
Abstract
Background:
A permanent, unpleasant atrophic leishmaniasis scar is a potentially disfiguring condition that causes social stigma with limited treatment choices. Fractionated carbon dioxide (CO2) laser resurfacing is expected to be a safe and effective treatment for leishmaniasis scars.
Objective:
To assess the safety and efficacy of ablative fractional resurfacing (AFR) with a CO2 laser for facial leishmaniasis atrophic scars.
Methods:
Eleven patients (five males, age 18–47 years) underwent the fractional CO2 laser procedure. The mean duration for scars was 18.3 years. Three to five treatment sessions with the fractional laser eCO2 (10,600 nm, Lutronic Corporation, Gyeonggi-do, Korea) were performed for each patient, at 2-month intervals, under topical anesthesia. Two passes (with tip type 120, density 150 spots/cm2 in static mode, and peak power of 30 watts) were performed on each leishmaniasis scar. Pulse energies ranged between 100 and 140 mJ. Posttreatment improvements in texture, atrophy, and overall satisfaction with appearance were graded on a quartile scale 1 month after the second session and 3 months after the final session. Scar improvement was graded using a 4-point score with a maximum score of 20.
Results:
At the 3-month posttreatment follow-up, all subjects were rated as having at least 50% improvement in texture, atrophy, borders, and overall appearance of scars. The median score of improvement was 18 of 20 (range 11–19). Mild postinflammatory hyperpigmentation was the only adverse effect, observed in 18% (2 of 11) of subjects. After the procedure, moderate to severe erythema and edema typically resolved within 24 to 48 hours. No additional adverse effects were observed.
Conclusion:
Fractional CO2 resurfacing represents a safe, effective, and well-tolerated potential treatment for atrophic facial leishmaniasis scars in ethnic skin.
ATROPHIC FACIAL SCARS resulting from cutaneous leishmaniasis in Middle Eastern populations are an important aesthetic concern. Leishmaniasis is a nonlethal disease, but it can have grave consequences for the patient as it can leave a permanent scar with disfigurement, resulting in social stigma.
Many therapies have been employed to treat other atrophic scars, such as chemical peeling, surgical excision, mechanical dermabrasion, tissue augmentation with fillers, and laser resurfacing. Most of these modalities can result in incomplete improvements, postoperative infections, worsening of scars, or pigmentary changes.1,2
Conventional ablative carbon dioxide (CO2) lasers have been successfully used for many years to treat surgical, atrophic, and acne scars.3,4 However, significant side effects, including dyspigmentation, prolonged erythema, and scarring, can occur. 5 The avoidance of scarring, hypopigmentation, and lengthy recovery periods are major factors behind the development and rising popularity of newer fractional CO2 lasers.
Fractional photothermolysis (FP) is a well-tolerated and effective modality for an expanding variety of conditions, such as photoaging, periorbital wrinkling, mild to moderate acne scarring, melasma, pigmented lesions, and poikiloderma of Civatte.6–8 Patients generally require multiple treatments to achieve significant results with nonablative energies. By depositing a pixelated pattern of microscopic ablative wounds surrounded by healthy tissue in a manner similar to that of FP, 9 ablative fractional resurfacing (AFR) combines the increased efficacy of ablative techniques with the safety and reduced downtime associated with FP.
AFR was created by combining the 10,600 nm wavelength of the CO2 laser with an FP system. Because of the areas of spared epidermis and dermis inherent in a procedure that employs AFR, healing is more rapid compared to fully ablative CO2 laser skin resurfacing, and the downtime is proportionately reduced. 10
Treatment with AFR was previously demonstrated to safely improve the appearance of atrophic acneiform scarring 11 by reducing the depth of individual scars. In this pilot prospective study, we intended to evaluate the efficacy and safety of AFR in the treatment of atrophic leishmaniasis scars in dark-skinned individuals.
