
Abstract
Background:
Sarcoidosis is a multisystemic disorder of unknown etiology that can affect multiple organs, including the lungs, skin, and eyes. Vulvar sarcoidosis has anecdotally been reported.
Objective:
The aim of this article is to describe a case of vulvar sarcoidosis and review the few cases that have been reported.
Methods:
We report the case of a 39-year-old woman who presented to the dermatologist with a 2-year history of vulvar pruritus.
Results:
Examination revealed infiltrated plaques on the vulva and perianal region. The biopsy demonstrated well-defined, nonnecrotizing granulomas in the dermis. Further investigation revealed hilar adenopathy consistent with sarcoidosis. The patient responded well to topical corticosteroids.
Conclusion:
In the presence of granulomatous lesions of the genital region, infectious causes, foreign body reaction, Crohn disease, and sarcoidosis should be part of the differential diagnosis.
Classically, skin lesions are classified as specific when nonnecrotizing granulomas are present in tissue samples. The most typical specific lesions are annular or polycyclic brownish-purple infiltrated plaques, papules, nodules, and violaceous infiltrations of the face, extensor surface of the extremities, scalp, back, and buttocks.1,2 Nonspecific skin lesions do not have formation of granulomas and are reactive.1,3
Erythema nodosum is the most common nonspecific lesion, being present in 25% of cases. 3 Even in recent reviews, 3 genital sarcoidosis has rarely been reported.
Case Report
A 39-year-old Moroccan woman was referred to our clinic because of a 2-year history of vulvar pruritus.
She was initially seen by her gynecologist, who performed a vulvar biopsy that demonstrated well-defined, nonnecrotizing granulomas in the dermis without birefringent material. Periodic acid-Schiff, Gram, Grocott, and Ziehl-Neelsen stains were all negative. These observations led to the initial pathologic diagnosis of a nonspecific granulomatous dermatitis. An infectious cause could not be ruled out, and tissue cultures were recommended. Subsequent bacterial and superficial fungal cultures were negative. The patient also had an abdominal sonogram demonstrating an intrauterine contraceptive device, normal chest x-rays, and a negative tuberculin test.
The patient was then referred to our clinic. Her past medical and family history was noncontributory. She had three pregnancies and one miscarriage. Physical examination revealed annular erythematous plaques of the labia majora and perianal regions (Figure 1 and Figure 2).

Erythematous infiltrated plaques on the vulva.

Infiltrated and erythematous plaques in the perianal region.
Initial pathologic slides were reviewed by our derma-topathologist, and additional tests were performed to rule out Crohn disease and an infectious granulomatous dermatitis. While waiting for supplementary tests, the patient was treated with mometasone furoate cream daily for 2 weeks, with little improvement.
Chest radiography was repeated and was normal. The abdominal sonogram and a gastroduodenoscopy were all normal, with duodenal, ileal, and colonic biopsies showing normal tissue.
After completing the investigation, the patient was seen on follow-up 3 months later. She was still symptomatic but mentioned lesions on her knees that had once been present in her teenage years but disappeared and recently recurred (Figure 3). We performed a vulvar biopsy and a lesional biopsy of her knee that showed, in both cases, nonnecrotizing, well-defined granulomas (Figure 4 and Figure 5).

Small confluent erythematous papules on the knees.
