
Abstract
Background:
Poor hygiene and nutrition and resultant compromised immune status in some psychiatric patients can increase susceptibility to bacterial skin infections.
Objective:
We examined the frequency of ICD9-CM psychiatric disorders (codes 290–319) in bacterial skin infections (ICD9-CM codes 680–686) (N = 18,734) versus malignant and benign cutaneous neoplasms (ICD9-CM codes 172, 173, 232, 216) (N = 8,376), conditions that would be expected to cause psychological distress for the patient.
Methods:
Logistic regression analysis was conducted controlling for age, sex, race, diabetes, obesity, and the use of antineoplastic and immunosuppressant medications.
Results:
Skin infections were more commonly (odds ratio = 3.03, 95% CI 1.58–5.82) associated with a psychiatric disorder; the most frequent diagnoses were substance dependence and abuse (19.5%), depressive disorder (19.0%), attention-deficit disorder (14.4%), and anxiety disorders (11.6%).
Conclusion:
In contrast to cutaneous neoplasms, bacterial skin infections were three times as likely to be associated with a psychiatric disorder. Psychiatric comorbidity should be ruled out as a factor in patients with intractable skin infections.
The relationship between psychiatric morbidity and bacterial infections of the skin is likely bidirectional as the psychosocial impact of having to live with a cutaneous infection can in turn contribute to psychiatric morbidity. Infection and inflammation can also play a role in the pathogenesis of psychiatric disorders such as depressive illness, which has been associated with raised markers of ongoing inflammation, including raised levels of proinflammatory cytokines. 2 A subtype of obsessive compulsive symptom has been associated with group A β-hemolytic streptococcal infection in genetically susceptible children, 13 believed to be secondary to the cross-reaction of the antibodies to the bacteria with brain tissue. Finally, many antibiotics that are used to treat cutaneous infections can have psychiatric side effects. 14,15 Diabetes mellitus and obesity can confound the association of bacterial skin infections and psychiatric morbidity as they are both associated with an increased frequency of infectious skin diseases and are also more frequently encountered in psychiatric patients, often as a result of side effects of psychiatric medications. 16 To our knowledge, no large-scale studies have examined the frequency and nature of psychiatric morbidity in patients with bacterial infections of the skin and subcutaneous tissue.
In this study, we examined the frequency of psychiatric disorders in an epidemiologically representative sample of patient visits in the United States with infections of the skin and subcutaneous tissue. For the purposes of comparison, we examined psychiatric morbidity in patients with benign and malignant neoplasms of the skin, conditions that can be at least as life-threatening as complicated skin infections but, like cutaneous infections, are not typically known to be directly exacerbated by psychiatric factors (such as in the case of conditions such as psoriasis and atopic dermatitis). We statistically controlled for potential confounding factors such as age, gender, antineoplastic and immunosuppressive medication use, and the presence of diabetes mellitus and obesity. To our knowledge, this is the first reported study that has systematically examined psychiatric morbidity in patients with bacterial skin infections.
Methods
Sample and Measurement
Using a retrospective cross-sectional design, we examined data collected from 1995 to 2009 by the National Ambulatory Medical Care Survey (NAMCS) 17 and National Hospital Ambulatory Care Survey (NHAMCS). 17 The NAMCS and NHAMCS are national surveys conducted by the National Center for Health Statistics (NCHS) at the Centers for Disease Control and Prevention and use a multistage probability design to collect nationally representative samples of health care visits to physicians' offices (NAMCS) and hospital outpatient departments and emergency departments (NHAMCS) in the United States. Full details of the multistage data collection method are available on the NAMCS/NHAMCS website. 17 The NAMCS and NHAMCS Public Use Data files from 1995 to 2009 were merged into one database for our analyses. The combining of the NAMCS and NHAMCS databases from 1995 to 2009 improved the reliability of the estimates. 18 The NAMCS and NHAMCS code up to three diagnoses per patient visit using the International Classification of Diseases, 9th Edition, Clinical Modification (ICD9-CM) 19 codes. On the survey record form, 19 the attending physician is instructed to “as specifically as possible, list diagnoses related to this visit, including chronic conditions,” and there is provision for listing a primary diagnosis and two additional diagnoses. The visits associated with an ICD9-CM diagnosis of infections of the skin and subcutaneous tissue and the controls consisting of patient visits with both malignant and benign cutaneous neoplasms were extracted from the merged database for our analyses. Using the masked weighting variables provided by the NCHS, the two databases analyzed in this report represented 18,734 (weighted estimate ± SE: 165,734,499 ± 7,421,728) patient visits with infections of the skin and subcutaneous tissue and 8,376 (weighted estimate ± SE: 161,667,103 ± 8,825,772) patient visits with malignant and benign neoplasms of the skin to physicians' offices and hospital outpatient and emergency departments from 1995 to 2009. The demographic characteristics of the study sample are summarized in Table 1.
