
Abstract
Objective:
On the premise that historical background makes the present more understandable, this review covers the origins of Western dermatology from its Greek and Roman origins through the Middle Ages to the defining moments in the late eighteenth century.
Background and Conclusion:
The development of major European centers at this time became the background for future centers in the eastern United States in the midnineteenth century and, finally, to the West Coast of the United States and Canada by the midtwentieth century.
AS SKIN IS SO OBVIOUS, humans must always have been aware of any obvious disorder. Successful management depends on recognition of the disorder and the availability of a treatment. Where should a history start? Shelley and Crissey nominated Robert Willan as beginning modern dermatology in 1796 when he indicted his predecessors and contemporaries with the following words:
They employ the same terms in very different significations. They also make artificial and often inconsistent arrangements, some reducing all the diseases under two or three genera, while others too studious of amplification, apply new names to different stages of appearance of the same complaint. Those who attempt to theorize on the subject are seldom clear and satisfactory. 1
However, Greek civilization is widely accepted as the forebear of modern Western civilization, and records exist of skin disease from 2,500 years ago. Pusey 2 in 1933 took a longer view than Shelley and Crissey when writing the first modern English history of dermatology 20 years earlier.1,3 A Pusey reviewer, Ravenel, wrote:
The book begins with ancient dermatology, Egypt to Greece, 3000 to 300 B.C. It brings us down through Graeco-Roman, Arabian and medieval dermatology, Rome to the Renaissance, 300 B.C. to 1500 A.D., and so on to the present. Dermatology began to find itself, so to speak, 1750 to 1825, clinical and laboratory dermatology 1800 to 1850. The first phase of modern dermatology in Continental Europe and in Great Britain and the United States is placed from 1850 to 1900. 4
Although considerable information is available on ancient Indian, Chinese, and Egyptian medicine and more specifically Egyptian culture,
5
this is not relevant to Western development. A useful beginning for western dermatology is with the ancient Greek philosopher Anaximander (610–?546
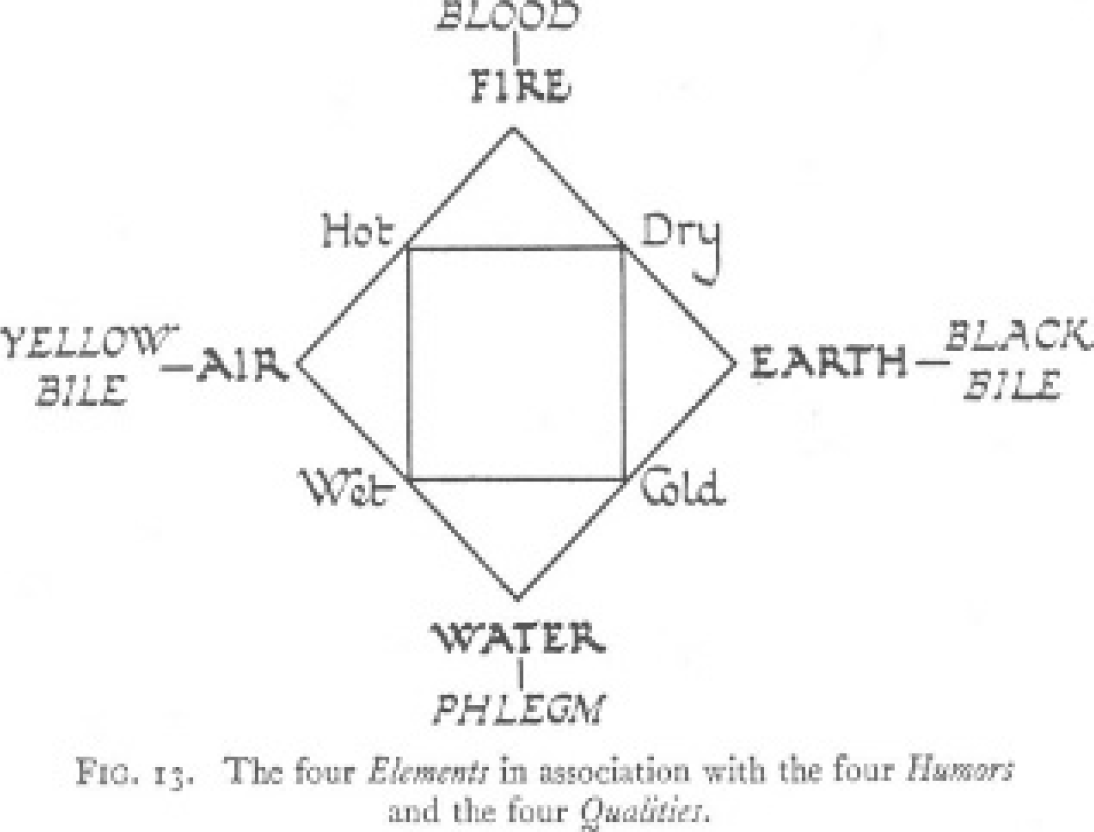
The humors. Reproduced with permission from Singer C. 9
The origins of scientific thought are from such beginnings. Although the Greeks did not have the contemporary Babylonian concept of numbers, they developed an academic learning system derived from Hekademos, (600 BCE) in whose gymnasia meetings for discussion and learning were held. Hekademos's name became corrupted to Ekademos and hence akademia as places of learning. In Platonic thinking phenomena had to be explained, not just accepted.
1200-600 BCE was a period of longstanding empiric medicine based on Temples. The Asklepiads (empiric priest- healers) were the historical ancestors of Hippocrates (460–370
In the next 250 years, observation combined with experience was expressed in the works and teaching of Aristotle (384–322
In a recent publication, Tilles and colleagues reviewed humoralist and diathetic (innate tendency toward a disease) doctrines relating to atopic eczema. 10 Although atopic dermatitis can be treated efficiently, there are conflicting data about the usefulness of bathing, diet regulation, and other therapeutic interventions. The authors commented that these controversies relate in part to the persistence of Hippocratic doctrines in current medical thinking.
