
Abstract
Background:
Syringomas are benign neoplasms of eccrine origin. A clinical variant is eruptive syringomas, which presents as firm, smooth, yellow to pigmented papules that appear as successive crops on the neck, axillae, chest, abdomen, and/or periumbilical region. To our knowledge, there are only 10 published reports of familial eruptive syringomas. Herein we describe the eleventh report of familial eruptive syringomas, review the literature on this unusual presentation, and suggest a novel classification of familial syringomas based on our literature review.
Observations:
We report two cases of eruptive syringoma within a family. Eruptive syringomas were widely distributed on the trunk of a healthy 16-year-old female and her 19-year-old brother. Both the 19-year-old man and his mother also had infraorbital syringomas.
Conclusion:
Familial eruptive syringomas are a rare clinical entity that is likely autosomal dominantly inherited. Future reports of this unusual condition may provide further insight into the etiology of familial syringomas, and genetic analysis of cases may enable the causative gene mutation to be determined.
Familial cases of syringomas can be localized, often in the periorbital area, which is the most common location for multiple syringomas. A clinical variant of this localized type of familial syringomas is cases reported to present with milia-like lesions. There are also reports of patients with familial syringomas in which eruptive syringomas occurred in one family member, whereas at least one family member only had localized periorbital syringomas. Familial eruptive syringomas in two or more family members are even more unusual than familial localized cases. There are rare cases of familial eruptive syringomas in at least two family members and one or more family members with localized periorbital syringomas.
To our knowledge, there are only 10 previously published case reports of familial eruptive syringomas.3,,,,,,,,–12 The inheritance pattern is likely to be autosomal dominant based on published case reports. We describe a new classification of familial syringomas and the eleventh report of familial eruptive syringomas. Our two siblings had eruptive syringomas, and one of them also had periorbital syringomas. Their mother had only localized periorbital syringomas. This would be classified as type 8 familial syringomas according to our new classification.