Total Visit Count, Age, Sex, and Race of Study Sample
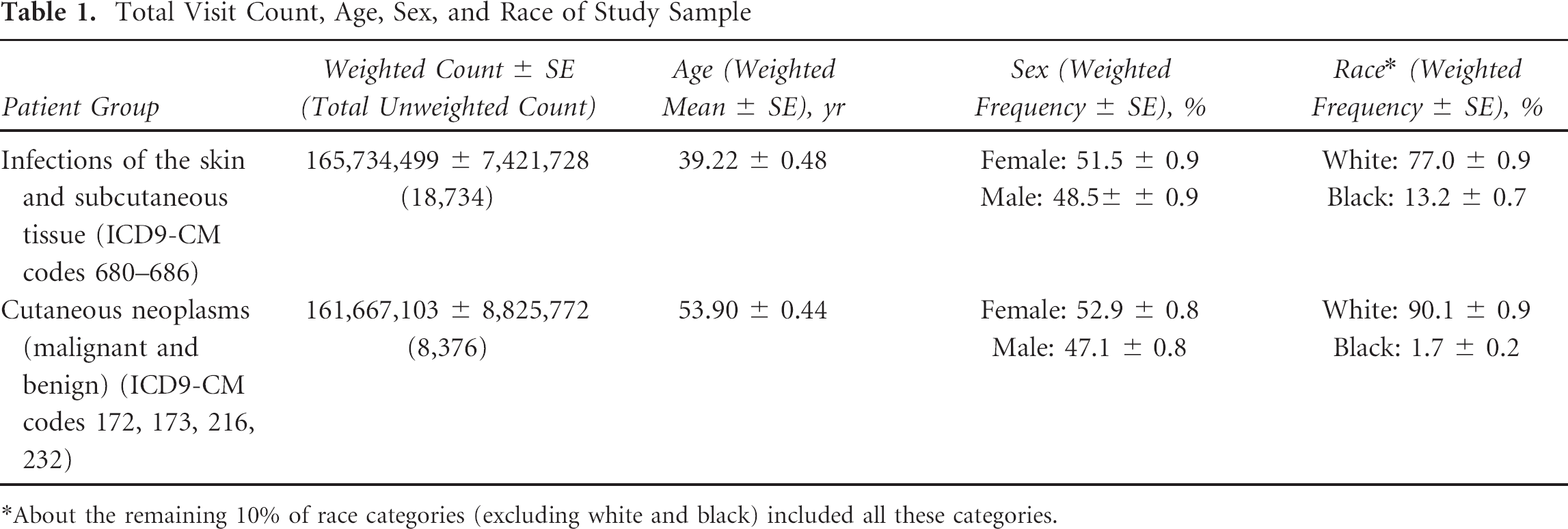
About the remaining 10% of race categories (excluding white and black) included all these categories.
Variables
The following variables were derived from the merged NAMCS/NHAMCS database representing patient visits for all diagnoses from 1995 to 2009:
The infection of the skin and subcutaneous tissue variable included any patient visit where at least one of the three possible diagnoses was coded using ICD9-CM codes 680 to 686, which denote the following major groups of infections: carbuncle and furuncle (all codes 680), cellulitis and abscess of finger and toe (all codes 681), other cellulitis and abscess (all codes 682), acute lymphadenitis (all codes 683), impetigo (all codes 684), pilonidal cyst (all codes 685), and other local infections of skin and subcutaneous tissue (all codes 686). The malignant and benign cutaneous neoplasms variable included any patient visit where at least one of the three possible diagnoses was coded using ICD9-CM codes for malignant melanoma of the skin (all codes 172), other malignant neoplasm of skin (all codes 173), carcinoma in situ of skin (all codes 232), and benign neoplasms of the skin (all codes 216). The psychiatric disorders variable included any patient visit where at least one of the three possible diagnoses was coded using ICD9-CM codes 290 to 319 for mental disorders. The diabetes mellitus variable included any patient visit where at least one of the three possible diagnoses was coded using ICD9-CM codes 250, which code for both non–insulin-dependent and insulin-dependent diabetes mellitus and their complications. The obesity variable included any patient visit where at least one of the three possible diagnoses was coded using the ICD9-CM codes 278, 278.0, 278.00, and 278.01 related to obesity and morbid obesity. Age was categorized as ≤ 50 years versus > 50 years. As skin type can affect the risk of skin cancers, a dichotomous white and nonwhite (which included black, Asian, Native Hawaiian, Pacific Islander, American Indian, Alaska Native, and more than one race reported) race variable was created to statistically control for the confounding effect of skin type as determined by race. We further controlled for the possible confounding effect of medications with immunosuppressive effects used to treat cutaneous malignancies as they can significantly influence the immune status and infection susceptibility of the patient. We therefore created variables for patient visits associated with the use of medications categorized as antineoplastic and immunosuppressive according to the Ambulatory Care Drug Database System (ACDDS)
20
that is used by the NAMCS and NHAMCS to classify medications.
