
Abstract
Introduction
Key Points
Diagnosing and managing external genital warts involve making treatment decisions in concert with the patient. Treatment regimens should be tailored to the patient because each case varies in terms of the wart type, size, and location and the patient's preferences. Education and counseling are vital for addressing patients’ treatment-related questions and concerns, including the decision of whether or not to treat warts. A health care provider must consider the pyschosocial effects associated with a diagnosis of genital warts.
Although the incidence of human papillomavirus (HPV) infections, inclusive of external genital warts (EGWs), has been on the rise for the past two decades, 1 treatment can still be difficult. In the United Kingdom, the number of reported cases of EGW has increased 10-fold over the past 30 years.2,3 The reality is that treatment can be long and painful, with variable success rates. When choosing a treatment, the health care provider must consider not only the clinical symptoms but also the patient's preferences and the provider's experience and availability of therapy choices. Another important aspect of managing EGWs in patients is offering counseling and education to assist the patient in dealing with both the physical symptoms and the psychosocial ramifications of this HPV infection as they relate to diagnosis, treatment, periods of remission, and recurrence.
Treatment and Monitoring
Key Points
Although a number of therapies are available to treat EGWs, choosing the right one is based on an individualized approach that considers the patient's particular case as well as his or her perceptions and preferences. Use of a locally relevant algorithm is recommended to help select the most suitable treatment, increase compliance, and improve patient outcome. Given that success rates are variable and local reactions are common with all therapies, monitoring can enhance treatment success by identifying any tolerance issues and lack of a response and enable the health care provider to switch treatments, if required. Patients diagnosed with EGWs should also be screened for other sexually transmitted diseases (STDs) because coinfection is common. Coinfection with multiple HPV types, including high-risk ones, is a common occurrence that modifies both viral persistence and cancer risk.
Given that the primary goal of treatment is to eradicate visible warty lesions, ultimately, treatment success is measured by their disappearance and the wart-free periods that ensue. Each patient case requires an individualized approach. No one treatment stands out as the best or constitutes the gold standard as the response to treatment will vary from one patient to the next. Moreover, patients should understand that warts may clear on their own and that 90% of HPV infections clear within 2 years even without treatment. 4 A treatment algorithm can be helpful in deciding the right treatment path for a patient and what to do in the case of local reactions being intolerable, serious side effects, treatment failure, or other impediments to continuing with the same therapeutic choice. Clinicians are encouraged to develop their own treatment algorithm in respect of local practice standards and guidelines. The US Centers for Disease Control and Prevention (CDC) 2010 treatment guidelines for EGWs maintain that a locally developed and relevant algorithm can help improve clinical outcomes and treatment success (Figure 1). 5
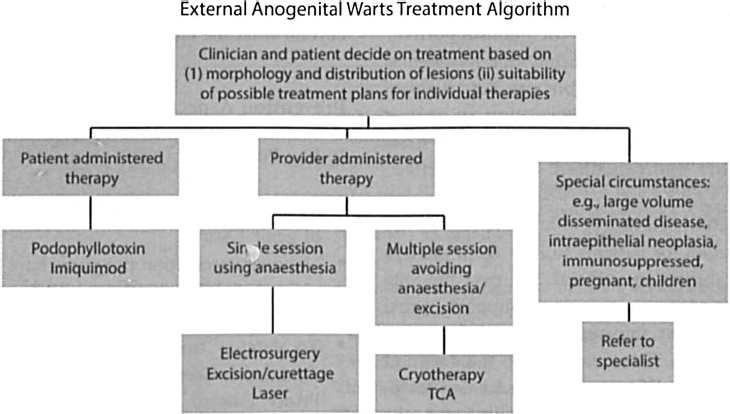
Algorithm for the treatment of external anogenital warts in the primary care setting. TCA = trichloroacetic acid.
