
Abstract
Background:
Laser therapy is a rapidly expanding new treatment modality for onychomycosis.
Objective:
To review current and prospective laser systems for the treatment of onychomycosis.
Method:
We searched the PubMed database, the Food and Drug Administration 510(k) database, ClinicalTrials.gov, and Google Scholar for in vitro studies, peer-reviewed clinical trials, manufacturers' white papers, and registered clinical trials of laser systems indicated for the treatment of onychomycosis. All published clinical trials were assessed on a 20-point methodological quality scale.
Results:
We identified three basic science articles, five peer-reviewed articles, three white papers, and four pending clinical trials, as well as numerous gray literature documents. The overall methodological score for the clinical trials was 9.1 ± 1.1, with peer-reviewed studies showing a higher score (9.8 ± 1.5) than white papers (7.5 ± 0.7). We also identified 11 commercial laser device systems of varying global availability.
Conclusion:
Laser therapy has been tested and approved as a cosmetic treatment only for onychomycosis. It cannot be recommended as a therapeutic intervention to eradicate fungal infection at this time as more rigorous randomized, controlled trials are required to determine if laser therapy is efficacious on par with oral and topical interventions.
The infectious agents that cause onychomycosis invade the nail bed, plate, and matrix. 2 Dermatophytes (Trichophyton spp.) are keratinolytic, so they digest the nail plate, leading to infiltration of multiple layers of the nail plate. 3,4 This niche can also be colonized by yeasts (Candida spp.) or nondermatophyte molds (eg, Fusarium spp., Aspergillus spp.). 5,–7 For laser therapy to be effective, the laser beam needs to have a wavelength that can penetrate through these layers and is strongly absorbed by the fungi. Photoselective processes then kill the fungi via photochemical, photothermal, and photomechanical effects (personal communication from Dr. Don Heller, 2012).
There has been a rapid expansion in the number and variety of laser devices that have been approved for the cosmetic improvement of onychomycosis. It is important to note that lasers have yet to undergo rigorous clinical trials as medical devices can obtain regulatory approval based on “substantial equivalence” to the technical specifications of previous devices. 8 Thus far, laser device systems have not yet been approved as a therapeutic cure for onychomycosis.
Methods
We searched the PubMed database, the Food and Drug Administration (FDA) 510(k) database, ClinicalTrials.gov, and Google Scholar for in vitro studies, peer-reviewed clinical trials, manufacturers' white papers, and registered clinical trials of laser systems indicated for the treatment of onychomycosis. Clinical studies were evaluated for methodological quality using a modified version of the scale we published previously (Table 1). 9 The methodological quality was assessed for peer-reviewed articles and white papers that included a full description of the clinical study conducted. 10,,,,,,,,–19 We excluded the information from the Light Age Q-Clear 510(k) clearance 20 and pending clinical trials 21,,–24 based on insufficient information for assessment.