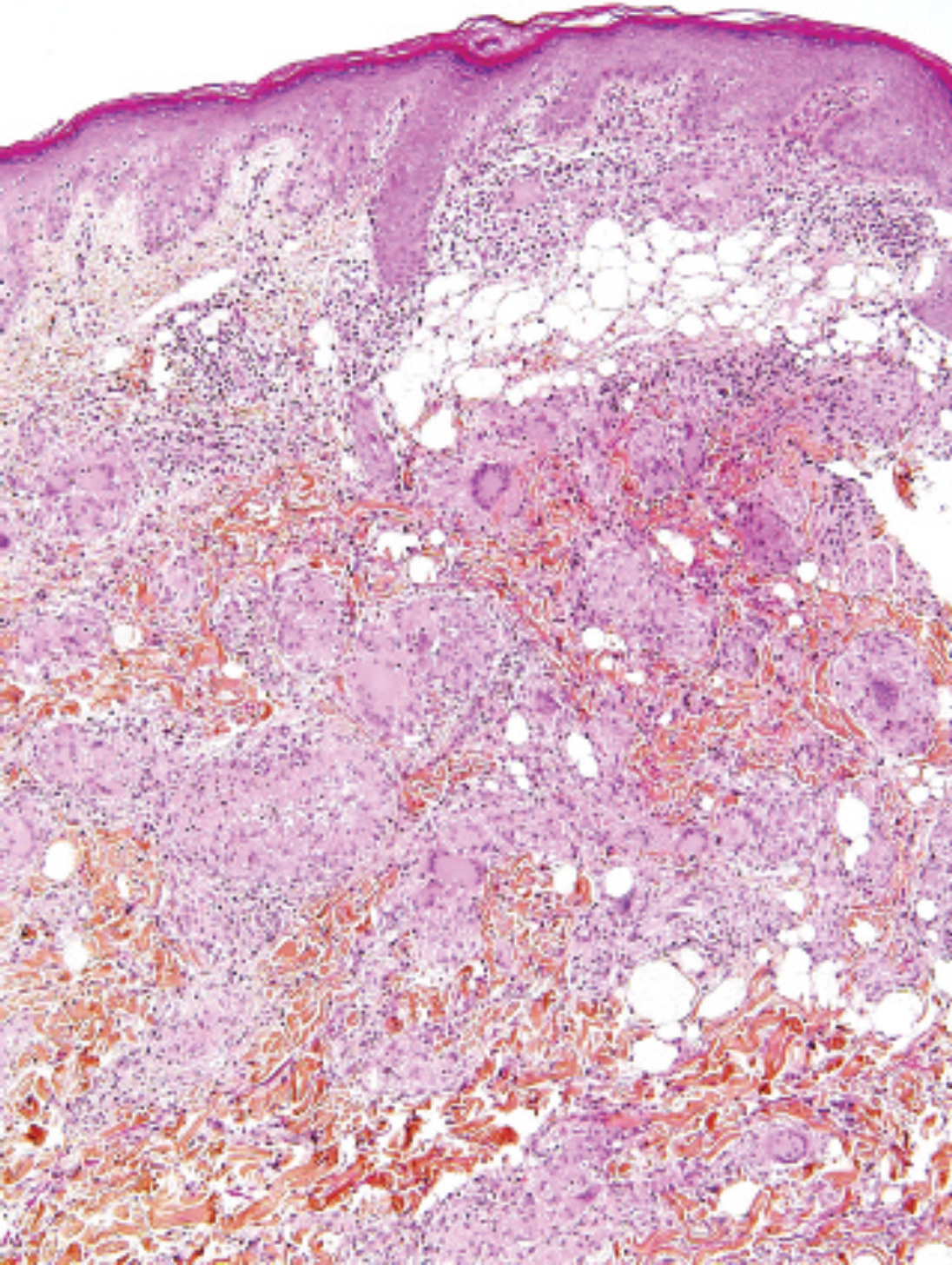
Nonnecrotizing granulomas in the dermis (hematoxylin-phloxin-saffron stain; ×10 original magnification).