Patient monitoring is advised, and follow-up visits should be part of routine care even for patient-administered therapies to answer any questions patients may have about treatment, assess the treatment area for the patient's response to treatment, and identify any possible issues. Considerations for home-based therapies include whether the patient fully understands how to use treatment, the chances of compliance, and the patient's ability to reach all areas that need to be treated. 6 Treatment modifications may be required under certain circumstances, including a lack of improvement after 3 months; if the patient cannot tolerate local reactions associated with treatment; or if the development of more severe adverse effects, such as pigmentation disorders, scarring, or chronic pain conditions, occurs. 5
Ease of use, tolerance, length of treatment, and cost all factor into treatment decisions. Available therapies include surgical options, which are provider administered, such as cryotherapy, bi- or trichloroacetic acid (BCA or TCA), electrocautery, CO2 laser, and excision. Topical treatments include podophyllin resin 10 to 25%, podofilox/podophyllotoxin 0.5% solution, and imiquimod 3.75%. The only patient-administered therapies available are podofilox/podophyllotoxin 0.5% solution and imiquimod. Although patient-administered therapies boast convenience and privacy, they have their challenges too. 7 For example, the dosing schedule for podofilox is twice-daily application for 3 days and then stopping treatment for 4 days up to four cycles. 5 Fortunately, improvements and innovations are making treatment easier without sacrificing efficacy. Imiquimod, for example, was originally approved in Canada in 1999 in a higher concentration of 5% but became available in 2011 in a 3.75% concentration, which reduced the occurrence of reactions, resulted in a simplified dosing schedule, and cut treatment length significantly from 16 weeks to 8 weeks. 8
Treatment considerations include choosing a therapy that best suits the patient and circumstances. Some factors that influence selection of treatment include the following5:
Wart size Number of lesions Wart location Wart morphology Patient preference Cost of treatment Convenience Adverse effects Provider experience
Capsule Summary
Health care providers can help address the questions, fears, and frustration that patients may have following a diagnosis of genital warts. Besides diagnosis and treatment of HPV infection, it is equally important to manage the patient's disease perceptions, treatment preferences, and related psychological sequelae. This discussion highlights the fact that a vital aspect of EGW management is strategically offering education and counseling via clear, practical information delivered in a supportive, nonstigmatizing way.
Patients newly diagnosed with genital warts, as well as their partners, should also ideally get screened for other sexually transmitted diseases (STDs) because coinfection is common among patients presenting with genital warts. The 2011 European Guideline for the Management of Anogenital Warts recommends screening current partners and other partners within the past 6 months for genital warts and offering education and counseling about STDs and their prevention. 9 Sturgiss and colleagues found that 53 (5.2%) of 1,015 new patients at a sexual health clinic tested positive for a coinfection with either Chlamydia or gonorrhea. 10 (Note that only 762 [75.1%] were screened for Chlamydia and 576 [56.7%] were screened for gonorrhea, so the number of other STDs cases could have been higher.)
Coinfection with multiple HPV types, both low and high risk, is also common, and the potentially related effects of infection persistence, new infections, and the development and progression of cancerous lesions have been weighed by various research efforts. For example, Muñoz and colleagues suggested that high-risk HPV infections last longer and reported that the median duration of a new HPV infection was 14.8 months for high-risk HPV types versus 11.1 months for low-risk HPV types. 11 The findings of Franco and colleagues proposed that viral persistence with high-risk HPV types may play a role in cervical carcinogenesis, 12 and more recent findings have confirmed this suspicion. 13 Some studies have suggested that infection with multiple HPV types, particularly high oncogenic-risk types, may act synergistically to increase the risk of precancerous cervical lesions or invasive cancer. 14
Trottier and colleagues reported that the risk of high-grade squamous intraepithelial lesions was notably higher among women with multiple-type infections compared to those with single-type HPV infections, 14 which other studies have similarly found. 15 Trottier and colleagues’ study, which included 2,462 Brazilian women from the Ludwig-McGill Cohort Study, found that risk increased relative to the number of HPV types present. Given the “unknowns” that remain around HPV infection, treatment and counseling decisions must consider current and evolving knowledge along with the individual patient case.
Education and Counseling
Key Points
Education and counseling are an integral part of successfully managing EGWs because patients will have different perceptions and questions relating to their HPV infection. Patient information should be provided both verbally and in written form. Educating and counseling patients can help improve patient outcomes by clearing treatment hurdles, improving compliance, and addressing the psychosocial concerns of patients. Health care providers should convey the right information in a manner that is informative, supportive, and nonstigmatizing.
