
Abstract
Objectives
This study examines plasma interleukin 33 (IL-33) levels in patients with osteonecrosis of the femoral head (ONFH) and explores the possible use of IL-33 as a marker for early diagnosis and progression of ONFH.
Methods
One hundred twenty-five ONFH patients and 126 control subjects were recruited for this study. The plasma IL-33 levels were measured using a commercially available enzyme-linked immunosorbent assay kit. Effects of disease stage and risk factors on IL-33 level were also assessed.
Results
Plasma IL-33 levels were significantly higher in the 125 ONFH patients (174.33 [SD, 65.73] pg/mL) than in the 126 control subjects (90.50 [SD, 25.17] pg/mL, P < 0.001). Plasma IL-33 levels were significantly higher in patients with stage III/IV ONFH (184.17 [SD, 43.75] pg/mL) than in patients with stage I/II ONFH (158.24 [SD, 50.11] pg/mL, P < 0.001). There was no significant difference in IL-33 levels between alcohol-induced, idiopathic, and steroid-induced cases.
Conclusions
Plasma IL-33 may be an alarmin for ONFH, and its levels may be related to disease progression.
Interleukin 33 (IL-33) is a member of the IL-1 superfamily and functions through inducing helper T cells, mast cells, eosinophils, and basophils to produce type 2 cytokines. The induction of type 2 cytokines by IL-33 in vivo is believed to produce severe pathological changes.1,2 Recently, IL-33 was demonstrated to be expressed in human bone, particularly in osteocytes, osteoblasts, and marrow adipocytes,3,4 and may play a role in osteonecrosis after it is specifically released by necrotic cells.5,6 However, there is very little evidence in literature on whether plasma IL-33 levels are elevated in human osteonecrosis of the femoral head (ONFH) and whether it is predictive of ONFH progression.
Osteonecrosis of the femoral head is a disabling disease affecting people of all ages, especially young adults, and often leads to the destruction of the hip joint. A large number of pathological conditions have been established as risk factors for ONFH, such as trauma or hip surgery, hypercortisonism, hyperlipidemia, and alcoholism. 5 Despite the important role played by these risk factors, a predictive factor for ONFH is not available.
We hypothesized that an elevation of IL-33 plasma level may be associated with the development of ONFH, thus allowing early diagnosis and eventually conservative treatment. In the present study, we examine plasma IL-33 levels in 125 patients with ONFH and in 126 age- and sex-matched control subjects using enzyme-linked immunosorbent assay (ELISA). The potential significance of IL-33 in ONFH pathogenesis and clinical diagnosis was evaluated.
Materials and Methods
Study Subjects
One hundred twenty-five patients with ONFH including 57 men and 68 women with an average age of 55.4 (SD, 9.7) years were recruited for this study from January 2011 to February 2013 from the 2nd Xiangya Hospital (Changsha, China). Osteonecrosis of the femoral head was diagnosed, and disease stage was determined according to the Ficat system 7 : stage I, the radiographs are normal; stage II, there is some evidence of bone remodeling including cystic and sclerotic areas; stage III, flattening of the femoral head can be observed; and in stage IV, there is joint space narrowing with secondary degenerative changes in the acetabulum. Among the 125 ONFH patients, 13 cases had stage I, 37 had stage II, 34 had stage III, and 41 had stage IV disease. Stage I was diagnosed with x-ray examinations and magnetic resonance imaging (MRI). According to etiologic factors, patients were subgrouped into idiopathic (65 cases), steroid-induced (27 cases), and alcohol-induced osteonecrosis (33 cases). Patients with direct trauma or possible combined causes, such as smoking, cardiovascular diseases, HIV infection, diabetes mellitus, renal disease, and so on, were excluded. One hundred twenty-six age- and sex-matched healthy individuals with an average age of 57.9±10.1 years old (61 males and 65 females) were simultaneously recruited as controls. All participants were Han Chinese. The study protocol was approved by the Ethics Committee of the 2nd Xiangya Hospital. Written informed consent was obtained from all participants or their guardians.
IL-33 Measurements
Blood samples were collected in sterile anticoagulation tubes, and plasma was obtained by centrifugation at 1600 rpm × 6 min. The plasma was immediately frozen and stored at −80°C until use. Concentration of plasma IL-33 was analyzed using commercially available ELISA kits (Enzo, Farmingdale, New York, USA) by following the user manual. The sensitivity of the kit is less than 1.7pg/mL (range 7.8 – 500 pg/mL). All samples were duplicated during measurements.
Statistical Analysis
Data were presented as mean (SD) and analyzed using SPSS 18.0 software (SPSS Inc, Chicago, IL). Categorical variables were presented as absolute and relative frequencies. Comparisons between variables were performed using 1-way analysis of variance or paired-samples t test. A P < 0.05 was considered statistically significant.