19
The specific medications listed under each category are described in detail on the ACDDS website.
20
The antineoplastic medications variable included all medications listed as antineoplastics (class 020) under the ACDDS
20
Drug Therapeutic Category, Level 1. The immunosuppressive agents variable included all medications listed as immunosuppressive agents (class 104) under the ACDDS
20
Drug Therapeutic Category, Level 2; the ACDDS
20
Drug Therapeutic Category, Level 1, for immunologic agents (class 245) had to be accessed first before the subcategory of ACDDS Drug Therapeutic Category, Level 2, immunosuppressive agents, was accessed.
Statistical Analysis
All analyses were conducted using the Complex Samples module of SPSS version 15 21 to account for the multistage probability sampling design used by the NAMCS and NHAMCS. A dichotomous variable was created using the infection of the skin and subcutaneous tissue and malignant and benign cutaneous neoplasms variables. The relationships of these variables to psychiatric disorders were contrasted using logistic regression analysis after controlling for confounders such as age (≤ 50 years versus > 50 years), sex, race (white versus nonwhite), diabetes mellitus, obesity, antineoplastic medications, and immunosuppressive agents (Table 2).
Results of Logistic Regression Analysis Using Infection of the Skin and Subcutaneous Tissue versus Malignant and Benign Cutaneous Neoplasms (Comparison Group) as the Dependent Variable
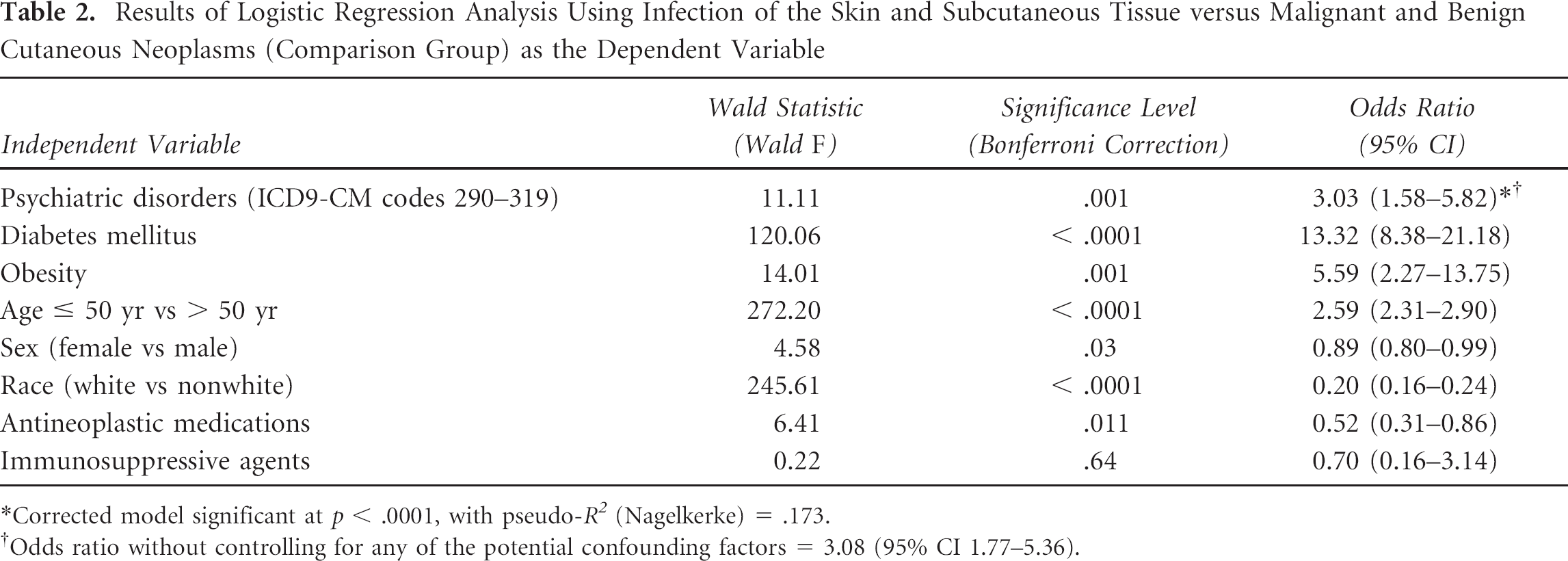
Corrected model significant at p < .0001, with pseudo-R 2 (Nagelkerke) = .173.