Successful management of EGWs hinges on the involvement of patients in their care. How they view their disease, how they approach treatment and follow-up, and how well informed they become about managing their condition can ultimately affect treatment success. For example, because all therapies, whether topical or surgical, are associated with localized reactions, discussing these possible effects in advance of starting any treatment can help inform patients’ choice of treatment and prepare them for monitoring their progress and any hurdles. Concurrently, for the clinician, understanding patient perceptions of the disease and preferences about treatment can help guide treatment decisions and result in individualized care. A national survey aimed to gauge the perceptions of Canadians toward genital warts, related health behaviors, and treatment preferences.
16
Among its findings, the survey of 1,520 Canadian adults (786 females and 734 males) ages 18 to 75+ reported that:
52% would monitor an unrecognized spot on their genitals and seek medical help only if it did not go away 43% would stop having sex until the spots were gone 10% would not inform their partner—14% of men and 7% of women
A diagnosis of genital warts can produce a number of negative emotional reactions, including anger, shame, stigma, frustration, and fear.16–19 Concerns include worrying that warts will not go away or that they will return, having to disclose to a partner, infecting a partner, or the possibility of cancer. 19 In a large study of over 70,000 women in Iceland, Denmark, Norway, and Sweden, Kjaer and colleagues reported that 1 in 10 Nordic women suffer the psychosocial burden of being diagnosed with genital warts, noting effects that include lower self-esteem, negative self-perception, embarrassment, and anxiety. 20 The fact that treatment can involve several rounds, multiple follow-up visits (especially for provider-administered therapies), and abstinence can contribute to increased stress for patients. Because long-term management is a necessity and cure is not an option, 21 it is essential to help patients manage acute symptoms, monitor for symptoms from recurrence, and cope with the emotional stress of what is essentially a chronic condition.
Effective Communication Strategies
As is the case with management of many dermatologic conditions, patient education and counseling are useful clinician tools that are essential to help manage treatment reactions, reduce psychosocial stress, increase compliance, and improve patient outcomes. 22 Research suggests that health care providers play a pivotal role in educating and counseling patients to arm them with the necessary information they need to manage their disease and providing such pertinent information in a sensitive, empathetic way. In fact, Dunne and colleagues call health care providers “the most trusted source of information about HPV infection.” 23 Bertram and colleagues found that how information is conveyed greatly affects whether patients perceive it as “supportive” or “nonsupportive” information. 24 For example, a reassuring tone was seen as supportive, but using medical jargon was not. Bertram and colleagues suggest framing information so that it “informs but decreases stigmatization.” They also stress the importance of “individualized and supportive” counseling.
Providing education in a variety of forms reinforces key messages and strategies for patients to help them manage their genital warts during an outbreak and over the long term because recurrence is common. Support verbal information with written information to reinforce key messages for patients. 25 These can be in the form of pamphlets, hotlines, websites, videos, and so forth. According to the 2012 European guideline for the management of anogenital warts, information should be clear, in written format. 25
According to the findings of Cortes-Bordoy and colleagues, offering an educational leaflet about warts to patients undergoing treatment modified sexual risk behavior. 1 The results showed that, at follow-up visits, there was a significant increase in the use of condoms and a decrease in the average number of sexual partners in the intervention group compared to baseline; education did not seem to improve recurrence rates. In a study by Winer and colleagues, consistent condom use in male partners resulted in a 70% reduction in HPV transmission among sexually active female college students. 26 Note, however, that in long-term, steady relationships, condom use may not protect the partner who will already have been exposed to and will probably contract the HPV infection.
Much like the mixed messaging we may provide about condom use vis á vis protection, Gravitt suggests that the lack of certainty about the natural history of HPV infection challenges the ability to develop and disseminate well-defined educational messages. 27 Patients will conceivably have more questions than can be answered unequivocally because gaps in our current knowledge remain about the natural history of HPV infection and, consequently, what we can tell patients about natural immunity (HPV-seropositive antibodies), reinfection, and HPV latency. 27 Still, physicians can anticipate some common questions that may arise in the course of counseling a patient diagnosed with genital warts.Table 1 lists some of these patient concerns and aims to help guide the type of discussion that may unfold between physician and patient. However, given the individual circumstances of each patient, the discussion and counseling messages would equally need to be tailored, so the information to be conveyed would likely extend beyond what the table captures.
