
Abstract

CHRONIC WOUNDS are becoming more prevalent as our population ages and are becoming more difficult to treat. Estimates suggest that there are 1.71 million people with leg ulcers in the United States, with the average yearly treatment cost of venous stasis ulcers being $10,000 per patient. 1 Approximately 10 to 15% of diabetic patients will develop foot ulcers, which increases the risk of amputation and death. 2 Pressure ulcer rates vary from 2.5 to 15% in hospitalized and nursing home patients; a 1990 estimate was a cost of up to $30,000 per patient to treat hospital-acquired pressure ulcers. 2 The chronic wound problem is compounded by the fact that many physicians are not trained in basic wound care principles, and there is often a lack of standardized treatment. Therefore, morbidity and the cost to health care systems from chronic wounds are increased.
Multidisciplinary wound care is emerging as an effective tool to improve wound healing and lower health care expenditures. Multidisciplinary teams allow earlier diagnosis and treatment, “one-stop shopping” with multispecialty collaboration, 2 increased compliance, development of clinical trials, and a resource for education of both patients and staff. 3 Several studies support the concept of a multidisciplinary approach to wound care. Donnelly and Shaw had 68% of patients over a 14-month period achieve complete or almost complete healing with a multidisciplinary complex wound care service. 4 Trang and colleagues found in a nursing home setting that a higher number of leg and pressure ulcers healed when being treated by a multidisciplinary team compared with ulcers that received the usual care. 5 There also was a cost saving of $277.90 per wound, mostly related to decreased nursing time. 5 It has been noted that concept centers improve the rate of healing in leg ulcers and decrease the necessity for major amputations. 6 Diabetic foot ulcers also require a prompt and accurate diagnosis to preserve the foot and should involve a multidisciplinary team. 7
Multidisciplinary centers have been increasing in numbers but differ in their structure. Teams involve any of the following specialties: dermatology, plastic surgery, internal medicine, infectious disease, vascular surgery, orthopedics, podiatry, and wound care nurses. Most care is provided on an outpatient basis. A thorough history is taken and a physical examination is performed during the first visit, with serial measurements and photographs of wounds documented at each visit. The wound is described based on location and size, and the wound bed is characterized by the presence of granulation tissue, exudate, color, infection, or inflammation. Débridement may be done as necessary. Ankle-brachial indices can be assessed both in clinic using Doppler ultrasonography and by noninvasive vascular studies in a vascular laboratory. Comorbidities are taken into account, and screening for contributing factors such as smoking, obesity, hypertension, peripheral vascular disease, diabetes, and hyperlipidemia is routinely performed. Centers may operate on a daily or weekly basis. Patients are often seen repeatedly, and the numbers of patients seen at each center vary depending on resources. One wound care center in Tennessee saw 2,685 patients over a 7-year period. 2
Our multidisciplinary wound care clinic began in November 2006 and is located at the L.A. Miller Centre, part of Eastern Health, St. John's, Newfoundland and Labrador. The team initially included wound care nurses, dermatology, orthopedics, plastic surgery, and vascular surgery. A lymphedema nurse recently joined the team in October 2008. Dermatology and wound care nurses are present weekly, with surgeons rotating through on a monthly basis. There is easy access to prosthetics and podiatry.
As of January 7, 2009, the wound care clinic has seen 398 new patients. Many have been seen in follow-up multiple times. The demographics show an even division between gender, with 198 male and 199 females. The age groups categorized by decade are illustrated in Figure 1. The greatest number of patients were in their fifties and sixties. Types of ulcers included venous (33%), neuropathic (23%; diabetic neuropathy, spina bifida, hereditary sensory neuropathy), pressure (11%), other (11%; connective tissue disease, hidradenitis, pilonidal sinus, inflammatory bowel disease, etc.), mixed (10%; combination of two or more of the types), arterial (5%), trauma (4%), and postsurgical (3%) (Figure 2). This was similar to types of wounds seen in other studies of multidisciplinary wound teams, including Sholar and colleagues, where the most common was “other” ulcer type, followed by venous and pressure ulcers. 2 Arterial and postsurgical wounds were the least commonly seen. These findings are consistent with the literature as venous ulcers represent 80% of ulcers, with a prevalence of 0.16 to 2%. 8 Several younger patients were seen in our clinic as well, including children, one of whom had spina bifida and one with sclerodermoid graft-versus-host disease with secondary foot ulcers. Approximately 34% (135) of patients' ulcers healed after being seen in our multidisciplinary wound clinic. Four patients were sent directly for amputation at their first visit. Fifteen patients have died since the inception of the clinic, most from other comorbidities. Three patients died as a direct result of their wounds: one lady with calciphylaxis and two patients with sepsis secondary to wet gangrene. There were five cases of significant contact allergic dermatitis to dressings (requiring treatment other than discontinuing the dressing).