Results
Demographic Data
The 125 patients with ONFH consisted of 57 males and 68 females with an average age of 55.4 (SD, 9.7 years). Among the 50 patients with stage I/II disease, 25 patients had idiopathic, 12 patients had steroid-induced, and 13 patients had alcohol-induced osteonecrosis. Among the 75 patients with stage III/IV disease, 40 patients had idiopathic, 15 patients had steroid-induced, and 20 patients had alcohol-induced osteonecrosis. There was no significant difference in the amount of patients in each etiologic category between patients with stages I/II and III/IV disease (P > 0.05). The 126 control subjects contained 61 men and 65 women with an average age of 57.9 (SD, 10.1) years. Among the 126 control subjects, 42 subjects regularly consumed mild to moderate amounts of alcohol. There are no significant differences in the percentage of alcohol-consuming individuals between ONFH patients and control subjects (P > 0.05). No significant differences in age and sex were observed between 2 groups.
IL-33 Levels
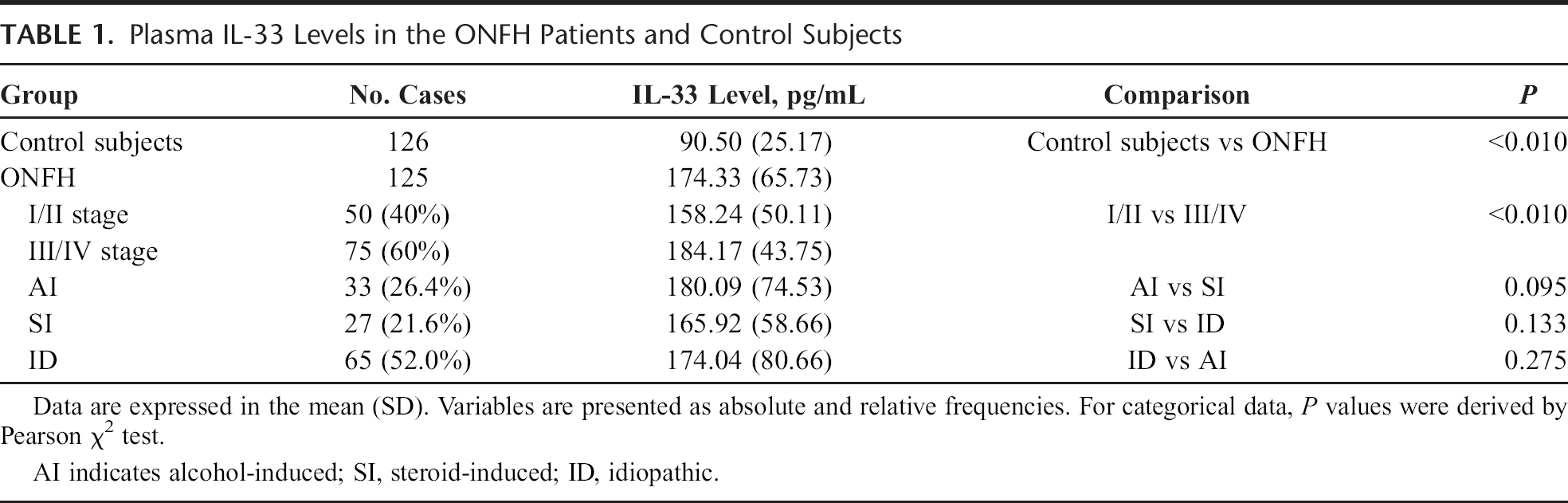
Plasma IL-33 levels were examined by ELISA and were demonstrated to be 90.50 (SD, 25.17) pg/mL (15.09–669.18 pg/mL), 158.24 (SD, 50.11) pg/mL (23.61–520.37 pg/mL), and 184.17 (SD, 43.75) pg/mL (17.45–630.77 pg/mL) in control subjects, stage I/II ONFH patients, and stage III/IV ONFH patients, respectively. Plasma IL-33 level was significantly higher in ONFH patients than in control subjects (P < 0.001). Also, plasma IL-33 level was significantly higher in patients with stage III/IV disease than in patients with stage I/II disease (P < 0.001). Although alcohol-induced ONFH showed a tendency of higher IL-33 level than steroid-induced ONFH (P = 0.095), no significant differences were observed between other causes, suggesting that IL-33 level is not significantly associated with different risk factors (Table 1).
