
Abstract

To the Editor:
A 42-year-old businessman presented with an asymptomatic, gradually expanding, elevated skin lesion on his right forearm for the duration of 1 year. There was no history of injury or preexisting skin lesion at that site. His personal and family histories were both negative for any form of skin cancer. He had no systemic symptoms.
Cutaneous examination revealed a well-demarcated, nontender plaque measuring 6 × 7 cm in size and studded with multiple dome-shaped nodules at the margin (Figure 1). The nodules (approximately 1 × 1.5 cm) were firm in consistency and had central keratin-filled craters. There were multiple small shallow cribriform scars at the center of the plaque. There was no regional lymphadenopathy. Examination of the cutaneous appendages was normal. His physical examination and review of systems were unremarkable. Routine laboratory investigations were normal.

Well-demarcated plaque showing central cribriform scars and bordered by multiple dome-shaped nodules with a keratinous crater.
Histopathologic examination of an excisional biopsy specimen from a peripheral nodule showed a deep crater invaginating the epidermis containing deeply eosinophilic keratinized cells (Figure 2). Epidermal proliferations buttressed the crater. Plenty of fully keratinized horn pearls were also evident in the sections (Figure 3). No evidence of cellular atypia was seen. The tumor mass was sharply demarcated from the surrounding dermis. There was a moderately dense mononuclear infiltration in the upper dermis around the epidermal proliferations. Abdominal ultrasonography and chest radiography were noncontributory. Based on the clinical evolution with centrifugal expansion in association with central restitution or scarring and histologic features, a diagnosis of keratoacanthoma centrifugum marginatum (KCM) was made.
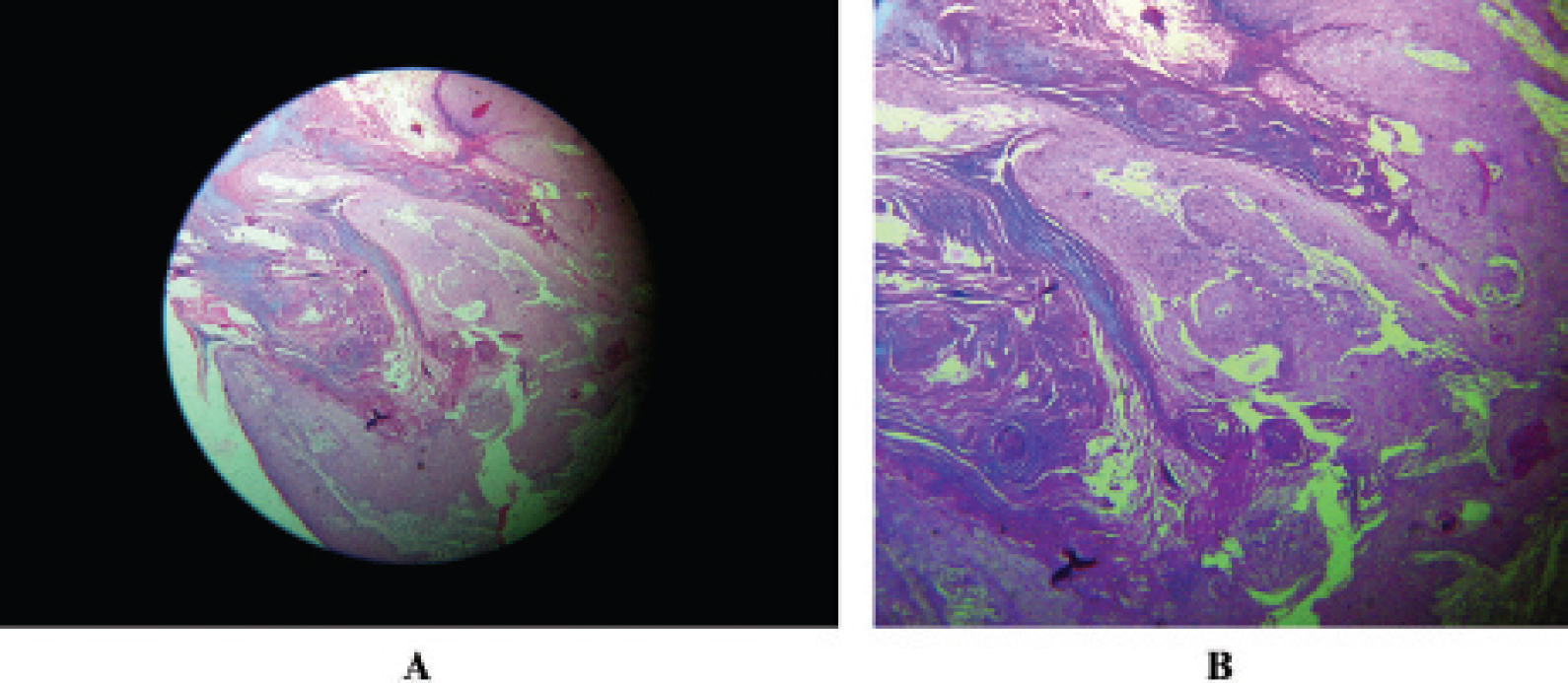
A, A deep crater invaginating the epidermis containing deeply eosinophilic keratinized cells. Epidermal proliferations buttressing the crater are also evident (hematoxylin-eosin stain; ×50 original magnification). B, A deep crater invaginating the epidermis containing deeply eosinophilic keratinized cells. Epidermal proliferations buttressing the crater are also evident (hematoxylin-eosin stain; ×50 original magnification).
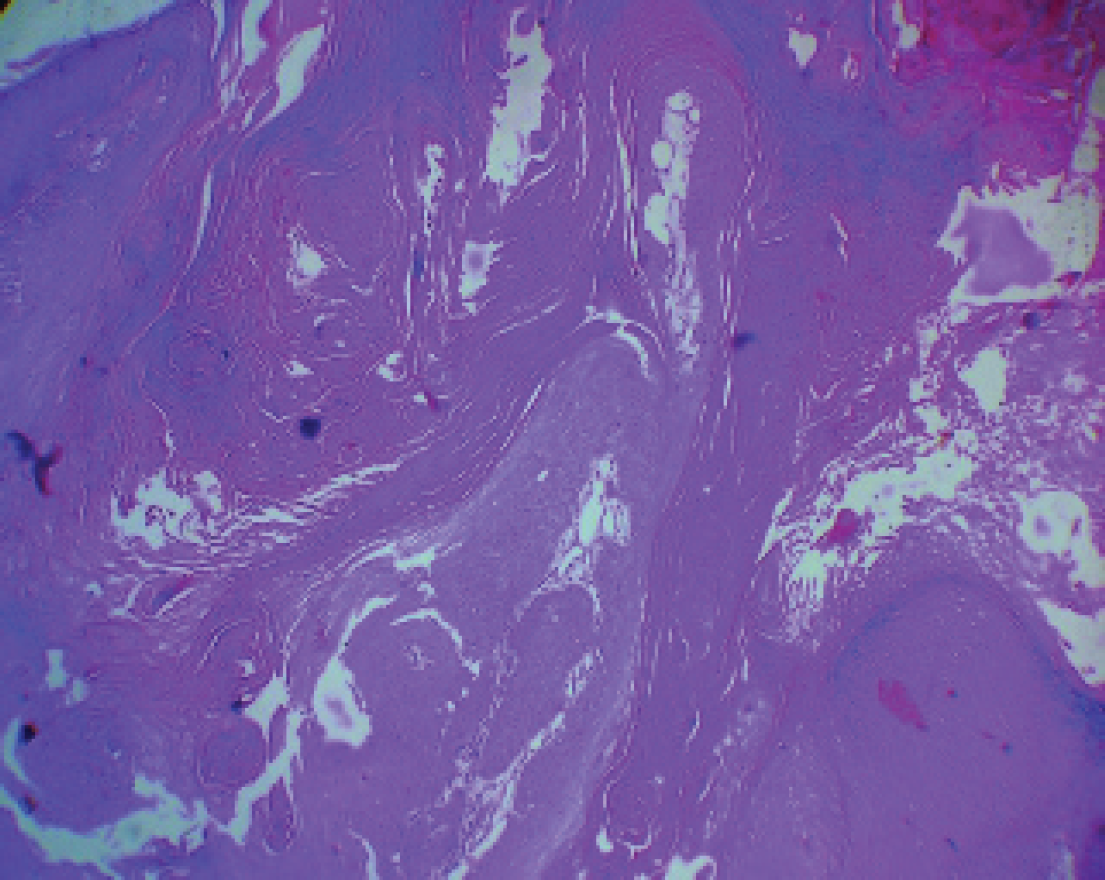
Higher magnification showing a large number of fully keratinized horn pearls (hematoxylin-eosin stain; ×100 original magnification).