Criteria Used to Evaluate Studies
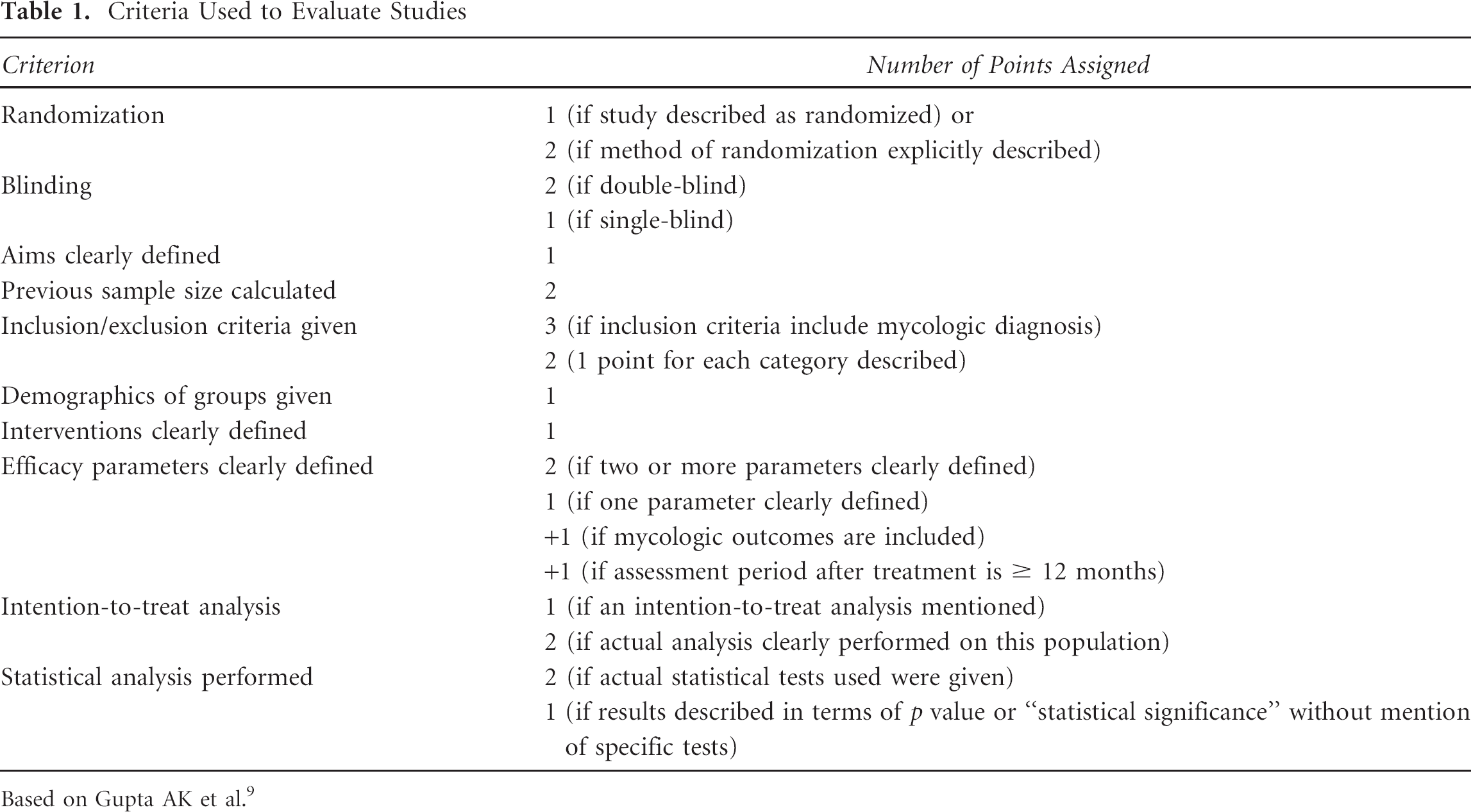
Based on Gupta AK et al. 9
Results
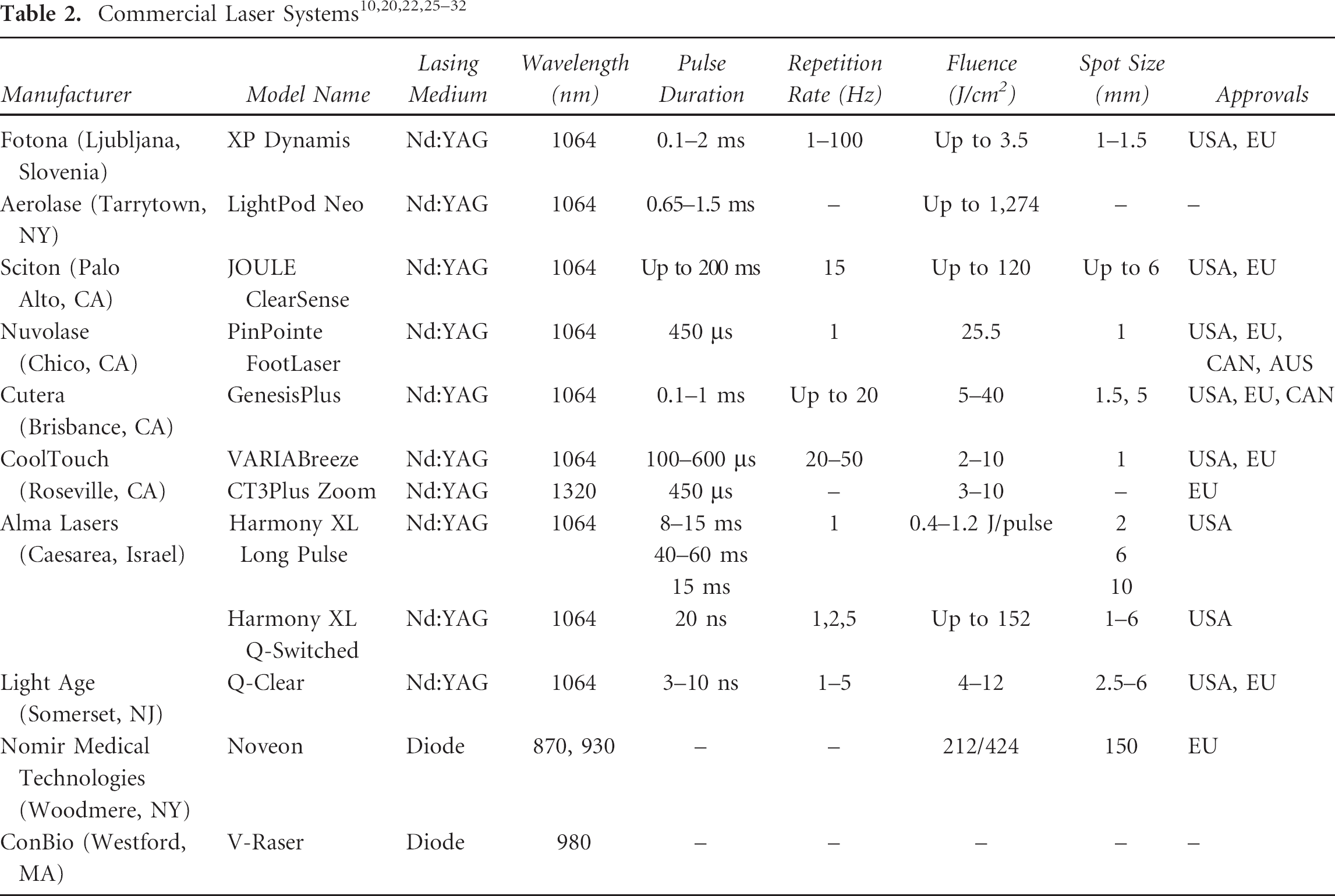
There are a variety of options in the commercial market for laser systems that can be used for onychomycosis. The most popular category of lasers is solid-state lasers, primarily lasers with neodymium:yttrium-aluminum-garnet (Nd:YAG) laser crystals. These lasers can have a variety of pulse durations that affect the power of the laser treatment from lowest to highest maximum pulse energy; these are long-pulse lasers (ms), short-pulse lasers (µs), and Q-switched lasers (ns). The other primary class of lasers is diode lasers, which are continuous lasers. These tend to have a wider variety of laser treatment wavelengths. The technical parameters of commercially available laser systems are summarized in Table 2. 10,20,22,25,,,,,,–32
In Vitro Studies
Three in vitro proof-of-concept studies have been conducted on dermatophyte fungi. 33,–35 The first study was conducted using the Noveon diode laser. 33 Liquid cultures of Trichophyton rubrum and Candida albicans were treated with 870 and 930 nm wavelength light at fluence of 4,074 and 4,500 J/cm2, which resulted in complete photoinactivation 91 hours after treatment. Vural and colleagues published an in vitro study on two intense pulse light devices, a 585 nm pulse dye laser, 532 nm and 1,064 nm Q-switched Nd:YAG lasers, an erbium:yttrium-aluminum-garnet (Er:YAG) 2,940 nm laser, and a 532 nm potassium titanyl phosphate (KTP) laser. 34 Only the Q-switched Nd:YAG lasers had any effect on growth inhibition of T. rubrum. Treatment with the 1,064 nm laser at 4 and 8 J/cm2 and the 532 nm laser at 8 J/cm2 resulted in the greatest inhibition of T. rubrum growth. An additional study was conducted by Manevitch and colleagues using a femtosecond titanium:sapphire laser on T. rubrum growth in nail clippings. 35 Laser energy above 1.7 × 1031 photons m–2 s–1 resulted in elimination of the fungus. An energy of 4.8 × 1031 photons m–2 s–1 resulted in elimination of the fungus without damage to the nail plate; however, increasing energies resulted in severe collateral damage to the nail plate.