As the Greek states waned, the center of medicine moved first to Alexandria (311
The major figure of importance of this period was Galen (c. 129–199
Through his father's direction, Galen was exposed to four philosophical sects: platonism, aristotelianism, epicureanism, and stoicism. The outcome of this was as important as that of the modern precursor of the Renaissance, which was to come another 700 years later. Although not a monotheist in modern terms, he did not believe in the multiple gods of Greek and Roman theology. He was a teleologic thinker seeking causes and outcomes. From his animal and human dissections, he recognized the muscular, nervous, respiratory, urologic, and vascular systems. The blood vessels did not carry air but blood. Here he applied the hippocratic humoral beliefs that blood flowing out of the liver was important in the balance of human health. Health depended on the equilibrium of the four humors: phlegm, black bile, yellow bile, and blood. Pneuma, a subtle component carried by the blood, was somehow responsible for guiding many body processes. Galen went to Rome, where he became physician to Marcus Aurelius. Above all, he was a great anatomist. His descriptive technique and his medical philosophy dominated the medical thinking of the next thousand years.
There is now a gap of almost 800 years. In this time, the Arab world, the Persians, and the Jews kept the flame of medicine flickering.
5
Rhazes of Baghdad (860–932
By this time, the focus of medical learning was moving toward Europe. Rogers of Palermo in 1170
Although historical records of this era, known as the Dark Ages, remain very sparse, Huckbody has provided useful information indicative of the state of medical knowledge at the time.
12
For example, the Venerable Bede (672–755
Signs of the beginning of a new era of scholastic interest, centered mainly on Palermo, appeared in the early thirteenth century. 13 The Romans, Chinese, and Muslims had taboos against the examination of the dead, and the Greeks and Indians cremated the bodies without examination. But the Holy Roman Emperor Frederick II ordered the bodies of executed criminals to be delivered to nearby medical schools. This allowed orderly and objective examination of the human body and gave an enormous stimulus to medical knowledge.
The fifteenth to sixteenth centuries can be viewed as a cauldron in which a brew of ancient philosophy and religious concepts, coupled with technological advances, caused an enormous change of thought. This directed the future course of medicine (Figure 2). 14

Beginning of modern science. Reproduced with permission from Koestler A. 14
The Transition Period
How the observed is interpreted depends on its significance relating to previous experience. Apuleius's (c. 124–?180
Relevant to dermatology are Leonardo da Vinci (1452–1519) and Antonie van Leeuwenhoek (1632–1723). Da Vinci is a hallmark for anatomic description and concurrent technological advances in mechanics and machinery of all types (Figure 3). Vasario (1511–1579), an Italian painter and writer wrote “I have heard it said that he was one of the first who began to illustrate the science of medicine, by the learning of Galen, and to throw true light upon anatomy, up to that time involved

Leonardo and anatomy. 15
in the thick darkness of ignorance.” 15 Pope Clement VI had ordered the bodies of plague victims to be opened and examined. Along with Andreas Vesalius at the start of the Renaissance, da Vinci studied bodies of the dead and recorded the information in extensive notebooks. The arid era of scholastic lull was over, but it took almost 300 more years until a conjunction of individual intellectual powers and related technological advances in the sixteenth and seventeenth centuries allowed the great step forward.
Da Vinci's multifaceted genius is important not only for his precise observation and record but also for his inventiveness in so many fields. European development took about 200 years to absorb and develop all the ideas fermented from his time. The seventeenth century philosopher Descartes' concept of the human body as a machine had a major influence on medical thought. But it took van Leeuwenhoek, with his lifelong enthusiasm for glass lenses, to advance Galileo's lens telescope to a microscope and all that it would reveal. 16
A dramatic change in thinking occurred in this midseventeenth century period. Philosophy in the Plato and Aristotle context focused on nature and its study. Using the new tools that had become available, “natural philosophy” emerged, eventually to become “science” in the way we understand it. This term began to be used in the late seventeenth century. The change was momentous for dermatology, along with many other medical sciences. Instead of a catalogue of isolated observations and cookbook remedies, the lens and the microscope converted skin from a covering bag to a functioning organ that could be logically assessed in its parts.