Methods
Eleven patients (five males) with leishmaniasis scars were recruited. Their ages ranged from 18 to 36 years, and they were classified as Fitzpatrick skin IV. Before the treatment, the skin was cleansed with an alcohol swab. Topical anesthetic cream containing 2.5% lidocaine and 2.5% prilocaine (EMLA, AstraZeneca LP, Wilmington, DE) was applied, under occlusion, to the treatment site for 1 hour before treatment. Patients with old, mature leishmaniasis scars who were older than 18 years of age were included in the study. Any patient with active infection or a history of keloid formation, allergies to lidocaine, isotretinoin use within the past 12 months, connective tissue disease, or cosmetic procedures in the treatment area or who were pregnant or smoked within 12 months of enrolment was excluded. Informed consent was obtained from each patient. The study was approved by the Institutional Review Board of King Khalid University Hospital.
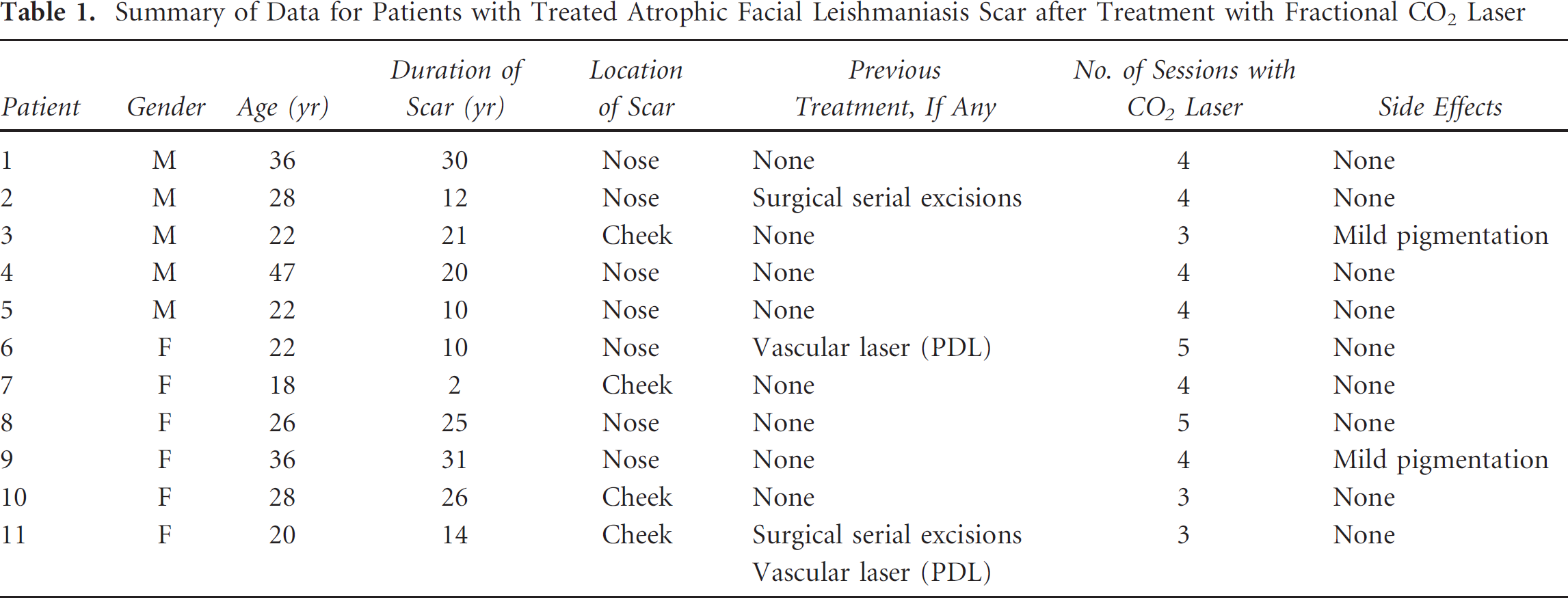
All patients with atrophic leishmaniasis scars received three to five AFR treatments 2 months apart. Patients returned for evaluation 1 month after the second session. The presence of mild erythema is not a contraindication for subsequent treatment. Table 1 displays the demographic details of the patients and the location, duration, and previous treatments for each scar.
