
Abstract
Background:
Pegylated interferon-α combined with ribavirin is the current standard treatment for chronic hepatitis C virus infection. During interferon and ribavirin therapy, both local and generalized mucocutaneous adverse reactions have been reported. Erythema annulare centrifugum induced by this therapy regimen has not been reported previously.
Case Report:
A 29-year-old woman was referred to our clinic for a 1-week history of slightly pruritic annular erythematous eruptions on the lower extremities and hands. The eruptions had first occured on the hands 3 to 4 days after pegylated interferon-α-2a plus ribavirin combination therapy for hepatitis C virus infection. Histopathologic examination supported the diagnosis of erythema annulare centrifugum. The lesions completely regressed within 2 weeks after the cessation of treatment but recurred on similar localizations within 24 hours with the same therapy. It was thought that erythema annulare centrifugum was induced by pegylated interferon-α-2a plus ribavirin combination therapy.
Conclusion:
Erythema annulare centrifugum is considered an inflammatory skin disease with unknown etiology. It is thought to represent a hypersensitivity reaction to some triggering factors, including infections, immunologic disorders, malign neoplasms, foods, pregnancy, and drugs. We report the first case of erythema annulare centrifigum induced by pegylated interferon-α-2a plus ribavirin combination therapy.
ERYTHEMA ANNULARE CENTRIFUGUM (EAC) is an eruption characterized by slowly enlarging annular or polycyclic erythematous lesions. It is thought to represent a hypersensitivity reaction to many etiologic factors, although the etiopathogenesis is not clear in most patients. 1,2 Cases of EAC due to some drugs, such as chloroquine, cimetidine, etizolam, and ustekinumab, have been reported in the literature. 2 We report a case of EAC induced by pegylated interferon (IFN)-α-2a plus ribavirin combination therapy. This is the first reported case of EAC associated with IFN plus ribavirin combination therapy.
Case Report
A 29-year-old woman was referred to our clinic with a 1-week history of slightly pruritic annular erythematous eruptions on the lower extremities and hands. Pegylated IFN-α-2a (180 μg/wk) plus ribavirin (1,000 mg/d) combination therapy had been initiated for chronic hepatitis C virus (HCV) infection 10 days previously. The skin lesions first occurred on the hands 3 to 4 days after the initiation of hepatitis therapy. These lesions gradually extended outward and healed centrally to form annular patterns. The size of the lesions ranged from 2 to 3 mm to 3 to 4 cm in diameter and were particularly localized bilaterally on the knees, ankles, and dorsa of the hands (Figure 1 and Figure 2). The patient's past medical history revealed an operation for aortic aneurysm 7 years previously. The results of the laboratory examinations, including complete blood count, blood chemistry profile, Veneral Disease Research Laboratory (VDRL), antinuclear antibody, anti-double-stranded deoxyribonucleic acid (DNA), anti-SS-A and -B antibodies, and thyroid function tests, were normal or negative except the elevated levels of alanine aminotransaminase (46 U/L; normal: 10–35 U/L), aspartate aminotransferase (58 U/L; normal: 10–35 U/L), and HCV ribonucleic acid positivity. A potassium hydroxide (KOH) examination of the lesion was negative.

Annular erythematous eruptions on the knees and hands.

Annular erythematous eruptions on the ankles.
A biopsy specimen was obtained from the lesions for the differential diagnosis of dermatoses such as EAC, granuloma annulare, and erythema multiforme, and the treatment of hepatitis was stopped. The histopathologic examination of the lesion showed epidermal spongiosis and lymphocyte exocytosis in addition to red cell extravasation and mild lymphocytic infiltrate in the upper dermis (Figure 3). EAC was diagnosed clinically and histologically. It was thought that pegylated interferon-α-2a plus ribavirin combination therapy induced EAC. This hypothesis was supported by complete improvement of the lesions within 2 weeks after the cessation of treatment and recurrence of similar annular lesions on similar localizations within 24 hours with readministration of the same treatment. Topical steroid and oral fexofenadine therapies were administered to the patient without cessation of the combination therapy, and the eruption was tolerated by the patient during the management of hepatitis.