Clinical Studies
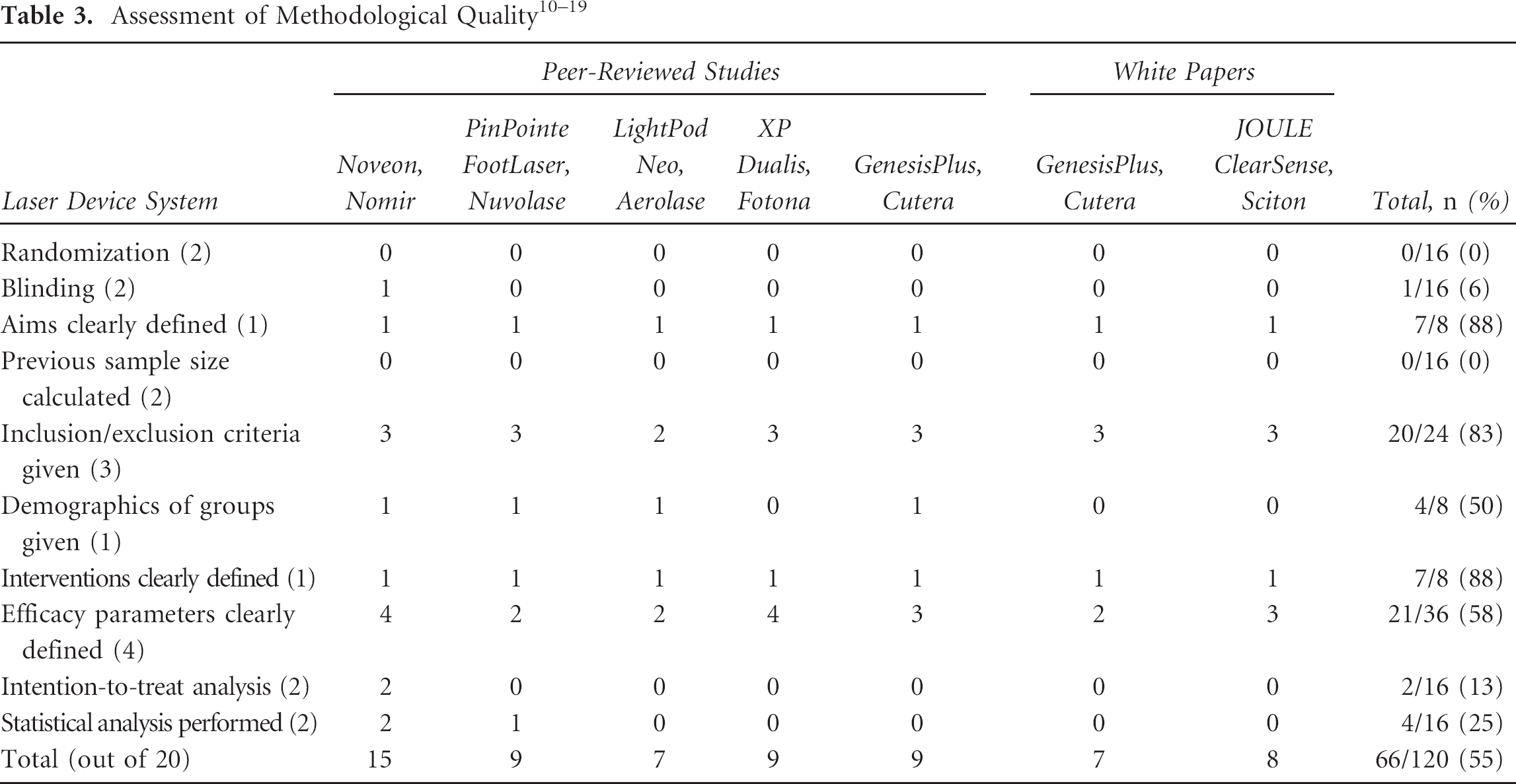
The results of our assessment of methodological quality are shown in Table 3. Overall, clinical studies of lasers have a mean score of 9.1 ± 1.1 out of 20 possible points (see Table 3). 10,,,,,,,,–19 The maximum score was 15, 10,11 and the minimum score was 7. 12,17 Assessed by publication type, peer-reviewed studies have a mean score of 9.8 ± 1.5, 10,,,,,–16 whereas white papers have a mean score of 7.5 ± 0.7. 17,–19
Peer-Reviewed Studies
Noveon, Nomir Medical Technologies
The first clinical study of a laser for onychomycosis was conducted using the Noveon near-infrared diode laser. 10 This dual wavelength system was designed based on the results of the in vitro study by Bornstein and colleagues. 33 Participants with distal and lateral subungual onychomycosis (DLSO) of the great toenail that did not involve the lunula or the hyponchium were enrolled in the study, and diagnosis was confirmed with culture and periodic acid–Schiff (PAS) stain. Patients were treated on days 1, 14, 42, and 120 with a 4 minute dual wavelength treatment followed by 2 minutes at 930 nm with fluences of 424 and 212 J/cm2, respectively. Treatment was paused if the nail exceeded 39°C. The primary outcome measure was negative PAS staining at day 180, which was found in 42% of the participants. The secondary outcome measure was negative mycologie culture, which was found in 39% of participants at day 180. A secondary study with observations at 270 days showed that 35% of participants had improved clear linear nail growth over 3 mm, 38% of