Summary of Data for Patients with Treated Atrophic Facial Leishmaniasis Scar after Treatment with Fractional CO2 Laser
The treatment protocol was based on our previous clinical experience with AFR treatments for acne scars. All treatments were performed with an ablative laser, eCO2 (10,600 nm, Lutronic Corporation, Gyeonggi-do, Korea). One pass with tip type 120 (refers to a 120 μm treatment tip spot size), density of 150 spots/cm 2 in static mode, and peak power of 30 watts was applied to each leishmaniasis scar. Pulse energies ranged between 100 and 140 mJ per pulse. Static mode offers deeper penetration and greater patient comfort, and dynamic mode is ideal for larger area blending and smoothing.
Patients were instructed to wash their face with a mild cleanser and then apply a thin layer of fusidic acid ointment over the whole face three times daily for 5 days to avoid posttreatment infection. Posttreatment erythema and edema as well as improvements in texture, atrophy, and overall satisfaction with appearance were recorded by subjects and investigators (dermatologists) 1 month after the second session and 3 months after the final session.
Improvements in the quality of skin texture and pigmentation, degree of skin atrophy, and overall appearance were graded on a quartile scale (0 = no improvement; 1 = 1–25% improvement [mild]; 2 = 26–50% improvement [moderate]; 3 = 51–75% improvement [marked]; and 4 = 76–100% improvement [very significant]) by patients and investigators 1 month after the second session and 3 months after the final session. The maximum score for all five parameters (color difference with surroundings, atrophy/depression, texture, borders, and overall appearance) was 20 (Table 2).
Improvement in Individual Atrophic Leishmaniasis Scar Characteristics in Patients at 3 Months Posttreatment
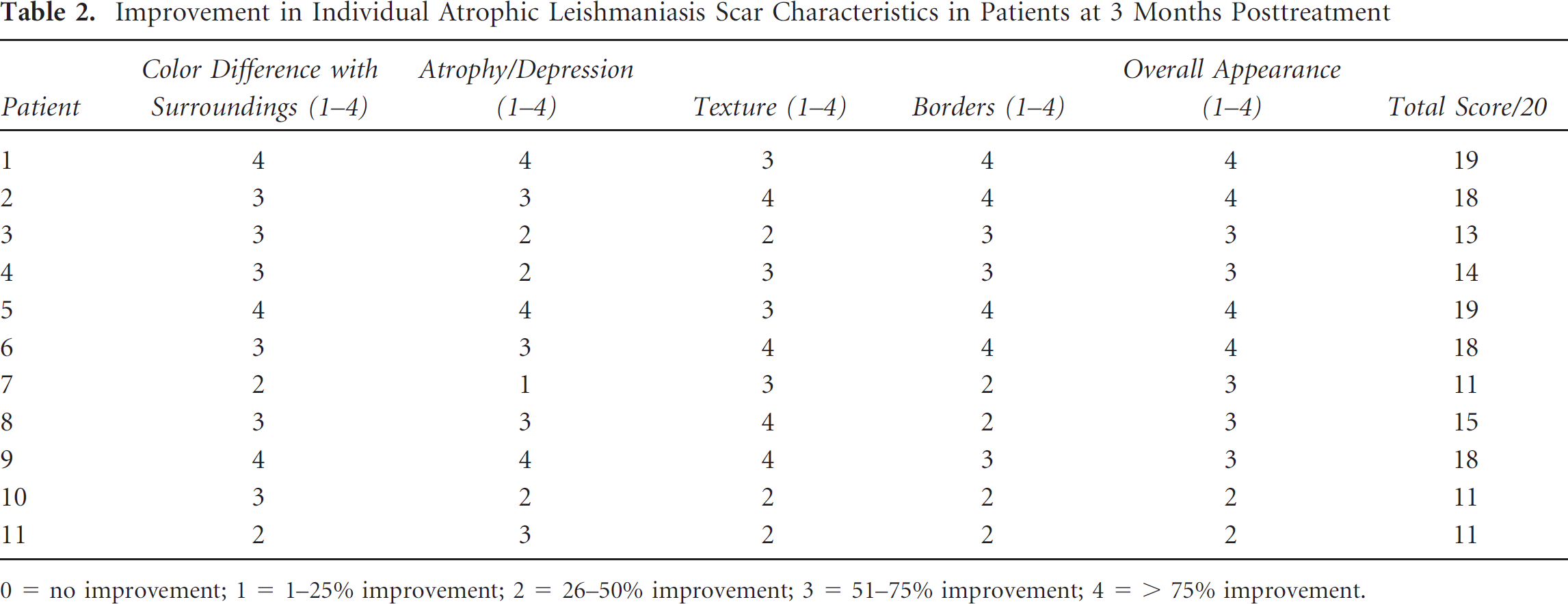
0 = no improvement;
1 = 1−25% improvement;
2 = 26−50% improvement;
3 = 51−75% improvement;
4 = > 75% improvement.