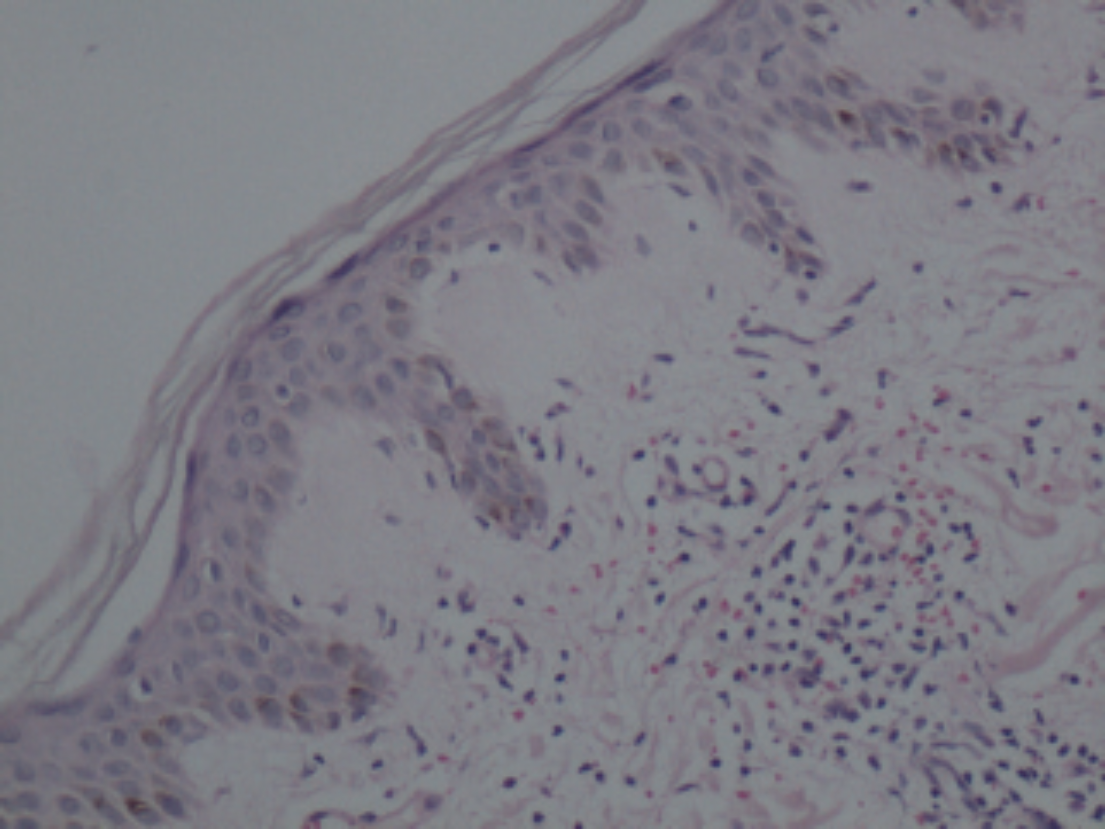
Mild lymphocytic infiltrate in the superficial dermis (hematoxylin-eosin stain; ×200 original magnification).
Discussion
Pegylated IFN-α-2a or −2b and ribavirin combination therapy has been shown to improve anti-HCV activity of IFN. 3,4 Coadministration of ribavirin and IFN-based treatment regimens has been accompanied by an increased incidence of skin reactions. 4,,–7 This therapeutic combination may cause local reactions at the sites of IFN injection and onset or worsening of skin disorders such as psoriasis and lichen planus. Moreover, inflammatory cutaneous eruptions may occur at distant sites from the points of IFN injection. 4,5
Localized reactions at the sites of IFN injection are common and are characterized by ill-defined, pruritic, erythematous patches or plaques. They are generally transient and do not require treatment. However, cutaneous necrosis may develop, albeit rarely, at the site of injection. 5
In the literature, a few studies investigated the cutaneous side effects of ribavirin and IFN combination therapy. Eczematous lesions characterized by pruritic, confluent, erythematous papular and microvesicular eruptions, which are often excoriated, were the most common cutaneous reactions reported due to this therapeutic combination in these investigations. 4,,–7 These eruptions were predominantly localized on the extremities and on truncal skin sites exposed to friction, and the onset of the inflammatory lesions ranged from 2 weeks to 4 months after implementation of the therapy. 4 Xerosis, lichenoid eruptions, prurigo, photosensitivity, malar erythema, and nonspecific eruptions were other observed skin reactions. 4,,–7 Also, alopecia, other hair changes, sarcoidosis, fixed drug eruption, pigmentation disorders, and a lot of uncommon cutaneous side effects have been reported, but EAC has not been reported previously. 5,8
Although the etiology of EAC is mainly unknown, a hypersensitivity reaction to etiologic factors has been suggested and has been related to infections, immunologic disorders, malign neoplasms, foods, pregnancy, and drugs. 1,2 The pathogenetic mechanisms of the disease and its peripheral migration are still unresolved, but it has been thought that they might be explained with localized production of proinflammatory cytokines and vasoactive peptides. 9 A histopathologic study of a case of EAC showed that most of the inflammatory cells around the vessels were T lymphocytes (cytotoxic/suppressor) and histiocytes. The presence of these cell types suggested that a cell-mediated immunity might be responsible for the pathogenesis of EAC. 1 In the present case, it is not known which drug triggered EAC as the patient used ribavirin and IFN combination therapy. Although IFN therapy was effective in a patient with EAC, paradoxically, IFN might have caused EAC by changing the immune system. IFN-α promotes the development of T helper 1 (Th1) cells and suppresses the production of T helper 2 cytokines. 10 The increased activity of Th1 cells might have caused the development of EAC lesions.
In the present case, the lesions occurred within a short time, 1 week after the onset of the combination therapy. Moreover, recurrence of the lesions occurred in even a shorter time when the therapy was readministered. This might be due to the patient's immunity or to IFN, which can directly affect the immune status of the patient.
If EAC is due to an underlying disorder, when the underlying disorder is successfully treated, the skin lesions will usually resolve. There are many therapeutic options, with variable results. Topical treatments include corticosteroids, calcipotriol, tacrolimus, and metronidazole. Systemic therapy alternatives are corticosteroids, antihistamines, and even etanercept. Although clinical remission may be achieved, relapses are frequent when the medications are discontinued. 11
Conclusion
Pegylated IFN-α and ribavirin combination therapy may cause the development of many dermatologic disorders. The present case is the first case of EAC induced by this combination. The development of EAC lesions does not require the cessation of treatment.
Footnotes
Acknowledgment
Financial disclosure of authors and reviewers: None reported.