP/OLL. Of the 16 patients who had positive patch-test readings, 8 (50%) had unequivocal biopsies. Although unlikely, this raises the possibility that the other 50% of the patients in the study may have been misdiagnosed (by merely relying on clinical findings). It is conceivable that the amelioration noted by our patients was unrelated to allergen avoidance but rather to spontaneous improvement associated with the natural history of the disease. Another caveat involves the fact that many of the follow-up data (with respect to improvement with allergen avoidance) were obtained via telephone conversations with patients, without clinical observation to verify these claims.
In conclusion, although we, and others, have correlated allergy with OLL, carefully designed and properly executed prospective studies are required to further clarify the underlying causes. Many of our patients seemed to improve by diligently avoiding various allergens. Hence, we recommend patch-testing patients with OLP-like lesions (especially when lesions are confined to the mucosa in close contact with or in proximity to dental restorative materials) using the standard, dental, and cheilitis series as part of routine evaluation.