It took a long time for this new thinking to have an effect on the medicine of the time. For example Brookes's The General Practice of Physic was a popular medical text in 1751. 17 The first paragraph of the chapter “Of the Itch” reads as follows: “The Itch is a cutaneous disease arising from a corruption of a serous lymphatic matter, sometimes attended with mild, obstinate and dangerous Symptoms” (Figure 4). This reflects the hippocratic method, which was dominant to this time. Humoral theory abounds throughout, although sulfur and the resins are found in a number of his prescriptions. The continuing hippocratic influence is seen to the end of the nineteenth century. 18
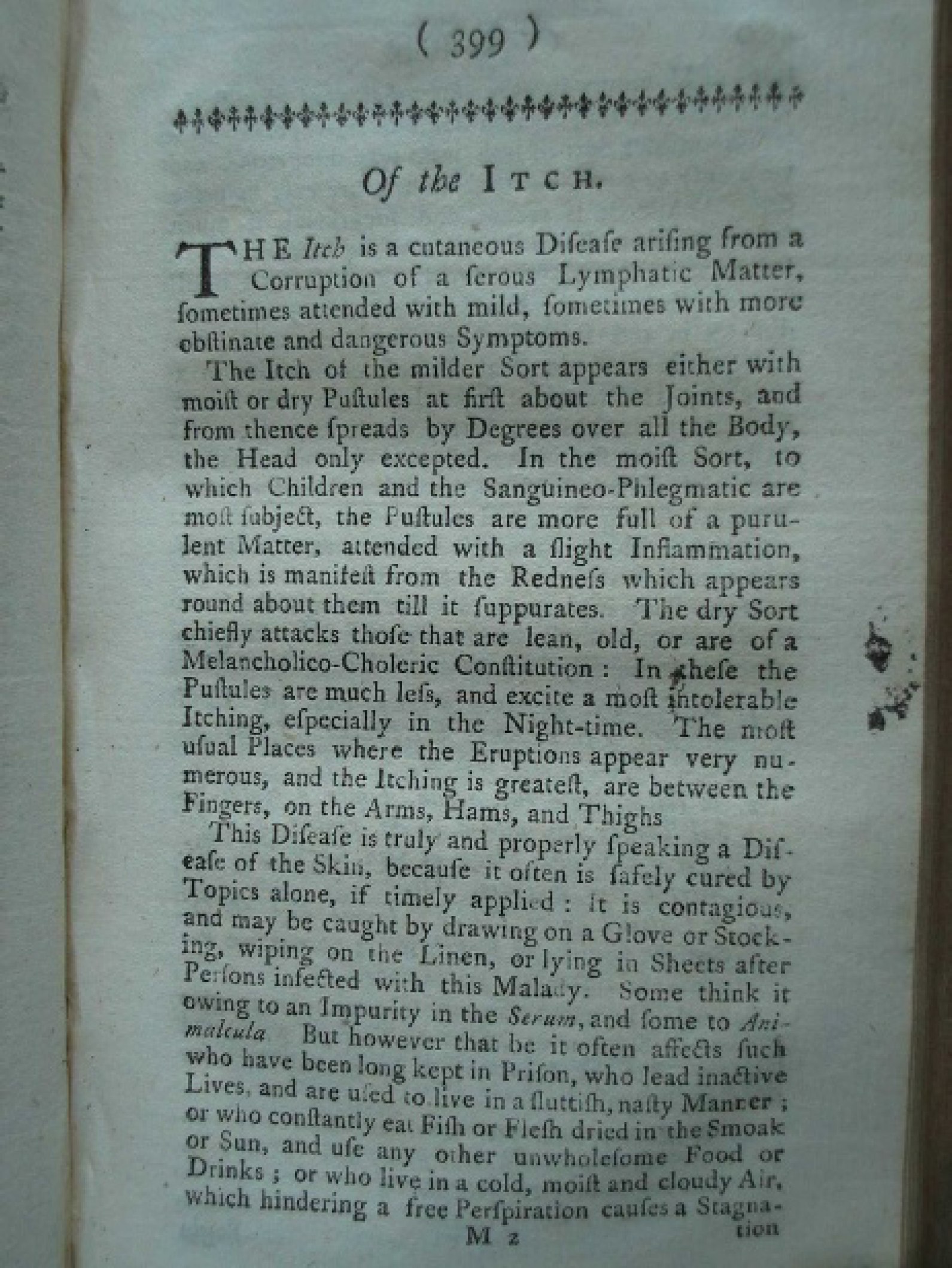
Scabies from Brookes General Practice of Physic, 1751. 17
Transition to the Early Scientific Period
The scientific process demands an orderly method of thought no matter what discipline. Linnaeus (Carl Linné) (1707–1778) of Sweden, Charles Darwin's inspiration, provided the linnean method. Essentially, it was the basic binomial system. In the binomial system every species is identified by its genus and species name, for example, Felix leo for lion and Homo sapiens for man. Many contemporary scholars had tried to classify plants but failed. Ray of England, Tournefort of Paris, and Rivinus of Leipzig, all seventeenth-century botanists, had attempted to develop systems for the classification of the burgeoning recognition of plants, without success. 16 However, Linnaeus's Systema naturae encompassed Class, order, genus, species, and variety and was applied to 15,000 species. His discipline applied strict definitions and was eventually adopted for the whole biologic and mineral world.