patients had a mycologie cure, and 40% had a complete cure. 11 The Noveon laser studies scored 15 of 20 on the methodological assessment scale and were the most complete set of studies assessed; however, the Noveon laser has not been approved by the FDA for the treatment or cosmesis of onychomycosis.
PinPointe FootLaser, Nuvolase
Harris and colleagues conducted an initial study of the PinPointe FootLaser, a 1,064 nm Nd:YAG short-pulse laser system, in a randomized, placebo-controlled, crossover study. 12 Seventeen participants with bilateral onychomycosis of the great toenail were enrolled in the study, and 14 patients were included in the treatment groups. Eleven of 14 participants showed improvement in clear linear nail growth. The only adverse event reported was painful sensation during treatment. The PinPointe study received a methodological score of 9 of 20.
LightPod Neo, Aerolase
An initial study of an Nd:YAG 1,064 nm short-pulse laser (0.65 ms) was conducted by Hochman using a LightPod Neo laser. 13 Eight participants with fingernail or toenail onychomycosis confirmed by culture or PAS stain were enrolled in the study. Participants were treated with a 2 mm spot with a 223 J/cm2 fluence. Patients were treated two or three times at 3-week intervals. Seven of eight participants resulted in a negative fungal culture at 4 to 6 months after the initiation of treatment. The LightPod Neo study received a quality assessment score of 7 and suffered primarily from a small sample size, limited efficacy outcomes, and the use of descriptive instead of qualitative outcomes.