Counseling Information: Patient Information Chart
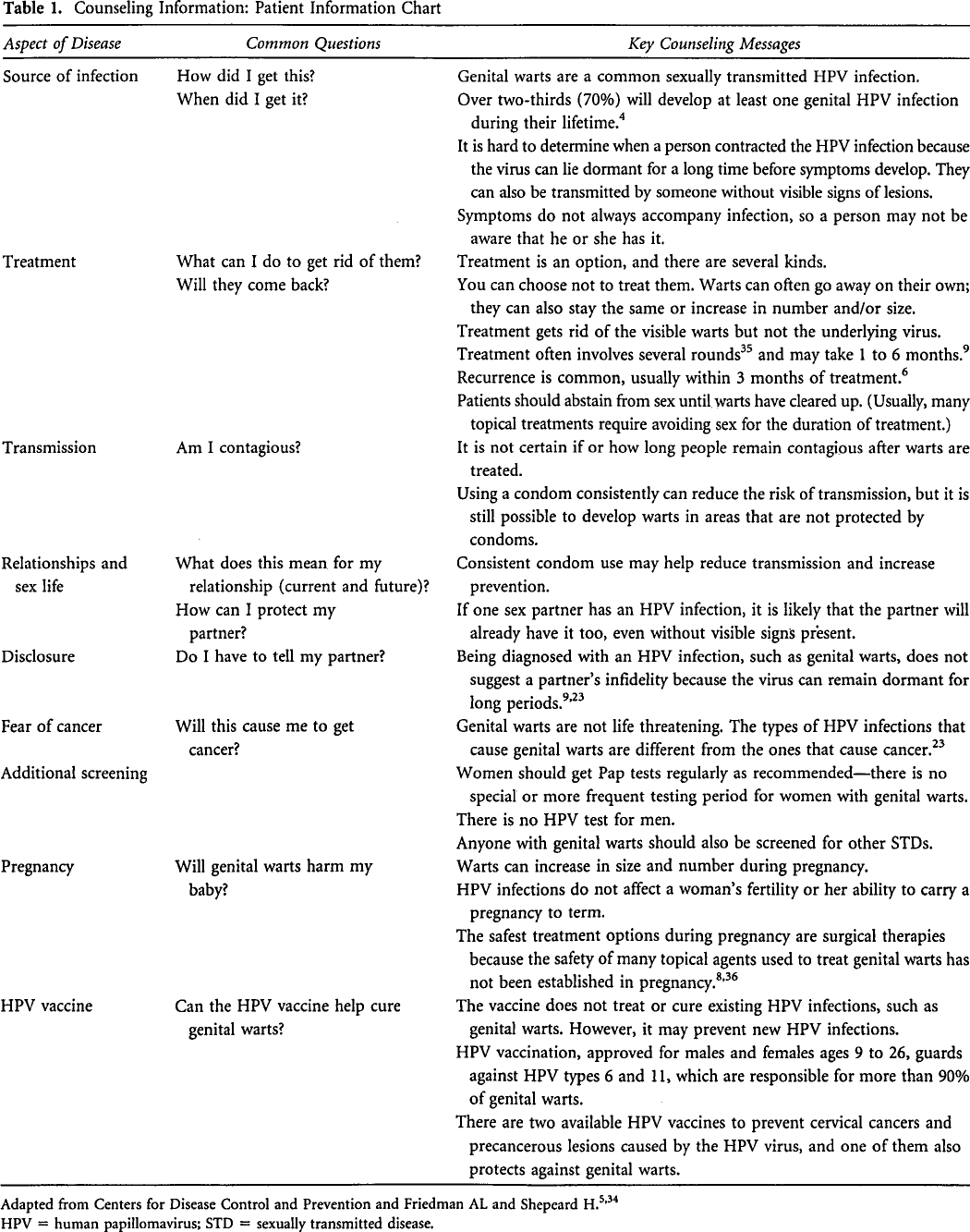
Adapted from Centers for Disease Control and Prevention and Friedman AL and Shepeard H.5,34
HPV = human papillomavirus; STD = sexually transmitted disease.
Prevention Aspects of Management
Key Points
Vaccination is increasingly relevant for the prevention of genital warts. National vaccination programs have provided data that assert decreasing trends in genital warts in both women and men. To date, a free national HPV vaccine program in Canada has been approved only for females, except for Prince Edward Island, where a school-based program now offers vaccination to males as well.