Plasma IL-33 Levels in the ONFH Patients and Control Subjects
Discussion
Although the putative direct effects of IL-33 on osteoclastogenesis and its proposed direct release from necrotic cells during osteonecrosis have been discussed in literature, plasma IL-33 levels in ONFH patients have not been reported. Particularly, the significance of plasma IL-33 level in the pathogenesis and clinical management of ONFH has not been validated. In this study, significantly higher plasma IL-33 levels were observed in ONFH patients compared with control subjects. Importantly, sustained elevation of IL-33 level was observed as the disease progressed, with higher levels being identified in patients with more severe disease stages. No significant association was observed between ONFH patients with different risk factors. Our study suggests that IL-33 level may be predictive of the development of ONFH.
Osteonecrosis of the femoral head is a disabling joint disease that affects patients of all ages, especially those between 20 and 50 years. Early diagnosis and treatment are key to good clinical prognosis. Although MRI can identify stage I ONFH, it is expensive and inconvenient in most countries, making it ill-suited for early screening. Therefore, there is a need for developing a more convenient, easily accessible, and cost-effective method to diagnose ONFH. Interleukin 33 is specifically released from necrotic cells and constitutively expressed in osteoblasts and adipocytes, which are abundant in bone marrow. 8 Moreover, IL-33 also affects angiogenesis and vascular permeability. Interestingly, IL-33 levels have been revealed to be elevated in sera and synovial fluid samples from patients with rheumatoid arthritis and correlated with disease activity. 9 In this study, plasma IL-33 levels were found to be elevated in stage I patients compared with control subjects and were not affected by the etiology of ONFH.
An interesting finding in this study is that elevated plasma IL-33 level is not associated with risk factors of ONFH. Plasma IL-33 levels were elevated, but no significant differences were observed between alcohol-induced, steroid-induced, and idiopathic ONFH. Previous studies reported that long-term use of steroids may induce apoptosis.10,11 However, IL-33 was thought to be largely retained inside apoptotic bodies during apoptosis, preventing its accidental release. 5 In contrast, studies indicated that IL-33 levels undulate with the balance of osteogenesis and osteoclast processes. 12 Therefore, plasma IL-33 should be reduced in steroid-induced ONFH. A possible reason for the observed elevation of IL-33 level in steroid-induced ONFH in this study might be the withdrawal of steroid medication. In fact, all ONFH patients with steroid use being a risk factor had stopped using steroids for at least several months before they were recruited for this study (data not shown). Therefore, effect of steroids on apoptosis is limited, but the damage caused by the steroids, including fat embolism, fatty change, and increased intramedullary pressure to femoral head still exists.13–15 Therefore, low IL-33 levels in steroid-induced ONFH may automatically return to normal levels after the removal of steroids. In this situation, IL-33 may only reflect the current pathological condition and suggest a relationship with the progression of ONFH. However, our study provided no evidence on whether IL-33 is an inducer of ONFH. It is therefore unknown whether blockade of IL-33 expression could be envisioned to treat ONFH. The effect of IL-33 blockade should be investigated in animal models of osteonecrosis.
We acknowledge that there are some limitations to this study. First, the Ficat criteria appear to be very nonspecific. Many of the characteristics listed are similar to that of osteoarthritis. Although MRI was used for diagnosis of stage I ONFH, a criterion standard for MRI has not been established. Also, the positive and negative predictive value of the Ficat diagnostic criteria for ONFH has not been determined. In addition, MRI was not included in the diagnoses of stages II, III, and IV ONFH, their diagnoses were limited to radiograph. Second, the sample size is relatively small, and the analysis was not stratified for age, sex, and disease stages. Third, although the controls were matched in age and sex, they were not matched with etiology, such as alcohol consumption. Fourth, although plasma IL-33 was proposed to be a useful index for early diagnosis of ONFH, the elevated levels of IL-33 before bone collapse were not shown. Also, sensitivity and specificity of plasma IL-33 level have not been evaluated. For establishing the specificity, the number of ONFH patients with normal IL-33 plasma level should be compared with the number of control subjects with elevated IL-33 plasma levels. The IL-33 levels in other joint diseases such as rheumatoid arthritis and osteoarthritis should be compared. Fifth, a correlation between the area of the necrosis and plasma IL-33 levels in ONFH has not been analyzed. The IL-33 expression in necrotic femoral head has not been revealed by an immunohistochemical method. These can provide direct evidence for the involvement of IL-33 in ONFH. Even with these limitations, our study first demonstrated that plasma IL-33 level was higher in patients with stage III/IV ONFH than in patients with stage I/II ONFH. Also, IL-33 levels still increased during the course of ONFH. These findings suggest that plasma IL-33 is an indicator of disease progression, and dynamic changes in plasma IL-33 level could be used as a sign for clinical management of ONFH. In conclusion, our study suggests that the plasma IL-33 concentration is associated with ONFH and is a useful index for early diagnosis of ONFH.