Odds ratio without controlling for any of the potential confounding factors = 3.08 (95% CI 1.77–5.36).
Results
There were an estimated (weighted count ± SE) 3,340,689 ± 423,230 (unweighted count = 344) patient visits with both infection of the skin and subcutaneous tissue and psychiatric disorders, and there were an estimated (weighted count ± SE) 1,079,574 ± 283,913 (unweighted count = 52) patient visits with both malignant and benign cutaneous neoplasms and psychiatric disorders. Cutaneous infections of the skin and subcutaneous tissue were over three times more likely (odds ratio [OR] 3.03, 95% CI 1.58–5.82) to be associated with a psychiatric disorder than malignant and benign cutaneous neoplasms after the potential confounding effects of diabetes, obesity, age, sex, race, and use of antineoplastic and immunosuppressive agents were controlled for statistically (see Table 2). All conditions were physician diagnosed at the time of data collection and coded using standard ICD9-CM codes. Table 3 summarizes the most frequent psychiatric diagnoses, with their respective ICD9-CM diagnostic codes, in patient visits associated with bacterial infection of the skin and subcutaneous tissue.
Most Frequent Psychiatric Diagnoses (as One of Three Possible Diagnoses) in Patient Visits with Infection of the Skin and Subcutaneous Tissue
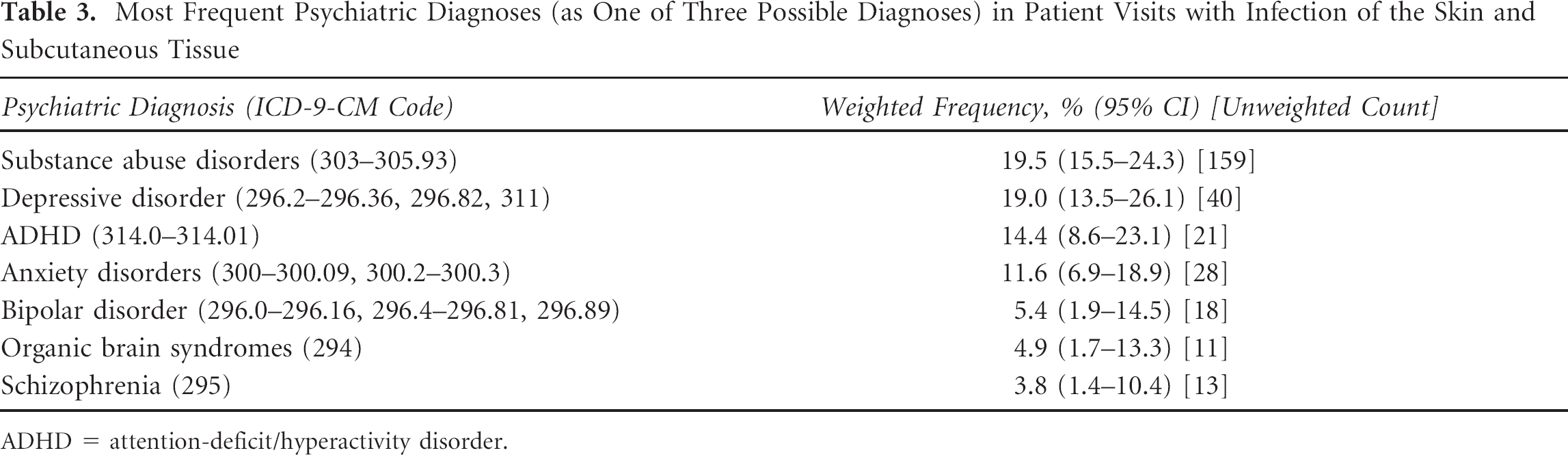
ADHD = attention-deficit/hyperactivity disorder.