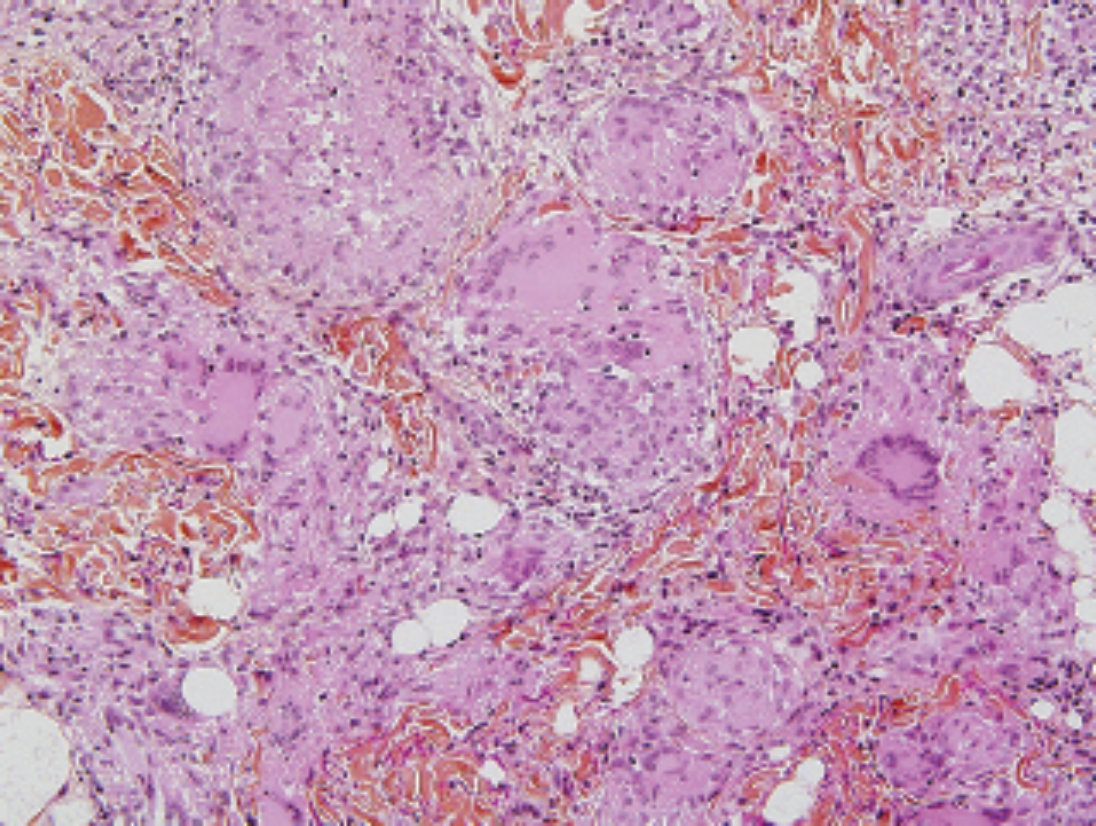
Higher magnification of naked sarcoidosic granulomas in the dermis (hematoxylin-phloxin-saffron stain; ×20 original magnification).
The patient's serum angiotensin-converting enzyme level was 60 U/L (normal up to 52 U/L), but the blood count, calcium, renal, and liver functions were normal. An electrocardiogram was also normal. Pulmonary function tests were normal, but a second chest radiograph revealed hilar adenopathies. This was confirmed by a chest computed tomographic scan that showed multiple hilar and axillary nodes.
The patient was seen by the pneumology team, and bronchoscopy was performed along with nodal biopsies. Epithelioid granulomas consistent with sarcoidosis confirmed the diagnosis of sarcoidosis, but as the patient was asymptomatic, no treatment was suggested. The patient was also referred to Ophthalmology, and no anomalies were detected.
The vulvar lesions resolved with amcinonide cream 0.1%, a high-strength topical steroid. The patient is still asymptomatic and is seen on a regular basis by Dermatology and Pneumology.
Discussion
Vulvar sarcoidosis is a very unusual presentation, and to date, only five cases have been reported in the literature4,,,–8 (Table 1).