At this time, the earliest dermatology texts of significance in the Western world were those of Mercurialis of Venice (1530–1606) (Latin), Daniel Turner of London (1667–1741) (English), and Anne-Charles Lorry of Paris (1726–1783) (Latin). Mercurialis was educated in Greek and philosophy.19,20 He studied medicine at the University of Padua when it was a vibrant center of scholarship and eventually succeeded to its chair of medicine. He was widely respected for his voluminous knowledge of Greek, Latin, and Arabic writings in the 2,000-year span from Hippocrates. 18 Between 1552 and 1601, he wrote 12 publications, not all related to dermatology (Figure 5 and Figure 6). Paulus Aicardius, one of his pupils, collected and translated Mercurialis's lectures. The authorities Mercurialis quoted give insight into the state of medicine and dermatology of the time. 16 This is the beginning of a classification built either on appearance or specific diagnoses. Treatment is based on
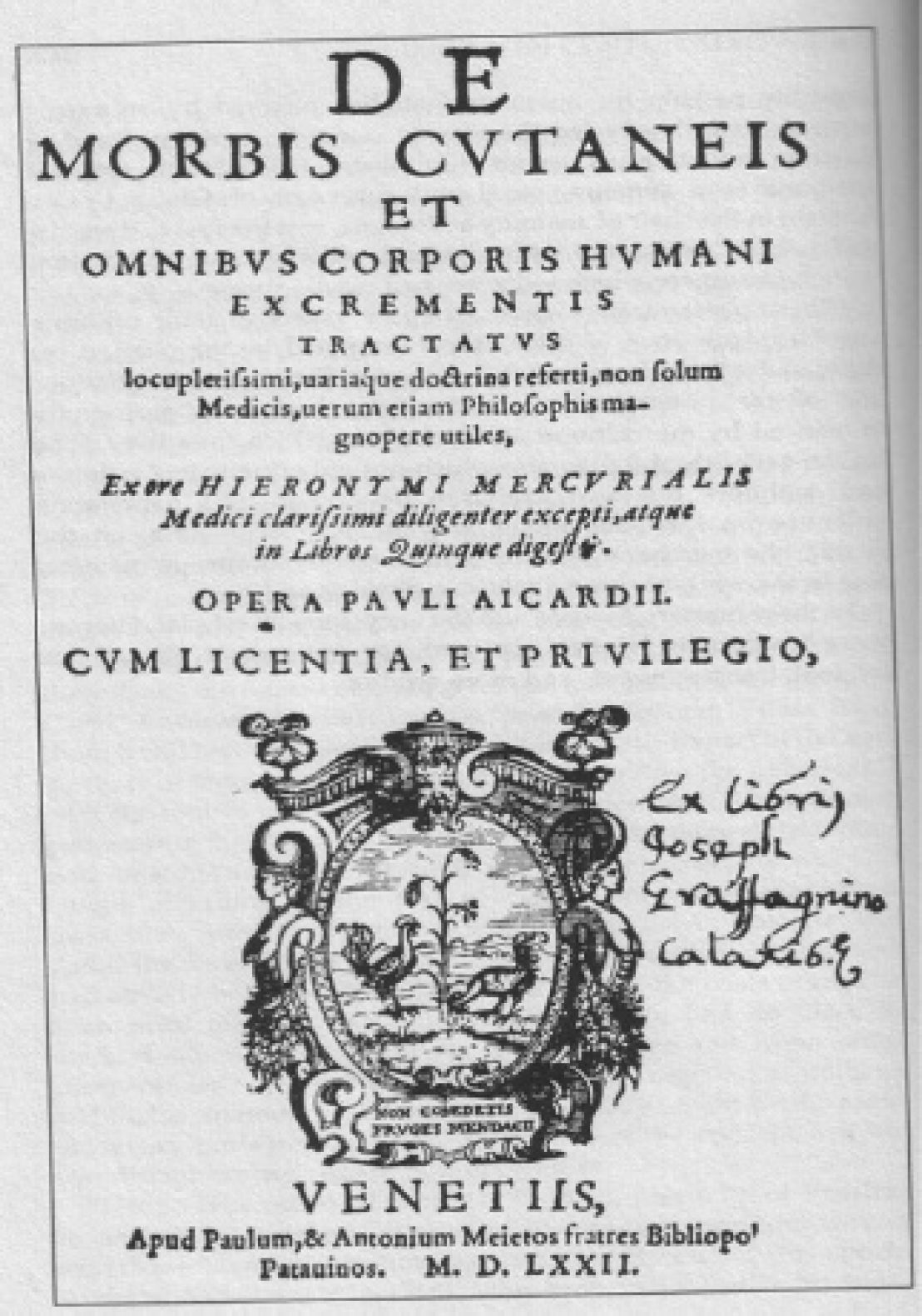
Frontispiece for Mercurialis's, 1703. On Diseases of the Skin and All Excrements of the Human Body, with copious references to numerous and diverse doctrines, useful not only to physicians but also to philosophers, carefully compiled from the words of the most illustrious physician, Hieronymous Merculiaris, and arranged in five books by Paulus Aicardius, with authorization and approval. Venice, Paulus and Antonius Meitus Brothers, Publishers, 1572.
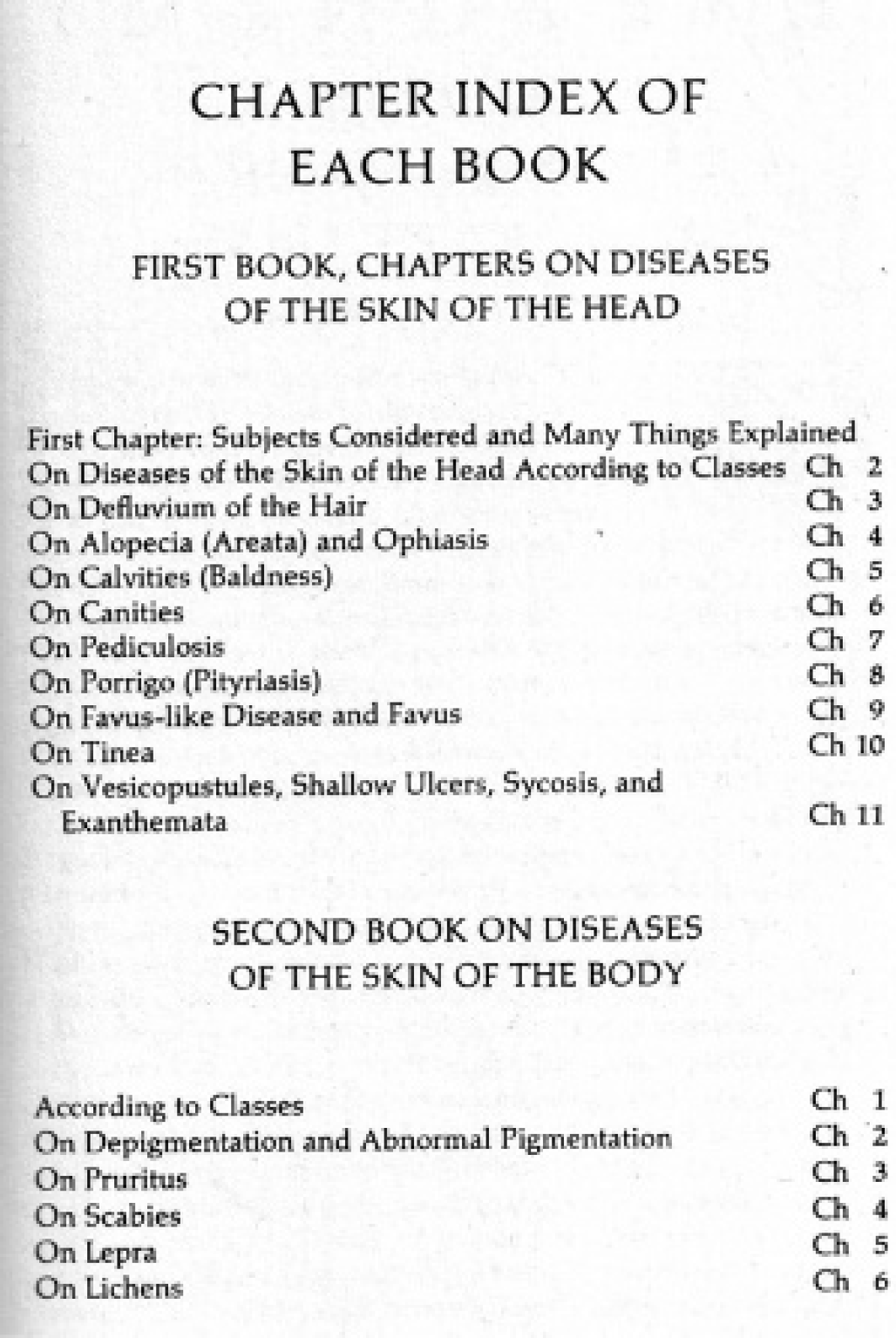
Mercurialis's classification of skin diseases. Reproduced with permission from Sutton RL Jr. 19
quotations from the ancient authorities and consists of basic chemicals such as sulfur and arsenic, liquids such as vinegar, and a wide range of botanicals.