Case Report
A healthy, 16-year-old female of Asian descent presented with a 2- to 3-year history of asymptomatic lesions on her axillae and abdomen. She denied the use of medications or dietary supplements and previous diseases. On examination, the patient had slightly yellow-pigmented papules in her axillae (Figure 1) and flesh-colored papules on her abdomen.

Familial eruptive syringomas. Multiple pigmented papules on the left flank of a 16-year-old girl.
Our first patient's 19-year-old brother had a similar asymptomatic condition for 4 years. He was not on any medications and was otherwise well. On examination, there were pigmented papules on his arms, axillae, abdomen, and groin (Figure 2). In addition, he had several infraorbital flesh-colored papules.

Familial eruptive syringomas. Pigmented papules in the periumbilical area and suprapubically in the girl's 19-year-old brother.
The mother of these teenagers also had small, flesh-colored papules that were located only in her infraorbital region. The father was not available for examination.
Skin biopsies were performed of lesions on the sister and brother's abdomens. Hematoxylin and eosin (H&E) staining revealed small, “comma-shaped,” duct-like structures and strands of epithelial cells with pale cytoplasms associated with fibrotic stroma within the upper portion of the dermis of both siblings' biopsies (Figure 3). This histopathologic pattern is typical of syringomas.
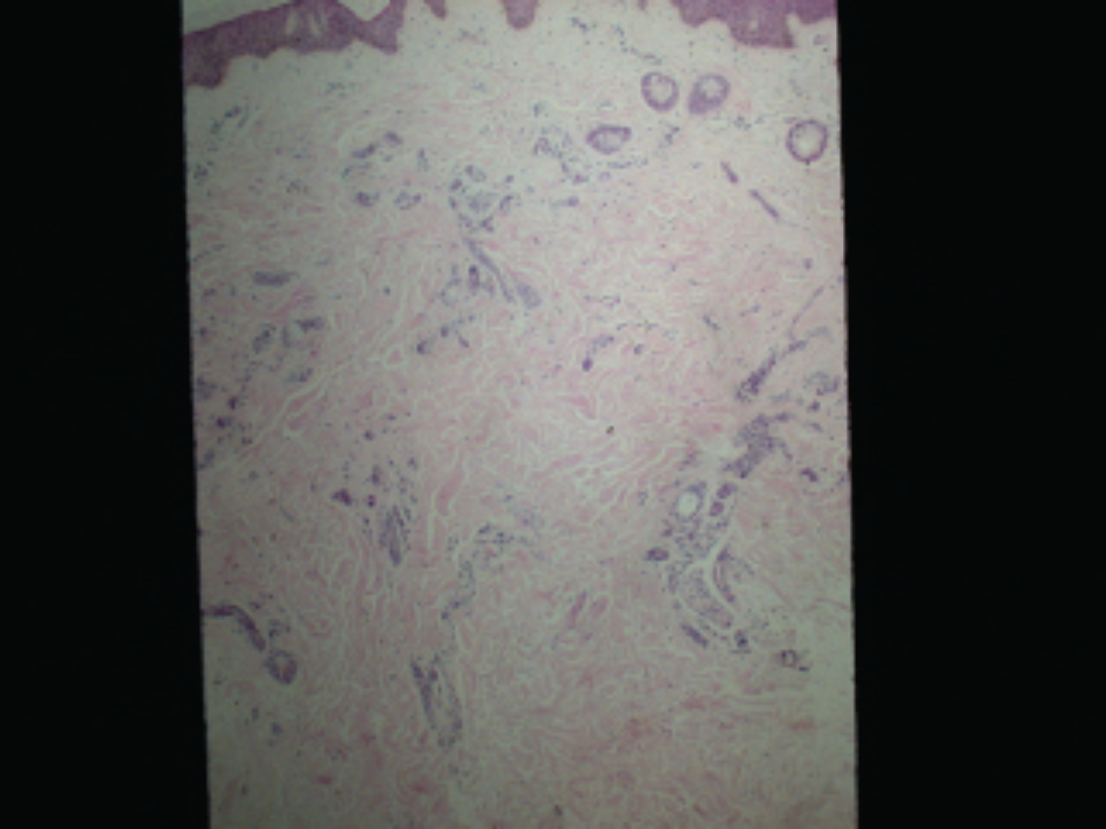
Eruptive syringoma histology (hematoxylin-eosin stain; × 40 original magnification). Small, comma-shaped, duct-like structures and strands of epithelial cells with pale cytoplasm are seen in the upper dermis, associated with a fibrotic stroma. The histologic appearance is typical of a syringoma.
Discussion
Eruptive syringomas were first described in 1887 by Jacquet and Darier. 13 Firm, flesh-colored to yellow papules appear in large numbers and in crops on affected persons' anterior chest, neck, axillae, and trunk during childhood and puberty.1,3 There are only 10 publications in the medical literature that describe this clinical entity affecting people within the same family based on our literature review using the following search terms: “familial eruptive syringomas,” “hereditary eruptive syringomas,” “familial generalized syringomas,” “hereditary generalized syringomas,” and “generalized eruptive syringomas.” 3,,,,,,,,–12 Table 1 describes the reports of familial eruptive syringomas that have appeared in the literature.
