
Abstract
Background:
Eosinophilic fasciitis is a rare sclerosing syndrome with a poorly understood etiology.
Objective:
We report a case of eosinophilic fasciitis in a 40-year-old man undergoing treatment with natalizumab for multiple sclerosis. Natalizumab is a selective adhesion molecule inhibitor that prevents interaction of leukocytes with endothelial cells. Peripheral blood eosinophilia has been described under treatment with natalizumab, but we herein report the first case to our knowledge of eosinophilic fasciitis as a possible complication of this medication.
EOSINOPHILIC FASCIITIS is a rare sclerosing syndrome first reported by Shulman in 1975 1 as the association of diffuse fasciitis with blood eosinophilia. It presents clinically as edema and diffuse subcutaneous induration of the limbs and trunk. On biopsy specimens, a thickened muscular fascia with eosinophilic infiltration is observed. To date, the etiology of this syndrome is poorly understood.
We report a case of eosinophilic fasciitis in a patient undergoing treatment with natalizumab for multiple sclerosis (MS). Natalizumab is a recombinant humanized monoclonal antibody that prevents adhesion of leukocytes to endothelial cells by binding to the α4 subunit of α4β1 and α4β7 integrins present on the surface of lymphocytes, eosinophils, basophils, and monocytes. It was approved by the Food and Drug Administration in 2004 for the treatment of relapsing-remitting MS. Natalizumab has been associated with peripheral blood eosinophilia. 2,–4
Case Report
A 40-year-old man with long-standing treatment-resistant MS presented with bilateral erythematous to brownish indurated plaques of the pretibial areas. This had been progressing for 2 weeks following the completion of intensely physical renovation work that had lasted 2 weeks. He was not known for any other medical conditions. He had started treatment with natalizumab a year before, at a standard dose of 300 mg IV every 4 weeks. No other medication was taken by the patient.
He first presented to the emergency service and was treated with multiple courses of systemic antibiotics for a presumed diagnosis of bilateral infectious cellulitis. The lack of improvement in his condition justified a consultation at our dermatology department, where the diagnosis of eosinophilic fasciitis was evoked due to the suggestive clinical appearance. A blood panel demonstrated a normal white blood cell count except for a slight hypereosinophilia of 1,800 × 109 cells/L. Hemoglobin and platelet counts were normal. A basic metabolic panel for renal and hepatic function was normal. The antinuclear antibody was negative. A biopsy of the fascia revealed an abundant infiltrate of eosinophils (Figure 1, Figure 2). We interrupted treatment with natalizumab and initiated hydroxychloroquine at a dose of 200 mg once daily. He demonstrated rapid clinical improvement in 3 weeks. Complete clinical resolution allowed discontinuation of hydroxychloroquine after 3 months. Blood eosinophilia normalized in 6 months. Because of his progressive MS, a decision was taken to resume treatment with natalizumab, which had been interrupted for 2 months. Fortunately, our patient presented no recurrence of the fasciitis to date and now receives natalizumab every other month because of better control of his MS.
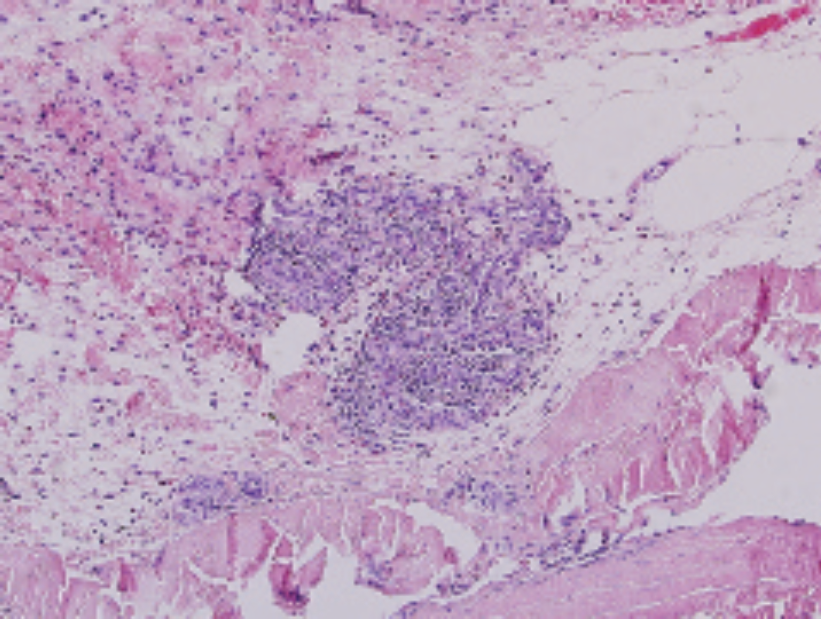
Thickened subcutaneous fascia with numerous eosinophils (hematoxylin-eosin stain, ×40 original magnification).