XP Dualis, Fotona
Two studies were conducted using a 1,064 nm Nd:YAG long-pulse laser (35 ms). 14,15 Overall, these studies included 234 participants with fingernail and toenail onychomycosis confirmed by potassium hydroxide (KOH) microscopy. Participants were treated with a 4 mm spot size with a fluence of 35 to 40 J/cm2 and a repetition rate of 1 Hz. The treatment consisted of four treatments at 1-week intervals. In the initial study of 72 participants, follow-up confirmed that 100% of participants had achieved a mycologie cure after 1 year. The second study of 162 participants confirmed that 100% mycologie cure was achieved after 12 months. The adverse events reported in both studies included pain and sensation during treatment and a slight yellowing of the nails. This study received a quality score of 9, suffering primarily from the lack of a control group to compare to the results of the single assignment study. It is important to note that this system differs from the current laser marketed by Fotona to treat onychomycosis that has FDA approval. 25
GenesisPlus, Cutera
In 2012, Kimura and colleagues published a study on 13 participants with KOH microscopy–confirmed onychomycosis. 16 Participants were treated with a spot size of 5 mm, an energy fluence of 14 J/cm2, a pulse duration of 0.3 ms, and a repetition rate of 5 Hz. Nineteen of 37 affected toenails showed a complete cure with negative mycologie microscopy. An additional 19% of nails showed significant clearance. The only adverse event reported was a mild warming sensation during treatment. This study received a quality assessment of 9 of 20. In addition, the assessment of nails rather than participants diminishes the validity of the efficacy outcomes.
White Papers and Gray Literature
GenesisPlus, Cutera
Weiss conducted a trial of the GenesisPlus, which is a 1,064 nm Nd:YAG short-pulse laser system. 17 Seven participants with onychomycosis received two treatments at a 6-week interval. This laser has a 5 mm spot size, a 16 J/cm2 energy fluence, a repetition rate of 2 Hz, and a pulse duration of 0.3 ms. At the 3-month follow–up, 70% of the nails treated showed improvement in clear nail growth. This study received a quality assessment score of 7 of 20.
JOULE ClearSense, Sciton
Waibel conducted a preliminary trial of the 1,064 nm Nd:YAG short-pulse JOULE ClearSense laser system. 18 Twenty-one participants with onychomycosis confirmed by KOH microscopy and culture were enrolled in this study. Participants received four treatments at 1-week intervals, with follow-up at 6 months. The treatment was conducted with a 13 J/cm2 energy fluence and a repetition rate of 6 Hz. At follow-up, 95% of participants had achieved a mycologie cure. Mild sensation during treatment was the only adverse event reported.
Bessinger released two case reports of treatment with the JOULE ClearSense laser. 19 A 50–year-old woman and a 53-year-old man with DLSO of the right hallux toenail were treated with a 5 J/cm2 energy fluence, 0.3 ms pulse duration, and 3 Hz repetition rate. Each participant received two treatments at a 1-month interval. No adverse events were observed. Two months after the treatments, both participants showed an increase in clear nail.
The JOULE ClearSense is one of the only laser systems to have clinical results reported by multiple clinicians. The methodological quality score is 8 of 20, despite multiple reports, as the Bessinger article is based on case reports, not clinical trials data.
Q-Clear, Light Age
Light Age conducted a preliminary trial of the 1,064 nm Nd:YAG Q-switched Q-Clear system on 100 subjects with dystrophic toenails. 20 Treatment resulted in improvement in clear nail in 95% of patients, with an average clearance of 56 ± 7% of toenail area. Some participants reported a low-level sensation during treatment. These data were presented in the FDA 510(k) clearance of the Q-Clear model and were not derived from a publication of the clinical study.