Many believe that offering a unisex and universal HPV vaccine program could greatly reduce the burden of disease.28,29 Findings from an Australian study show that vaccination is effective for reducing genital warts and preventing cancers. The vaccination program began in 2007 and has been credited with a fast and steady decline in the number of young heterosexuals diagnosed with genital warts at sexual health outpatient clinics. Ali and colleagues found a similar downward trend in hospital inpatients, according to findings that examined annual treatment rate trends using data from Medicare records and Australian population data. 30 In women ages 15 to 24, this study indicated a steady drop in the annual treatment rates of vulval or vaginal warts during the vaccination period (2007–2011), with an overall decrease of 85.3% and a decrease of 70.6% for penile warts in men of the same age group. In 25- to 34-year-old men and women, there was a decreasing trend of 33 and 59%, respectively. Both in men and women, ages 35 to 44, no significant changes in treatment rates were observed for genital warts. The authors note that although the dramatic drop in numbers among women is attributable to the vaccine program, herd immunity is the likely explanation for the decreasing trend in men because free HPV vaccination was not extended to men.
A similar experience in a Danish population was reported after a national HPV vaccination program began in 2009, providing the quadrivalent HPV vaccine to all 12-year-old girls; catch-up vaccination was also offered to girls up to 15 years of age, starting in 2008. 31 Using the Danish National Patient Register, Baandrup and colleagues examined trends between January 1995 and July 2011. 31 The data showed a significant, increased incidence of EGWs in women until 2007 and then an average annual drop of 3.1%, which was attributed to the national HPV vaccination program. The quadrivalent HPV vaccine used in Denmark not only protects against HPV types that cause cervical cancer (16 and 18) but also the types that commonly cause EGWs (6 and 11), which suggests that it could prevent most cases of EGWs. 2
Both the Danish and Australian examples report the effects of vaccination in younger women—the targeted groups of national vaccine programs. However, as some findings suggest that evidence of viral latency, reactivation of previous HPV infections, and diminished seropositive protection in women older than 26 (the recommended age cutoff in Canada), vaccination should perhaps be reconsidered for older women. In Canada, Gardasil was approved for use in women up to the age of 45. 32
Barriers to Vaccination
In Canada, there are two approved vaccines: Gardasil and Cervarix. Gardasil provides protection against four HPV types: high-oncogenic risk HPV-16 and HPV-18 and low-risk HPV-6 and HPV-11. Cervarix provides protection against HPV-16 and HPV-18 but not against genital warts. 33
However, although a national vaccine program has made both vaccines available to females (Gardasil was approved in 2006 and Cervarix became available in 2010), the same is not yet being extended to school-aged males. The rationale is a paucity of data with regard to the epidemiology and natural history of HPV and burden of HPV-related disease in males. 33 Only Prince Edward Island has adopted the free HPV vaccine for males, but other provinces and territories have not followed suit yet. In the United States, the CDC recommends the HPV vaccine for all boys, ages 11 and 12, and males through age 21 for catch-up. Gay and bisexual men, as well as those who are immunocompromised, are also advised to get the vaccine if they are 26 years of age or younger and were not vaccinated earlier. 5
The quadrivalent vaccine (Gardasil) is also safe and effective for men and protects against the types of HPV infections that typically cause genital warts, if they have not contracted the disease yet. As well, the vaccine targets HPV types associated with cancers. It can protect against cervical cancer in women and cancers of the penis and oropharynx in men. The National Advisory Committee on Immunization (NACI) stated in a report update in January 2012 that a recommendation for Cervarix in males would be forthcoming once more data on efficacy against infection and disease end points become available. 32
Conclusion
EGWs are a sexually transmitted infection that can remain dormant or asymptomatic indefinitely, making it difficult for the clinician to properly determine when or how the patient contracted the virus. Often a diagnosis of genital warts can be challenging for patients, in terms of both treatment and monitoring and the psychosocial components that accompany this STD, such as shame and fear. In addition to informing patients about treatment options and regimens, education and counseling can prove invaluable in terms of managing treatment expectations, helping patients understand disease transmission and protective measures, and cope with recurrence.
Footnotes
Acknowledgment
Financial disclosure of authors and reviewers: None reported.