The next of the trio of protodermatologists is Daniel Turner. Turner's 1714 De Morbis Cutaneis: A Treatise of Diseases Incident to the Skin 21 was the first work in the English vernacular solely devoted to skin disease. Wilson noted good evidence of the first controlled trial from Turner's writings. 22 He writes about the skin being permeable to applied agents and gives differential diagnosis.
Lorry, the third of the trio, wrote a massive work in which skin was treated as a living organ rather than a body enclosure. 23 Essentially a listing of diseases, this work marked the transition from medieval thought to the Enlightenment.
These three authors heralded the modern period to follow in some 20 years. Plenck (1738–1807), Lorry's Austrian contemporary, was a physician, scholar, and probably a botanist (the dates and record vary a little). 24 He broke away from current practice and produced his own classification (Figure 7). Because of Lorry's prominence in France, Plenck must have been aware of his work. There are still some inconsistencies in his classification (see Figure 7), but the forerunner of future thought was by now clearly established.
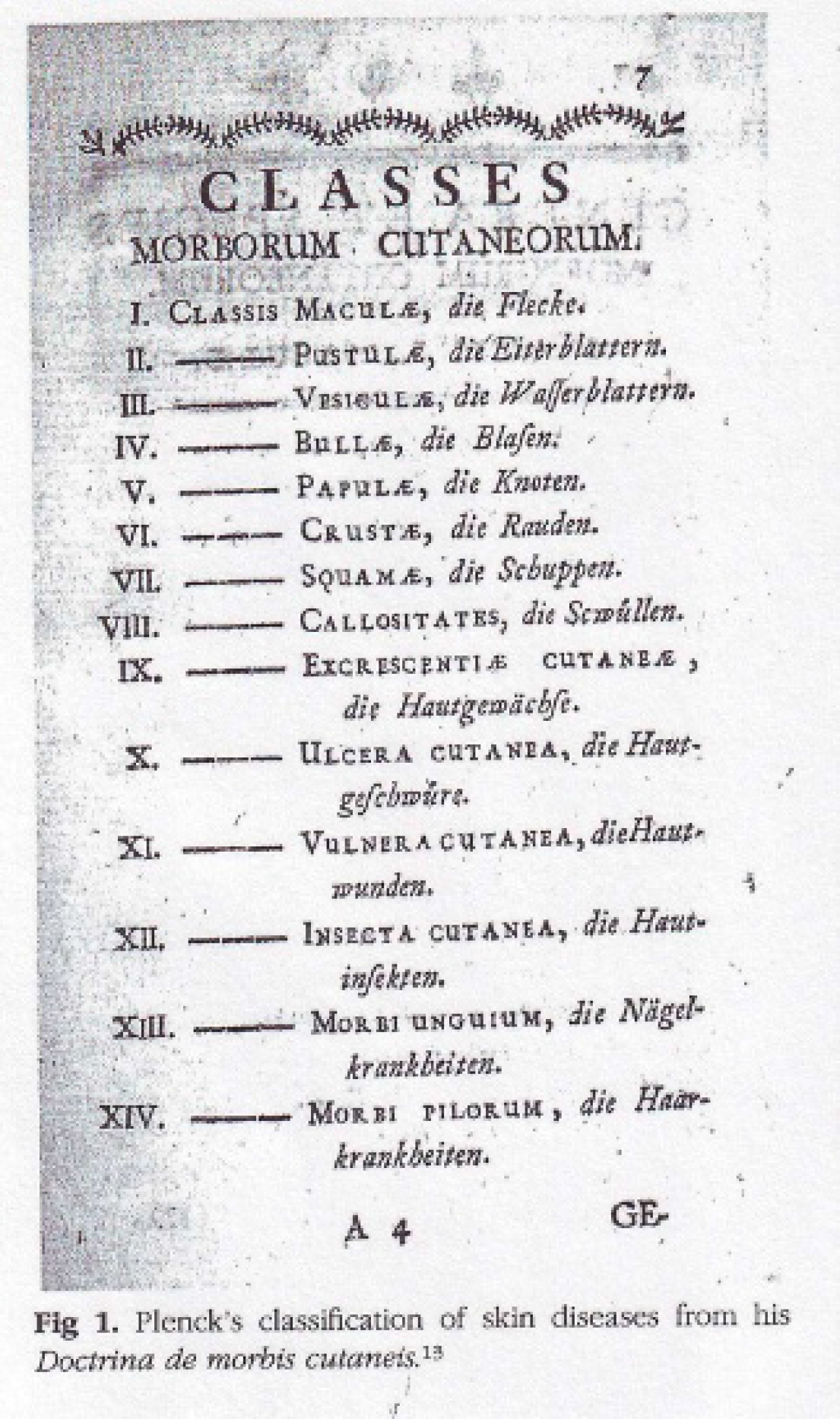
Plenck's classification of skin diseases, 1776. 24
Origin of the Modern Period
The beginning of modern dermatology came in due course 20 years later. 25 Willan refined Plenck. Considering his travel to major academic centers at that time, and his opinion that he had not seen sufficient dermatologic patients by the time he published his classification (Figure 8), he had to have been much influenced by Plenck. 26