Standardized photographs using the Canfield Visia CR system (Canfield Imaging Systems, Fairfield, NJ) were assessed by two independent observers 1 month after the second session and 3 months after the final session. Descriptive statistics were used to analyze the data.
Results
Efficacy
Both the patient and the dermatologist noted the improvement in skin texture, borders, pigmentation, atrophy, and overall appearance of scars. Improvement was observed after the first treatment, and subsequent treatments resulted in incremental improvements in overall appearance. Quartile grading scores correlated to a median score of 18 out of a total score of 20 (see Table 2). Of 11 patients, 4 showed > 75% improvement in overall appearance. Almost all patients achieved at least 50% improvement (see Table 2). Digital photographic analysis showed that all patients had quantifiable, objective improvement in the depth and texture of leishmaniasis scars.
Table 2 demonstrates investigator grading of texture, atrophy, and overall satisfaction with appearance 3 months after the last treatment.
Figure 1 and Figure 2 demonstrate improvement in atrophy and texture of leishmaniasis scars 3 months after the last treatment.
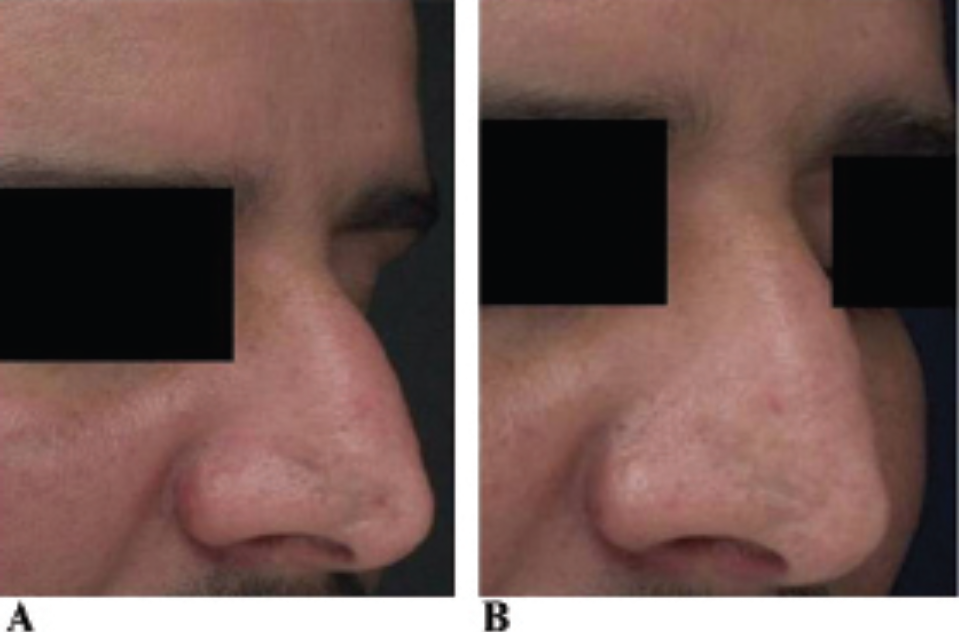
A, Atrophic leishmaniasis scar on the cheek and nose before fractional CO2 laser treatment in patient 1. B, Resolution of the leishmaniasis scar on the cheek and nose 3 months after the fourth session of fractional CO2 laser in patient 1.