Case Reports of Familial Eruptive Syringomas
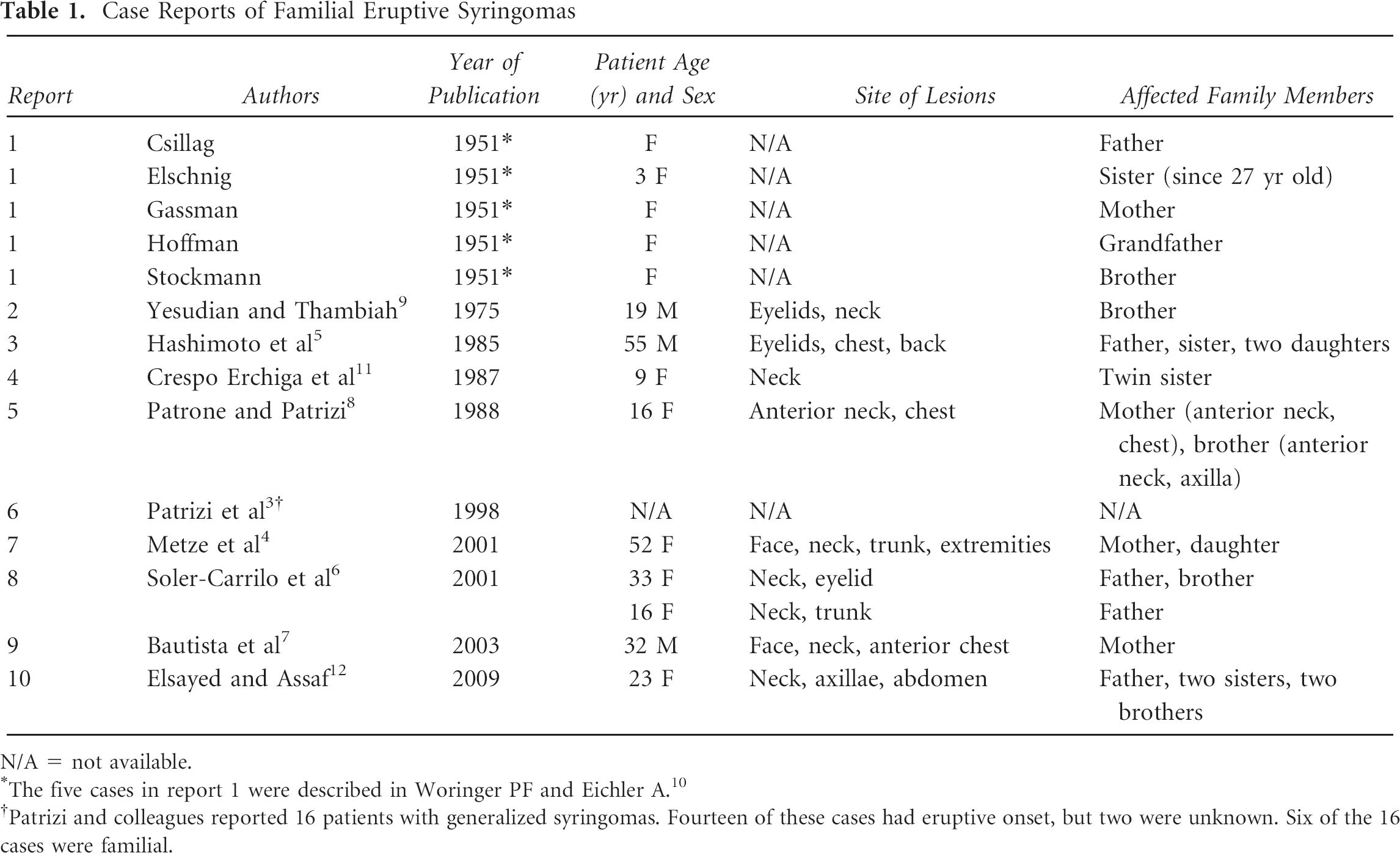
N/A 5 not available.
The five cases in report 1 were described in Woringer PF and Eichler A. 10
Patrizi and colleagues reported 16 patients with generalized syringomas. Fourteen of these cases had eruptive onset, but two were unknown. Six of the 16 cases were familial.
H&E staining of skin biopsies of syringomas demonstrates dilated, cystic eccrine ducts in the dermis.1,3,5 The majority of these sweat ducts have characteristic commalike tails, which gives them a tadpole shape. There are also nests of epithelial cells that are commonly surrounded by collagen bundles in the dermis.
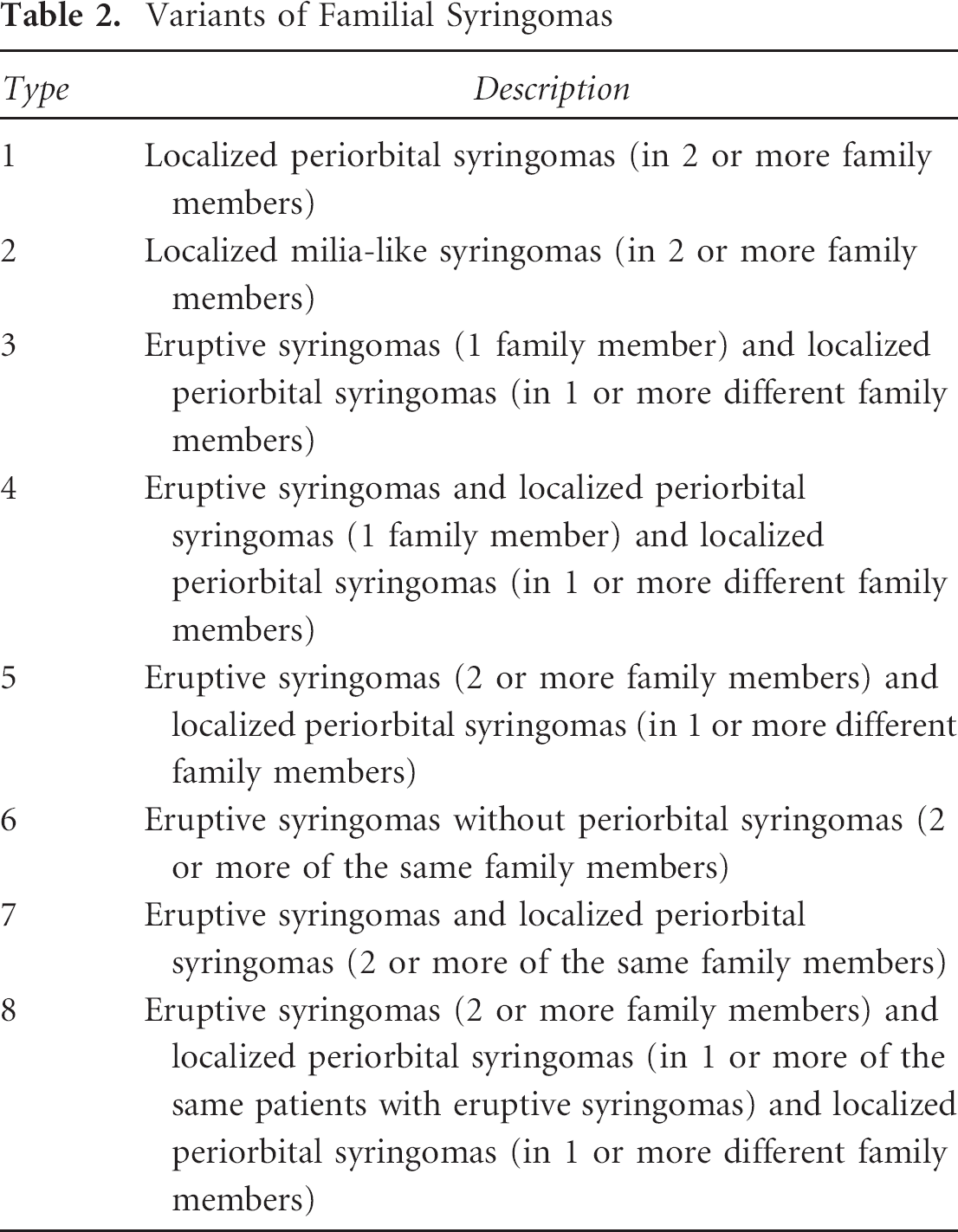
Familial cases of syringomas can be localized, usually in the periorbital area, as it is the most common location for multiple syringomas (type 1).1,4,5,14,15 A clinical variant of this localized type of familial syringomas is cases reported to present with milia-like lesions (type 2).15,16 There are also reports of patients with familial syringomas in which eruptive syringomas occurred in one family member, whereas at least one different family member had only localized periorbital syringomas (type 3).5,17 Familial eruptive syringomas in two or more family members3,,,,,,,,–12 are even more unusual than familial localized cases. Some of these patients have eruptive syringomas without periorbital syringomas (type 6),4,8 whereas other families have eruptive and periorbital syringomas in the same patients (type 7).6,7,9 There are rare cases of familial eruptive syringomas in multiple family members and a minimum of one different family member with only localized periorbital syringomas (type 5). 11
Finally, there are rare reports of multiple family members with eruptive syringomas who may also have localized periorbital syringomas and different family members with localized periorbital syringomas (type 8). 5 Our newly described case would also fit under type 8. Table 2 describes this new classification of familial syringomas.
Variants of Familial Syringomas