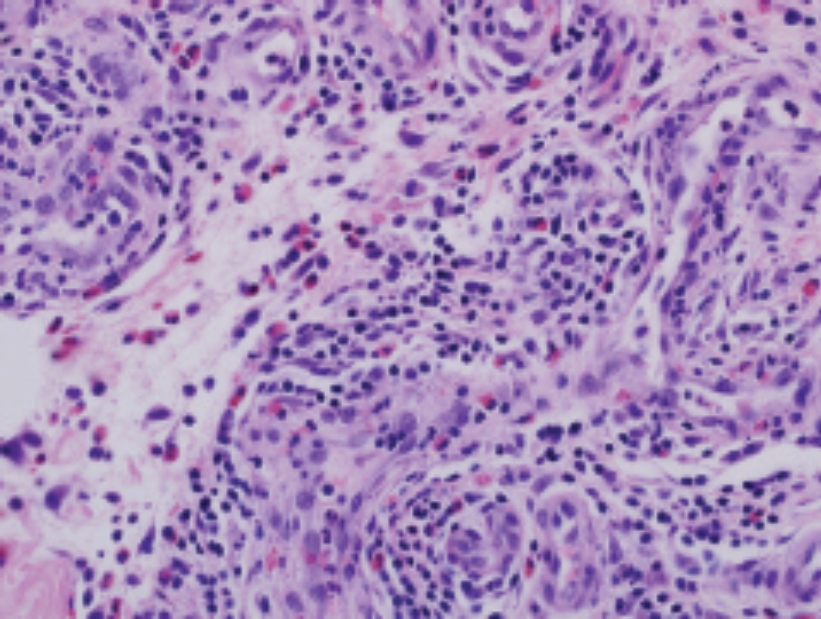
Dense eosinophilic infiltrate (hematoxylin-eosin stain, ×40 original magnification).
Although prednisone is the treatment of choice for this condition, our patient declined this medication because of reported intolerance (general malaise and fatigue). Other reported alternatives include hydroxychloroquine, methotrexate, cyclosporine, sulfasalazine, and topical tacrolimus, 5 usually in addition to the standard treatment of systemic corticosteroid. Our patient demonstrated an excellent clinical response to monotherapy with hydroxychloroquine, highlighting an interesting clinical option for patients with contraindications to systemic corticosteroids. In accordance with this, in one published case series, prednisone and hydroxychloroquine seemed equally beneficial in treatment. 6
Discussion
A recent review of drug-induced inflammatory myopathies with cutaneous manifestations reports that L-tryptophan is the first agent linked with eosinophilic fasciitis. 7 Druginduced eosinophilic fasciitis has also been reported from phenytoin 8 and antituberculous therapy. 9
Natalizumab is a selective adhesion molecule inhibitor that prevents interaction of leukocytes with endothelial cells. Consequently, it has been associated with blood hypereosinophilia. A generalized erythematous pruriginous skin drug eruption with accompanying peripheral eosinophilia has been previously described. 10 However, this is the first case report to our knowledge of a pathologic tissue infiltration of eosinophils in the form of an eosinophilic fasciitis associated with treatment with natalizumab. As our patient was able to resume natalizumab without recurrence, it is possible that this adverse effect represents a more complex interaction between medication-induced hypereosinophilia and other unknown environmental and/or genetic factors. As intense physical exertion is a known provoking factor, it is possible that it played an important role in unmasking this adverse reaction in our patient.
Conclusion
Although the underlying physiopathologic mechanisms are not well understood, it is possible that eosinophilic fasciitis represents a rare drug-induced complication of treatment with natalizumab and thus should be considered in patients with onset of woody edema under this medication.
Footnotes
Acknowledgment
Financial disclosure of authors and reviewers: None reported.