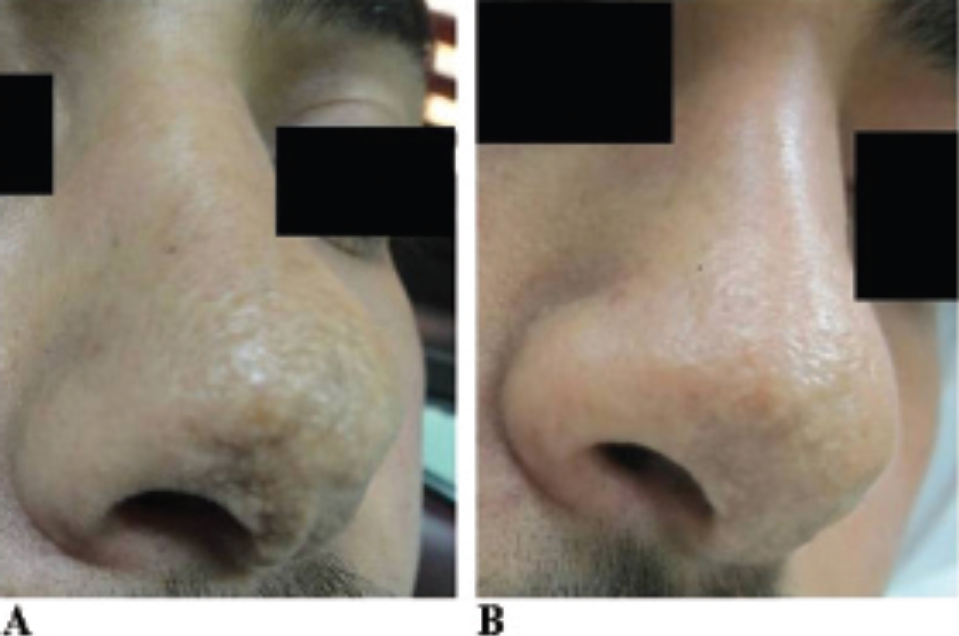
A, Atrophic leishmaniasis scar on the nose before fractional CO2 laser treatment in patient 2. B, Near-resolution of leishmaniasis scar on the nose 3 months after the fourth session of fractional CO2 laser treatment.
Safety
All 11 patients with leishmaniasis scars completed the scheduled visits for AFR treatment. After each treatment, immediate postprocedure erythema was noted. Erythema peaked at 24 hours after each treatment and typically resolved within 48 to 72 hours. This showed that the energy used here was modest in view of any possible complication avoidance in ethnic skin.
Mild to moderate edema was routinely observed and peaked immediately after treatment. By 3 to 5 days after each treatment, edema had resolved in all patients. No marked pigmentary changes were observed at the follow-ups except mild pigmentation in two patients. Mild pinpoint bleeding was noted in most patients. No treatment-induced scarring was observed throughout the study period. No bacterial infections or episodes of viral reactivation occurred during the study. Complications including persistent erythema, permanent hyper- or hypopigmentation, hypertrophic scarring, or keloids were also not observed in our patients.
Discussion
This is, to the best of our knowledge, the first case series demonstrating the safety and efficacy of AFR treatments for atrophic leishmaniasis scars. Enhanced efficacy was most likely due to deeper dermal penetration of energy that could not be achieved with traditional ablative devices without unwanted side effects. Despite our small sample, a median score of 18 out of 20 in response to various treatment energies was identified. All patients experienced some improvement (at least 50%). Our data suggest that AFR is a safe and efficacious treatment for leishmaniasis atrophic scars on the face in dark-skinned individuals. We used modest and conservative parameters to avoid any side effects in skin of color.
A permanent, unsightly leishmaniasis scar is a potentially disfiguring condition with limited treatment options that can cause psychosocial problems. The scar is usually atrophic and can be of variable size, ranging from a few millimeters to several centimeters.
Fractional lasers showed promising results in the treatment of atrophic scars in general. Surgical interventions are not as effective and can result in anatomic or functional disruption and tend to leave a new scar. Some locations (especially the nose) are difficult to treat surgically. Serial excisions with suturing require multiple surgeries and lead to scarring, and it is difficult to close thick nasal skin. Grafts can result in mismatching of skin texture and tone and are not widely acceptable. There can also be postsurgical scarring after graft suturing. Expanders can be used for atrophic scars but often with only partial success due to deformity, especially on the face. Other resurfacing techniques, including trichloroacetic acid (TCA) peeling, phenol peeling, radiofrequency, and electrosurgery,1,2 have been used but with limited success and significant side effects, in particular pigmentary changes in ethnic skin. Injectable fillers are a good option but are not permanent.