The pathogenesis of familial eruptive syringomas is controversial. There are three popular theories of how these lesions develop. The most widely accepted theory is that syringomas are benign neoplasms derived from the intraepidermal portion of eccrine ducts.1,5 Hashimoto and colleagues suggested that eruptive syringomas form by eccrine germ–like budding from the epidermis. 5 They used antibody staining with monoclonal antikeratin antibodies EKH4 and EKH6 to show that syringomas originate from the basal layers of the epidermis and eccrine secretory and ductal structures, respectively.
However, syringomas demonstrate a scant amount of proliferation, which challenges the theory of these lesions having a neoplastic origin. Recently, Guitart and colleagues hypothesized that eruptive syringomas are the result of a hyperplastic response of eccrine ducts to an inflammatory reaction. 18 They observed that syringomatous changes develop in nonneoplastic cutaneous disorders such as alopecia areata, melanocytic nevi, and prurigo nodularis. Furthermore, there are several reported cases of maculo-papular or eczematous eruptions preceding the formation of syringomatous lesions. 1
The third theory proposes that syringomas may be the result of a localized or generalized hamartomatous process in cases where there is a familial history of eruptive lesions. Hamartomas composed of embryonic pluripotent cells may precede the development of syringomas. 18 This hypothesis is based on Hashimoto and colleagues' observation that there is budding of eccrine germ cells from the epidermis overlying syringomatous lesions.
There are many different potential treatments described for syringomas, including topical retinoids, lasers, electro-coagulation, and monoclonal anti–eccrine gland antibodies.17,19,20 However, no single modality has been proven to be a consistently effective treatment.
Eruptive syringoma is a unique clinical entity with controversy surrounding its pathogenesis. Familial eruptive syringomas is even rarer and likely autosomal dominantly inherited. Recently, Wu and Lee reported linkage of autosomal dominant multiple syringomas confined to the palpebral area to a locus on chromosome 16q22. 21 The genetic basis of eruptive syringomas is currently unknown. Future reports of this unusual condition may provide further insight into the etiology of eruptive syringomas, and it is hoped that genetic analysis of cases may enable the gene mutation to be determined.
Footnotes
Acknowledgments
Sarah Sy, Faculty of Medicine, University of Calgary, assisted with reference translation.
Financial disclosure of authors and reviewers: None reported.