The patient was initially treated with systemic isotretinoin (0.5 mg/kg/d) for 1 month, without any improvement. Following this, liquid nitrogen cryotherapy was instituted at three weekly intervals. Each session consisted of two 1-minute freeze cycles applied to the nodular components of the lesions. Lesional crusting was seen a few days after each session. The lesion significantly regressed (Figure 4) within 2½ months, but the patient was subsequently lost to follow-up.

Significant regression of the lesion following cryotherapy.
Keratoacanthomas (KAs) are relatively rare benign epidermal tumors characterized by rapidly growing, firm, symmetric, dome-shaped nodules with keratin-filled craters in their centers and a tendency toward spontaneous regression. 1 KA presents with either solitary or multiple lesions. Approximately 98% of KAs are of the classic, solitary type, mainly occurring in elderly persons on exposed areas. 2 Several variants of KA with multiple lesions and some rare variants of solitary KA, namely, subungual KA, giant KA, and KCM, have been described in the literature. 3 Kurschat and colleagues note that JC Belisario first described the KCM as a separate entity in 1965. 2 KCM is an extremely rare variant of KA, with less than 50 cases reported in the English literature since it was first described. 4 Moreover, KA is uncommon in dark-skinned people. Although the etiopathogenesis of KA is unknown, trauma, human papillomavirus, genetic factors, and immunosuppression have been implicated as etiologic factors. 5 KAs developing on an underlying scar 6 or vitiligo 3 have been described in the literature, but our patient did not have any underlying skin lesion.
KAs typically reach their full size of 1.0 to 2.5 cm within 6 to 8 weeks, followed by spontaneous involution within less than 6 months. 4 Unlike the usual solitary variant of KA, KCM shows no tendency toward spontaneous resolution. Instead, peripheral extension with an elevated, rolled border and atrophy in the center of the lesion is characteristic.3,4 Histologically, KCM is similar to KA, with a central keratin-filled crater, overhanging lips of epithelium, a sharp delineation between the tumor nests and stroma, and a lack of anaplasia and stromal desmoplasia. 4 Histologically, KCM often demonstrates infiltrative behavior, and atypical mitoses may be seen occasionally. Although perineural invasion has been described in the early proliferative stage, the invasions do not adversely influence the biologic behavior and the prognosis. 7
Mohs micrographic surgery has been recommended for large lesions of KCM. 1 In several cases, multiple KAs have been successfully treated with oral retinoid. 1 Our patient declined to undergo any surgical procedure and did not respond to oral retinoid therapy. The lesion, however, responded very well to cryotherapy. We report this case because of its rarity and its responsiveness to cryotherapy in spite of resistance to systemic retinoid.
Footnotes
Acknowledgment
Financial disclosure of authors and reviewers: None reported.