Discussion
Our results from an epidemiologically representative sample indicate that psychiatric disorders (ICD9-CM codes 290–319) were diagnosed over three times as frequently in patients with bacterial infections of the skin and subcutaneous tissue (ICD9-CM codes 680–686) in contrast to malignant and benign cutaneous neoplasms (ICD9-CM codes 172, 173, 216, 232) (see Table 2), after the potential confounding effects of diabetes, obesity, age, sex, race, and use of antineoplastic and immunosuppressive agents were controlled for statistically (see Table 2). The estimates of the variable in our analysis met the NCHS standards 18 for reliability; that is, they are based on at least 30 sample records and have relative standard errors (standard error divided by the estimate) of less than 30%. 18 To our knowledge, there are no previously reported studies that have systematically examined the association between bacterial infections of the skin that constitute one of the most common dermatologic disorders and psychiatric morbidity.
The literature on psychiatric morbidity in bacterial skin infections has primarily reported the presence of substance dependence and abuse disorders. 3,,,,,,–10 Our results (see Table 3) are consistent with this literature and indicate a 19.5% (95% CI 15.5–24.3) frequency of substance abuse and dependence in our sample of patients with bacterial skin infections. We also report other psychiatric disorders, such as a 19.0% (95% CI 13.5–26.1) frequency of depression (see Table 3), which has not been previously reported in patients with bacterial skin infections (other than leprosy 12 ). Depressive disease is a common and treatable condition that can theoretically complicate the course of bacterial skin infections by affecting self-care functions such as personal hygiene; by increasing the tendency for intentional self-injury, which can perpetuate an existing infection; and by possibly compromising the immune status of the patient.
The following previously unreported psychiatric disorders (see Table 3) were also frequently present in patients with bacterial skin infections; however, these results should be interpreted as preliminary because the total number of unweighted cases for each diagnosis was less than 30 unweighted cases 18 : attention-deficit/hyperactivity disorder (ADHD), 14.4% (95% CI 8.6–23.1); anxiety disorders, 11.6% (95% CI 6.9–18.9); bipolar disorder, 5.4% (95% CI 1.9–14.5); organic brain syndromes, 4.9% (95% CI 1.7–13.3); and schizophrenia, 3.8% (95% CI 1.4–10.4). These disorders are often associated with poor self-care as a result of impulsivity and overall difficulties with executive functioning. Early stages of organic brain syndromes can theoretically result in neglect of self-care and poor hygiene as a more subtle sign of cognitive dysfunction.
As for demographic factors, there were significantly more males age ≤ 50 years with cutaneous infections and psychiatric morbidity, which is consistent with our finding that some of the most frequent psychiatric diagnoses (see Table 3) in this group included substance abuse disorder and ADHD, which are both more common among younger males. As for race (see Table 2), the significantly fewer whites versus nonwhites in the skin infections versus the skin malignancy group is entirely consistent with the fact that skin malignancies would be expected to be more common among individuals with Fitzpatrick type I and II skin who would have been classified as white.
The highly significant effect of diabetes mellitus (OR = 13.32, 95% CI 8.38–21.18) and obesity (OR = 5.59, 95% CI 2.27–13.75) (see Table 2) in the skin infections group is entirely consistent with the fact that diabetes and obesity are known to be frequently associated with skin infections versus skin cancers. The significantly lower frequency of use of antineoplastic medications among patients with skin infections versus skin neoplasms is entirely clinically expected; there was no significant difference in the frequency of use of immunosuppressive agents between the two groups (see Table 2).
A weakness of our study is the fact that our results are based on retrospective cross-sectional data; therefore, it is not possible to arrive at any conclusions regarding causation—for example, having a bacterial skin infection, which can impact the quality of life of the patient, could have caused psychiatric problems. Second, the basic sampling unit in the NAMCS and NHAMCS is the patient visit; therefore, it is possible that some of the data points represent the same patient seen for more than one visit during the data collection period.
Our preliminary results (see Table 3) also suggest that in addition to substance abuse disorders and depressive disease, bacterial skin infections may be confounded by the presence of ADHD or major psychiatric illness, such as bipolar disorder, schizophrenia, and organic brain syndromes, which can all be associated with difficulties with executive functioning and resultant poor self-care. These previously unreported findings from a large epidemiologically representative sample suggest that the clinician should maintain an index of suspicion for underlying substance abuse, depressive illness, and possibly other mental disorders in patients presenting with infections of the skin and subcutaneous tissue. Recognition and management of psychiatric comorbidity may help the management of bacterial infections of the skin and subcutaneous tissue and possibly decrease the frequency of medical complications associated with these infections.
Footnotes
Acknowledgment
Financial disclosure of authors and reviewers: None reported.