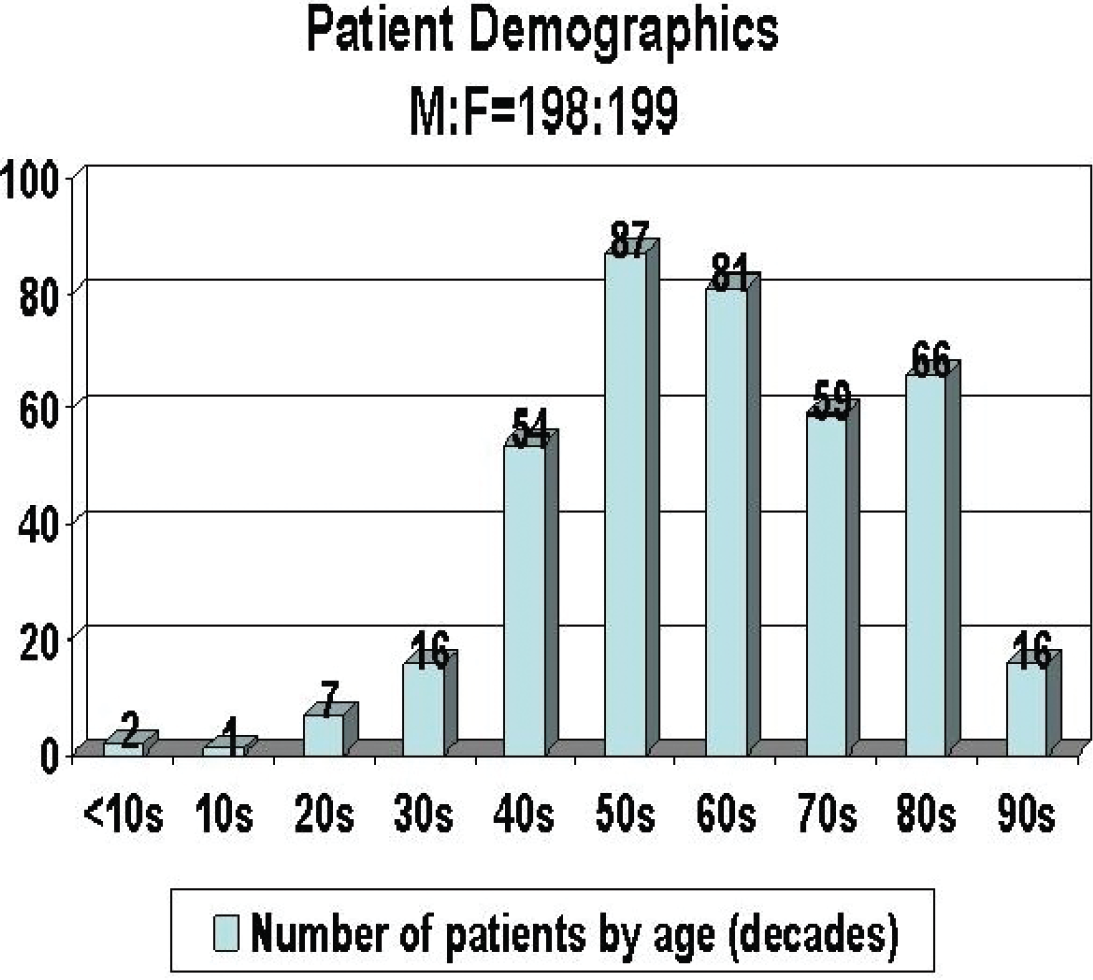
Numbers of patients seen according to age (in decades) at a multidisciplinary wound care clinic.