There are case reports in the literature on traditional CO2 laser treatment of “acute” leishmaniasis,12,13 but the data on the treatment of leishmaniasis scars by a fractional laser modality are sparse. One of the authors published a previous case report on the treatment of leishmaniasis scars by a nonablative fractional laser modality. 14 A recent study was conducted to compare the efficacy of 50% TCA solution and conventional CO2 laser for treatment of the atrophic scars due to leishmaniasis. 15 The scar improvement was 48.13% in the TCA group and 44.87% in the CO2 laser group. This difference was not statistically significant (p = .55). 15
Conventional ablative skin resurfacing is generally considered to be the most effective laser treatment option. Recontouring of atrophic facial scars with traditional CO2 and erbium: YAG laser vaporization has been used previously. This method typically requires a single session but is associated with extensive clinical downtime (4–7 days) and social downtime (up to 4 weeks), with lesion depths up to 1 mm or more per pass. There is prolonged recovery time, along with more side effects. The risk of dyspigmentation is high. 16
CO2 and erbium: YAG lasers emit infrared light, which targets water, resulting in tissue contraction and collagen formation. The first ablative laser systems created significant thermal damage, resulting in unacceptably high rates of scarring and prolonged healing. Newer fractional ablative lasers are capable of achieving significant improvements with fewer side effects and shorter recovery times. 17
Most likely the most prominent effect of fractional lasers is the formation of microscopic epidermal necrotic debris, which represents elimination of the thermally damaged dermis and epidermis. The thermally damaged collagen is completely replaced within 3 months without any dermal fibrosis. 18 This mechanism facilitates its use in treating leishmaniasis scars.
A clinical trial demonstrated significant results for the resolution of acne scars with a fractional CO2 laser. 19 In addition, it has shown promise in the resurfacing of thermal burns. 20 Compared to conventional ablative CO2 devices, 5 the side-effect profile with fractional CO2 lasers is significantly improved. Rapid recovery and reduced downtime noted with AFR are probably due to rapid reepithelialization from the surrounding undamaged tissue.
The treatment strategy in our protocol was based on previous studies with AFR in the treatment of acne scars. Ortiz and colleagues presented the first results of a pilot study with the fractionated CO2 laser for the treatment of acne scarring. 21 Fifteen subjects underwent up to three treatments. Patients with diverse skin types (I–V) were treated, with no short- or long-term hyperpigmentation complications reported; 87% of subjects experienced sustained significant improvement in the appearance of acne scarring at 3-month follow-up visits. All subjects reported transient erythema that resolved in the majority of subjects within the 1 to 3 months after treatment.
AFR technology with the fractionated CO2 laser significantly improved moderate to severe acne scarring in a large case series. 11 Improvements of 51 to 75% in texture, atrophy, and overall improvement were noted in all patients.
Delayed pigment abnormalities, which have been reported with traditional CO2 resurfacing, were not observed in patients following AFR treatment. Similar to results from our previous case report 14 and our personal experience, maximal benefit was observed 3 to 6 months after AFR treatment.
A limitation of this uncontrolled pilot study was the small sample size. In this study, patient satisfaction increased with each treatment. However, the optimum interval between consecutive treatments remains to be determined. The efficacy and low incidence of untoward effects make it a viable treatment for disfiguring leishmaniasis scars in this region of the world.
Conclusion
AFR with the use of a CO2 laser enables the creation of deep dermal ablation and coagulation and minimizes patient downtime. A lower adverse effect profile makes AFR an excellent choice for treating atrophic leishmaniasis scars on the face for ethnic skin. Further research into the ablative fractional laser for leishmaniasis scars with controlled and larger studies is needed. In addition, treatment settings for scars in darker skin types remain to be optimized.
Footnotes
Acknowledgment
Financial disclosure of authors and reviewers: None reported.