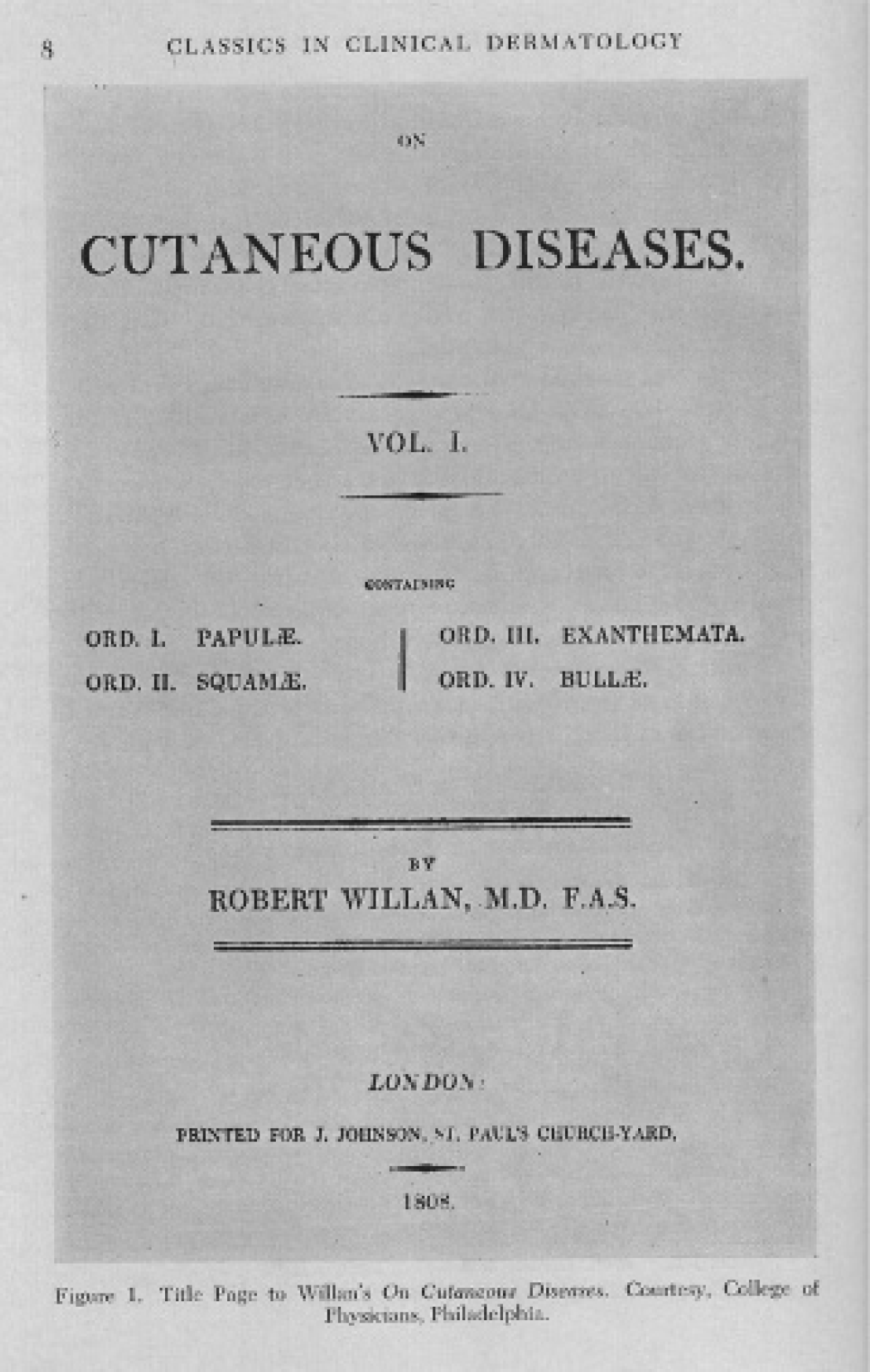
Willan's classification of skin diseases, 1808. 27
Robert Willan was born November 12, 1757, near Sedbergh, Yorkshire, England. He died April 7, 1812, in Madeira, where his grave is found. He is regarded as the founder of dermatology as a medical specialty. After receiving his medical degree from the University of Edinburgh in 1780, he practiced medicine in Darlington, northeast England, from 1781. He moved to London in 1783 to the new Carey Street Public Dispensary, teaching with Thomas Bateman. He remained there as a physician until 1803 and was recognized as a Fellow of the Royal Society (FRS) in 1809. 1
The crucial step that Willan made was the application of the linnean method to identification. He defined a limited number of basic physical characteristics and used them to classify and identify skin diseases. We recognize them as the primary and secondary physical signs. The basic hippocratic principle of observation as a tool of management of the sick remained intact. Willan and Bateman, working together, provided the first attempt to classify skin diseases from an anatomic standpoint. Willan was awarded the Fothergillian Medal in 1790 from the Medical Society of London for this work. In 1798, he described the occupational disease he named psoriasis diffusa, which affected the hands and arms of bakers, and in 1799, he first described the exanthematous rash of childhood known as erythema infectiosum.