Pending Clinical Trials
CT3Plus Zoom, CoolTouch
The University of California, Irvine, has registered a clinical trial of the 1,320 nm Nd:YAG CoolTouch CT3Plus Zoom laser with the CoolBreeze Zoom handpiece (NCT01498393). 21 This trial intends to enrol 15 participants with bilateral onychomycosis of the great toenails. The primary outcome measure is “improving fungal nail infection” at 6 months.
V-Raser, ConBio
ConBio has registered a clinical trial of the 980 nm diode V-Raser system (NCT01452490). 22 The trial aims to enrol 50 participants with confirmed subungual onychomycosis in a great toe that does not extend to the eponychium. Participants will receive four treatment sessions at 6-week intervals. The primary outcome measure is the amount of clear nail growth from baseline in millimeters or as a measurement of the total area of involvement at the 12-month follow-up.
Er:YAG Laser and Amorolfine Nail Lacquer
Brasilia University Hospital registered a clinical trial of joint treatment with an Er:YAG laser and amorolfine nail laquer (NCT01528813). 23 This trial aims to enrol 30 participants with onychomycosis of at least two fingernails or toenails confirmed by direct mycologie examination or culture. This internally controlled study will assign one nail to each treatment group. Group A will receive a single laser treatment followed by amorolfine lacquer for 6 months, whereas group B will only receive amorolfine nail lacquer for 6 months. The primary outcome measure is the extent of nail plate damage at 6 months. The secondary outcomes are mycologie cure and clinical cure at 6 months.
FSS Laser, Erchonia
The Erchonia Corporation has registered a clinical trial of a 405 and 635 nm dual wavelength laser system (NCT01534689). 24 This study aims to enrol 105 participants with onychomycosis of at least one great toenail. Participants will receive 10 minutes of treatment with the dual wavelength device. The primary outcome measure is mean percentage of increased clear nail at 6 months after the final laser treatment. The secondary outcome measure is change in millimeters of clear nail bed at 27 weeks.
Discussion
Laser device therapy is a nascent field of therapeutics for onychomycosis. At present, only three basic science research studies examined the efficacy of laser in culture and on ex vivo samples. 33,–35 This limits the data available for the development of diverse laser models for the targeting of dermatophyte fungi. Nomir is the only laser manufacturer to build directly from a basic science research study to develop a laser system, 10,11,33 although the Nd:YAG laser models are informed by the work of Vural and colleagues. 34 The clinical studies that have been initiated have been small, exploratory studies. The most notable insufficiencies have been the lack of control or active comparator studies that have undergone randomization and blinding. This makes intention-to-treat and statistical analysis of the efficacy outcomes difficult and explains the low methodological quality scores seen in all studies.
The goals of the regulatory approvals process for medical devices may explain why randomized, controlled trials have not been the primary study design for lasers. The FDA approves these laser systems on the basis of “substantial equivalence” to predicate models, 8 and their indications for onychomycosis have primarily been validated for “temporary increase of clear nail in onychomycosis.” 20,25,27,,–30,32 These approvals are only for cosmetic outcomes, which may explain why these trials have focused primarily on increases in clear nail plate area, not on mycologic cure. If laser systems do not need approval for therapeutic eradication of fungal infections to reach the market, there is no need to validate the clinical efficacy of the laser models in curing onychomycosis. Laser therapy may offer the advantages of being a minimally invasive, clinically conducted procedure with a minimal requirement for patient compliance, but it cannot be considered an effective cure for onychomycosis until more rigorous clinical trials are conducted.
Conclusion
Laser therapy for onychomycosis may become an alternative to traditional pharmacotherapy; however, there is a clear need for studies with increased enrolment, mycologie examination before and after treatment, extended follow-up periods, and standardized outcome measures to determine if laser therapy is effective for the treatment of onychomycosis or comparable to traditional pharmacotherapeutics.
Footnotes
Acknowledgment
Dr. Gupta has acted as a consultant for Nuvolase Inc. and Cutera Inc.
Financial disclosure of reviewers: None reported.