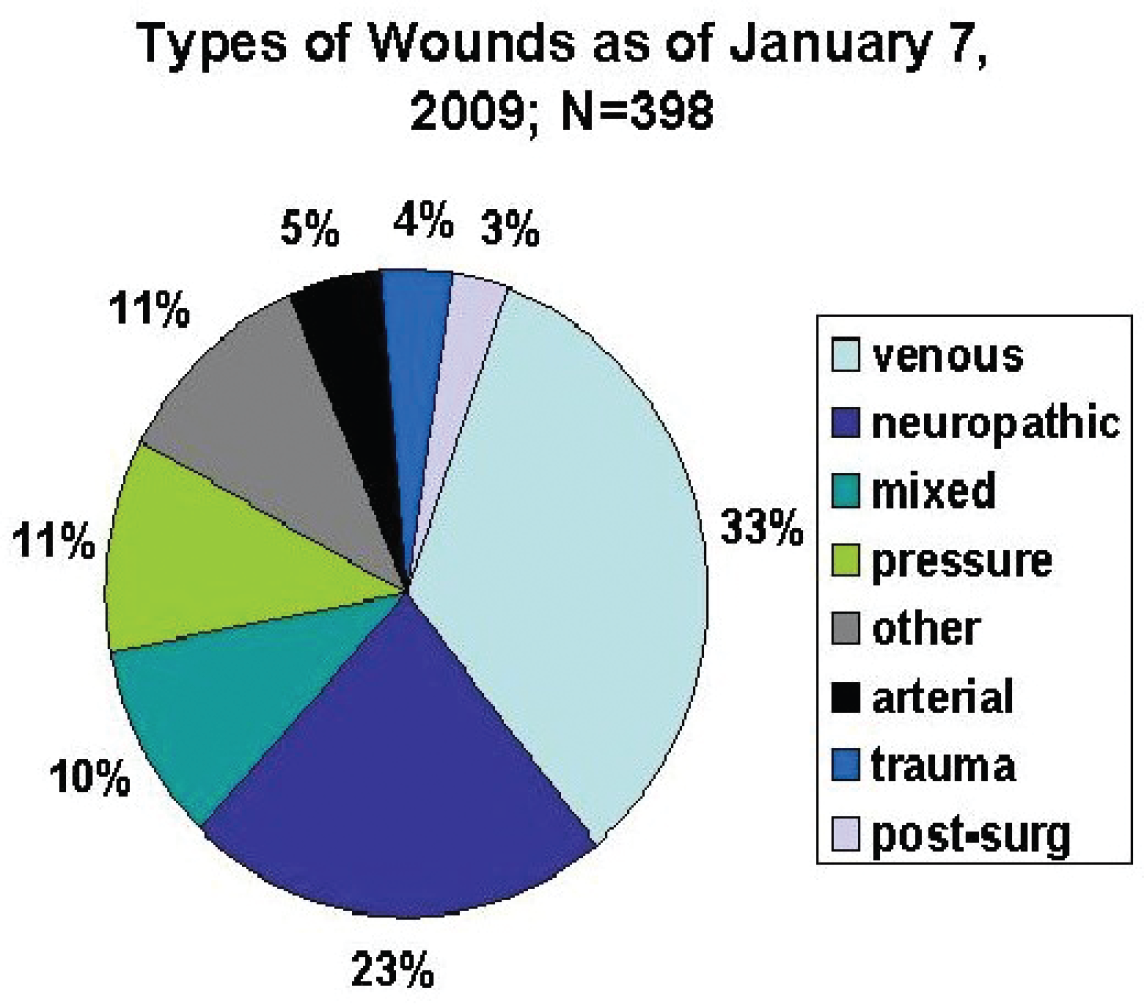
Types of wounds seen in a multidisciplinary wound clinic from November 22, 2006, to January 7, 2009 (n = 398).
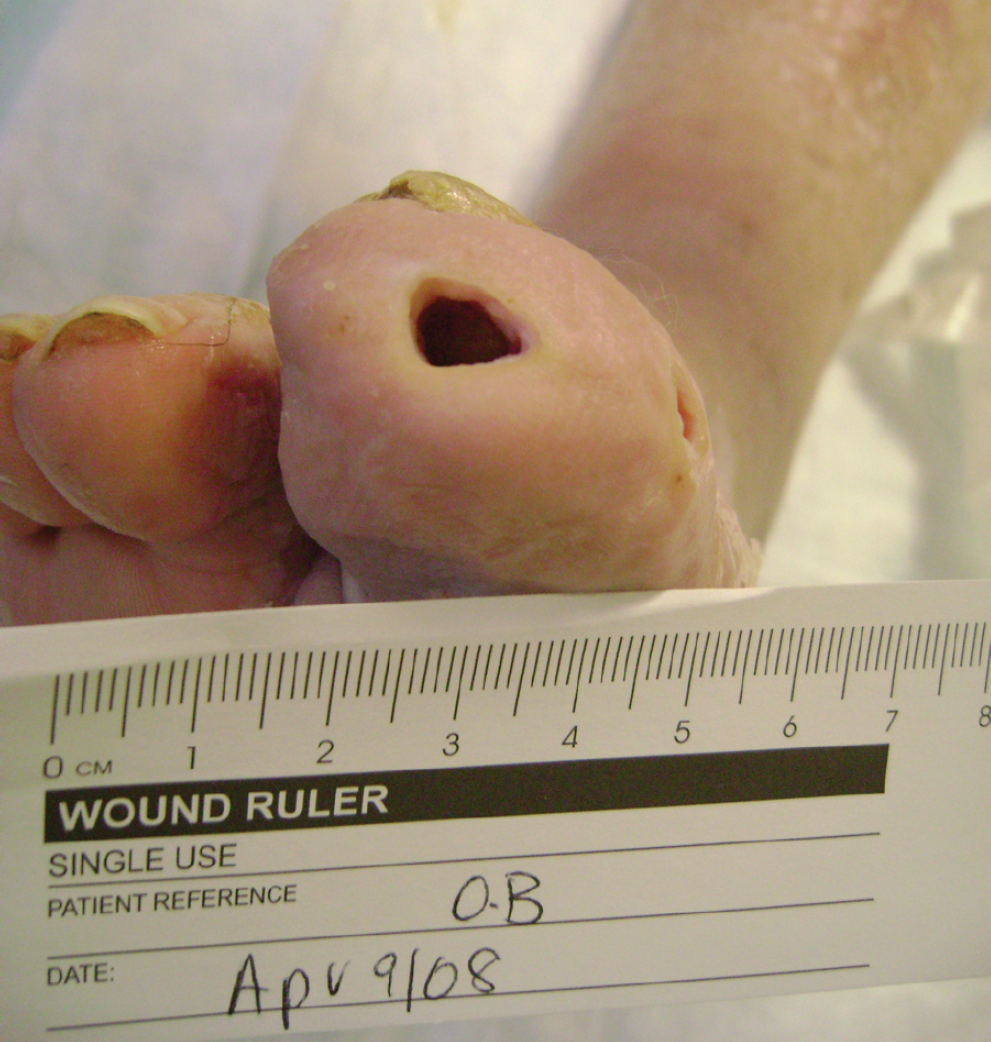
The following case from our clinic illustrates the importance of multidisciplinary care. A 66-year-old male with a history of type 2 diabetes for 10 years presented with a neuropathic ulcer on the plantar surface of the right great toe of 3 months' duration (Figure 3). He had an ulcer measuring approximately 2.5 × 2 cm with associated large exudate and erythema, suggesting cellulitis. The wound was macerated. Bone was palpable in the wound, and the patient was positive for methicillin-resistant Staphylococcus aureus. Osteomyelitis was suspected. The patient was initially started on trimethoprim-sulfamethoxazole orally and a silver and calcium alginate dressing. A radiograph confirmed osteomyelitis. One week later, the patient was reassessed when orthopedic surgeons were present at the clinic. The wound had worsened over the week, with increased size, maceration, drainage, and pain. The orthopedic surgeon felt that the best treatment option was to débride the infected bone. The infected metatarsal bone was removed in the wound care clinic with only local anesthesia and aseptic technique. Antibiotics were continued, and the dressing was changed to a hypertonic saline gauze, which was changed daily. Within 1 month, the wound was almost closed, with decreased drainage (Figure 4). The patient reported a substantial decrease in pain. Two months after débridement, the wound was closed.

Neuropathic ulcer with osteomyelitis in a patient with type 2 diabetes, prior to bone débridement.
Neuropathic ulcer 1 month after bone débridement showing great improvement.