Willan's 1808 book, On Cutaneous Diseases, is a landmark in the history of dermatology and in medical illustration. 27 It contains the first use of the word “lupus” to describe cutaneous tuberculosis. Shelley and Crissey have noted that although there were many accounts of conditions such as (possibly) psoriasis, pemphigus, and ichthyosis known since antiquity, they are of limited value because of carelessness in the use of terms. 1 Willan became the founder of modern Western dermatology by his insistence that terms used should have proper definitions; there should be organized orders of diseases classified by points in common; such orders should have specific names, and there should be a mode of treatment for each disease. This is the beginning of the Western dermatology we inherited and now practice.
At this time, there was divergence from the French method of practice. Jean Louis Alibert's (1768–1837) base of dermatologic practice was in Hôspital Saint-Louis, where he had over 400 dermatologic beds. After the Revolution, in 1794, hospitals, which were previously shelters for the homeless, now became places where scientific medicine could be practiced. Alibert continued the tradition of the school of Sydenham, which followed the inherited hippocratic traditions. The English philosopher Locke and later Condillac, the French philosopher, developed a system of sensualist philosophy that is based on only what the senses can perceive. Pinel, regarded as the founder of modern psychiatric practice, brought this philosophy to Hôspital Saint-Louis, and it influenced Alibert's method. The day-to-day observation of inpatients led to a different focus than that of the more voluminous outpatient visits in London. To classify skin disease, single criteria were not taken into account.
Choosing a dermatological hero for the millennium, Wallach selected Alibert. 28
Alibert believed that to classify skin diseases adequately, or rather to group them together, one must not take into account a single criterion, but many. Cause, when it is known; course, as it can be better observed in hospitalized patients; duration and appearance, which may be assimilated to the anatomy of the lesions and, response to therapy (abstracted from reference 28).
This was called the natural method—the classic method of hippocratic medicine.
Laurent Theodore Biett (1781–1840), a pupil and colleague of Alibert, had visited Bateman in London and undoubtedly made Willan aware of the current French approach. Biett had great regard for Alibert, but after visiting Willan and Bateman in their London outpatient practice, he saw the practicality of Willan's approach, which was based on the linnean method. However, even now, when the Willan method is used almost universally, there are still some conditions that cannot be fully classified using this approach. What made Alibert famous also made him fail. Unfortunately it was not possible to classify all skin disease on a logical Linnean basis and 200 years later, it is still not possible. 29
Early Modern Period
Europe's population grew rapidly throughout the eighteenth century. Roadways improved, and travel was much easier. Related to this, academic centers expanded greatly. By the beginning of the nineteenth century, dermatologic centers were founded in Italy and Germany. Alphêe Cazenave 30 (1795–1877) continued his teacher Biett's “Willan” method in Paris. At the same time in 1826, Pierre Francois Rayer (1793–1867) in Paris published the first attempt to relate skin diseases to pathology under the title Traité théorique et pratique des maladiese la peau. 31 Ferdinand Von Hebra (1816–1880) headed the predominant dermatologic center in Vienna, where he published his authoritative system and textbook of skin diseases based on pathology (1845 and 1860). Radcliffe Crocker's (1845–1909) highly influential textbook appeared in London and remained predominant in the English language for the next era. 33
In the next period, Jonathan Hutchinson (1828–1913) was the English polymath representative of the great learning tradition of nineteenth-century England. He was basically a surgeon, although he belonged to many different medical societies of special disciplinary interests. His influence in dermatology remains today with the emphasis on internal medicine in British dermatology.
North America
United States
North American dermatology developed along different lines, based initially on private office practice in the entrepreneurial spirit of the nineteenth century. Triggered by industrialization and technological advances, urban centers expanded rapidly, labor became specialized, and universal education produced an increasingly skilled population. Dermatology grew rapidly at this time, accompanied by the rise of outstanding medical schools in major cities in the east of the United States. The western United States and Canada would have to wait until the twentieth century for similar centers to be established.
Paul Bechet has left an invaluable record of this time in his paper, “The Early History of American Dermatology.” 34 He named November 27, 1801, as the beginning of scientific dermatology when the old Hôpital Saint-Louis in Paris was officially dedicated to the treatment of skin disease, with Alibert as its head. He wrote proudly that it was only 100 years later that dermatology in America had attained a commanding position in the medical world. Up to October 1940, there were four national bodies, six sectional societies, and 11 state and 20 local societies with an active and enthusiastic membership; New York alone supported 6 of those. Bechet paid tribute to a small band of devoted pioneers in this chosen subfield. They had to deal with a tangled skein of dermatologic symptoms and classification, relying on exhaustive clinical notes and analytic and photographic minds. All of this led to the development of rapid “sight diagnosis,” which he termed a sixth dermatologic sense (without clarifying the other five!).
Bechet identified the start of American dermatology as in New York in June 1836 with the opening of the Broome Street Infirmary under the direction of Henry Daggett Bulkley. Bulkley (1804–1872) translated Cazenave and Schedel's Manual of Diseases of the Skin in 1845 and edited an American edition of Gregory's Eruptive Fevers in 1851. This was followed by the first complete American textbook on dermatology written by Noah Worcester 35 (1812–1847). The New York Dermatological Society was founded in 1869 in Bulkley's home.
Noah Worcester had traveled to Paris where he came under the influence of the Hôspital Saint-Louis. 36 He was among the earliest lecturers in Dermatology in the nineteenth century. Prior to his text, only translations of leading European authorities had been used. In particular, Worcester stressed the importance of pathology.