Cases of Vulvar Sarcoidosis Previously Reported
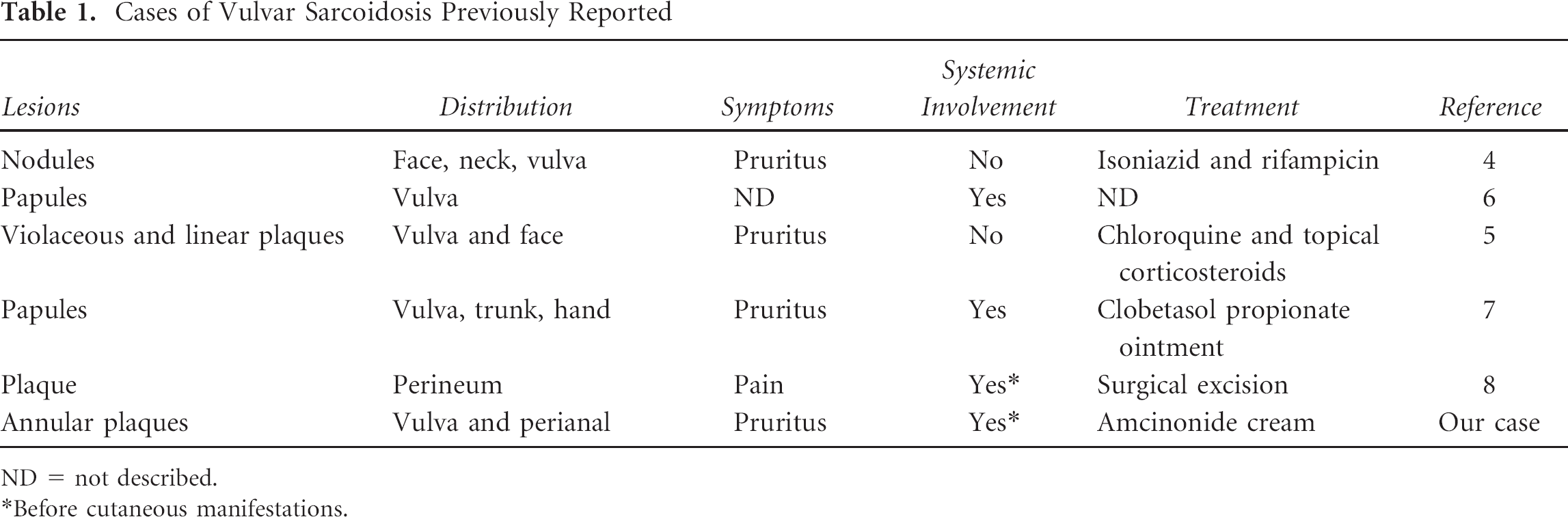
ND = not described.
Before cutaneous manifestations.
In two cases, the patients presented with lesions on the vulva, neck, and face.4,5 One of these cases reported pruritic violaceous lesions and linear plaques on the vulva. 5 The patient was treated with chloroquine and topical corticosteroids, with little improvement.
In two other reports, vulvar lesions led to the diagnosis of systemic sarcoidosis,6,7 as in our patient. One of these patients presented with pruritic papules on the vulva, trunk, and hand and was successfully treated with a potent steroid ointment. 7
In another case, a woman with a recent diagnosis of pulmonary sarcoidosis presented a painful lesion of the vulva that was excised by surgery. The histologic examination of the specimen showed well-defined granulomas of sarcoid type in the dermis composed of epithelioid histiocytes, lymphocytes, and a few multinucleated Langerhans giant cells. The final diagnosis was sarcoidosis of the vulva. 8
Extrapulmonary sites of involvement in sarcoidosis include the central nervous system, lymph nodes, skin, liver, eyes, anogenital regions, and, very rarely, the female genital tract.3,9,10
Treatment of cutaneous sarcoidosis can be difficult, and there are no guidelines for initiating therapy. 2 A recent review proposed an algorithm of treatment, 3 but as sarcoidosis can spontaneously remit, a stepwise approach should be considered when lesions are progressive, disfiguring, or function impairing.2,3,5
The accepted standard therapy for cutaneous sarcoidosis includes corticosteroids due to their ability to suppress inflammation and granuloma formation. It is reasonable to start with topical potent corticosteroids and to escalate to intralesional, oral, or systemic corticosteroids according to the response or degree of involvement.
Antimalarial agents, methotrexate, and a combination of these agents are also standard therapies for sarcoidosis. Other therapies that have been successfully used in case reports and series include tetracyclines, isotretinoin, leflunomide, thalidomide, pentoxifylline, and infliximab, as well as surgical excision and laser therapy with pulsed dye, Q-switched, or CO2 laser.
Our patient responded well to topical corticosteroids and is still asymptomatic.
Conclusion
Vulvar sarcoidosis is an unusual presentation that can be the only manifestation of sarcoidosis or can precede, be concomitant, or appear after a diagnosis of systemic sarcoidosis. When granulomatous lesions are present on the vulva, the differential diagnosis should include infectious diseases such as tuberculosis, syphilis, lymphogranuloma venereum, Crohn disease, and a foreign body reaction. All of these diseases were ruled out in our patient.
Footnotes
Acknowledgment
Financial disclosure of authors and reviewers: None reported.