The patient did not return for follow-up for over 4 months. To date, he has had no further issues. He was instructed to wear orthopedic shoes and follow a proper foot care regimen. Without the multidisciplinary clinic, débridement of his wound would have been delayed several weeks (perhaps months), and it is quite likely that the patient would have eventually required an amputation. Risk of amputation in diabetic foot ulcers varies from 14 to 24%; 5-year mortality after amputation is anywhere from 39 to 68%. 9 It is our belief that appropriate and timely treatment saved this patient from an impending amputation and therefore decreased his risk of death in the next several years.
Multidisciplinary wound care improves outcomes. It allows “one-stop shopping” and provides appropriate and comprehensive care, along with continuity of care. 6 It also allows teaching between specialties and decreases morbidity and costs. Patients enjoy the convenience of seeing multiple doctors in one visit.
The goal of our multidisciplinary wound care team is to perform research based on a database being developed from our clinic. The database would be partially funded by a research grant awarded from the Memorial University of Newfoundland Medical Graduates Society (Dr. Wallace Ingram Award for New Faculty 2008). We hope to determine more effective dressing regimens and perform a quality assurance study involving both patient and physician satisfaction. From our database, it would be helpful to document how many patients had difficulty with the cost of treatment (ie, compression stockings, podiatry, orthotic shoes) so that our provincial government could be approached to provide funding for these essential but costly treatments. Cost of chronic wound care and its effect on compliance have been significant issues in our multidisciplinary center. We hope to illustrate that the benefits of multidisciplinary wound care far exceed the ultimate cost to health care systems for long-term treatment of difficult chronic (and often recurrent) wounds.
Footnotes
Acknowledgment
Financial disclosure of authors and reviewers: None reported.