The next year, the American Journal of Dermatology and Syphilology, edited by M.H. Henry, was published. Dermatology and Syphilology would remain together until 1954, when the last AMA Archives of that name was succeeded by the current Archives of Dermatology. Penicillin had spelled syphilis's doom as a subject of major dermatologic interest.
Later in the century, Louis Adolphus Duhring (1845–1913) was the first American dermatologist with international fame. His textbook and atlas, published in Philadelphia 1876 and 1877, had considerable impact. Although chiefly remembered for his work leading to the diagnosis of dermatitis herpetiformis, his texts were translated into French, Russian, and Italian.1,37
The first independent chair in dermatology was established at Harvard in 1871. James Clarke White (1833–1916) headed the newly created Department for Skin Diseases at the Massachusetts General Hospital for 33 years. 38 He was strongly influenced by the Vienna School and, chiefly, Ferdinand Von Hebra, the outstanding dermatologist of his time.
Another individual who was influenced by Von Hebra was George Henry Fox (1846–1937). Fox trained in Pennsylvania, where he had exposure to the local dermatology clinics. 39 He later studied in Vienna under Ferdinand Von Hebra and then in Paris with their different teaching methods. Fox opened his practice in New York City in the fall of 1873, and although his was a general practice, dermatology was his chief interest. He is chiefly recognized for the founding of dermatology in New York City, taking part in the opening of the New York Skin and Cancer Hospital. Dermatology and urology were commonly associated specialties in one department, but they diverged at this time. Fox was appointed professor at the New York Postgraduate Medical School and Hospital when it was founded in 1882. His impact as a teacher was wide.
Growth of American Societies and Centers
Various national societies based on the major dermatology hospitals were formed late in the nineteenth century. The American Dermatological Association (ADA) was formed in 1886. It is of interest that all of the 13 men who were present came from the eastern United States. 40 Prior to that, informal meetings were held by the heads of each center or as part of major general medical meetings.
The end of the nineteenth century and the beginning of the twentieth century saw the development of prominent dermatology centers in the central and western United States. The health needs of the population often led to the establishment of new departments. An example is Cleveland, 41 which had a smallpox epidemic in the early twentieth century. Appropriate support services such as laboratories and physicians with expertise followed.
Canadian Dermatology and Its Association with American Dermatology
James Elliot Graham (1847–1899) has been identified as Canada's first dermatologist. His career is typical of the early pioneers of Canadian dermatology. Conscientious and capable doctors kept up to date by travel to the larger medical centers in the United States and Europe. 42 Graham became a member of the ADA, to which he presented papers. Canadians became associated with the British Association of Dermatology in 1921. The Canadian Dermatology Association was formed in 1925 and the American Academy of Dermatology, to which many Canadians belonged, formed in 1938. Regional societies began to appear in the 1920s, and their proceedings have appeared in a variety of journals. The early years of Canadian dermatology in the twentieth century up to the end of World War II have been well documented with brief biographies of the influential dermatologists who provided the clinical backbone of future academic training and research centers. 43 Vignettes of the personalities and organizations involved in the next era of Canadian dermatology moving into the twenty-first century have been published.44,45
A major influence in the rise to dominance of North American dermatology in the midtwentieth century was the rise of Nazism in Europe in the late 1920s after World War I. This resulted in the emigration and influence of large numbers of highly qualified and experienced Jewish doctors and scientists in many fields. They brought European scholarship with them. Dermatology has benefited greatly from this. American dermatologists of major note who have had major Canadian impact include Marion B. Sulzberger, Walter Shelley, T.B. Fitzpatrick, A.M. Kligman, A.A. Fisher (contact dermatitis), Alvin Jacobs (founder of pediatric dermatology), Walter F. Lever, and Bernard Ackerman (histopathology).
World War II and Subsequent Development
World War II saw major changes occurring. Technological innovation developed in the war provided new tools for research and the development of therapeutics. Research was followed by new concepts of disease, the recognition of new conditions, and new treatments. The sulfonamides had been introduced in the 1930s and then penicillin at the end of the war. Topical steroids were the next introduction. This caused a major change in the delivery of care. Large, specialized inpatient departments were reduced and outpatient departments with specialized subunits appeared.
Major university departments and divisions of dermatology were opened in the Midwest and on the west coast of the United States. In Canada, Montreal and Toronto had been the major centers since the 1920s. Now Vancouver on the west coast has been established, followed by Ottawa, the major prairie centers, Quebec, and, on the east coast, Halifax. Early in the twenty-first century, antiviral medications, the retinoids, synthetic biologics, cosmetic and dermatologic surgery, and refined dermoscopy are all recent introductions.
Historical Stages in the Development of Dermatology
Throughout the whole history of dermatology, recognition of form and structure has been followed by the recognition of function and its mechanism. Initially, the practice of dermatology was the identification of distinct disorders, each with its various treatments. Pathology added a second dimension in the 1870s. Biochemistry added yet another dimension in the first half of the twentieth century, and the latter half of the twentieth century saw the rise of immunology. Molecular biology, as a new science, led to the recognition of the genome and many novel synthetic treatments. The terminology of dermatology changed with each development. Earlier classifications have been revamped or replaced in entirety. Recognition that scientific research has been the key to each step has made governments, universities, national and regional societies, and industry all contribute to this end.
To the ancients, heaven was as light in the sky. The technology of glass manufacture led to the telescope and a new view of the heavens. Radiotelescopes and other technologies have revealed new objects changing our insight and the almost unbelievable concept that space is not empty. As demonstrated in this review, concepts and terminology are always changing. It will be interesting to revisit this topic in 50 years' time.
Footnotes
Acknowledgments
Manuscript criticism by Dr. Laura Finlayson is acknowledged.
Financial disclosure of author and reviewers: None reported.