
Abstract
The major biomarker for rectal cancer is the pathologic development of the tumor. In our study, we identified Dikkopf-1 (DKK1) as a novel biomarker and a therapeutic target for rectal cancer. To emphasize the biological and clinicopathologic significance, we performed tumor tissue and serum analysis of 150 rectal cancer samples with enzyme-linked immunosorbent assay. Serum DKK-1 levels are found significantly higher in controls, in poor differentiation, and depth of invasion (in pT3 and pT4), present lymph node metastasis, and TNM stage (in pT3 and pT4) according to good differentiation, depth of invasion (in pT1 and pT2), absent lymph node metastasis, and TNM stage (in pT1 and pT2; P < 0.001 and P < 0.0001, respectively). Tissue DKK-1 levels are found in patients with rectal cancer than in control tissues (P < 0.0001). Dikkopf-1 correlated significantly with depth of invasion (P = 0.009), lymph node metastasis (P = 0.028), venous involvement (P = 0.019), and advanced pTNM stage (P = 0.001). There was no correlation between DKK-1 and age or sex (P > 0.05). This marker is also a potential candidate for development of rectal cancer cells and cancer progression.
The major biomarker determinant of rectal cancer is the pathologic development of the tumor. In 2010, there were 39,670 new cases and 51,370 deaths related to colon and rectal cancer in the United States. 1 When rectal cancer is detected early, more than 85% of persons with the disease live at least 5 years beyond diagnosis. 2
Currently, none of the existing serum markers, such as carcinoembryonic antigen or cancer antigen 19-9, can be used individually for screening.
Retrospective studies have shown that multivariate predictive models combining existing tumor markers improve cancer. 3 Recent papers have methods to detect in protein expressions in serum samples, and the association of certain proteins with disease development may contribute to discovering markers with diagnostic importance.4–7
To determine biological marker targets for the diagnosis, treatment, and/or prevention of rectal cancer and all other cancer types, we measured serum and tissue dikkopf levels from 150 patients with rectal cancer. To verify the biological and clinicopathologic significance, we performed tumor tissue and serum analyses of rectal cancer materials with enzyme-linked immunosorbent assay (ELISA). 8 In this process, we identified Dikkopf-1 (DKK1) as a novel biomarker and as a therapeutic target for rectal cancer.
Dikkopf-1 encodes a secreted protein and is known as a negative regulator of the Wnt signaling pathway in colon cancer.9,10
Recent evidence points to an important role of the Wnt signaling pathways in the regulation of inflammation. Thus, activation of the Wnt/β-catenin pathway induces proliferation and survival of endothelial cells, increases monocyte adhesion, and regulates endothelial migration of monocytes.11–14 Dikkopf-1 binds to low-density-lipoprotein-receptor-related-co-receptor 5/6 and Kremen proteins and induces low-density-lipoprotein-receptor-related-co-receptor endocytosis, which prevents the formation of Wnt/Frizzled-low-density-lipoprotein-receptor-related-co-receptor 5/6 receptor complexes.8,10,15 Recently, Takahashi, 16 Yu, 17 and Mickheev 18 reported DKK-1 expression in human cancer cells, but the role of the Wnt-related families of secreted proteins in angiogenesis is rather unknown. Based on the emerging importance of the Wnt signaling pathways and the secretion of the DKK-1 in rectal cancer cells, we hypothesized a role of DKK-1, as a major marker of Wnt signaling, in angiogenesis and in rectal cancer tissue specifically. Here, this hypothesis was investigated in patients with rectal cancer and found to change between clinicopathological features, as determined by focusing on the role of DKK-1.
Materials and Methods
Patients
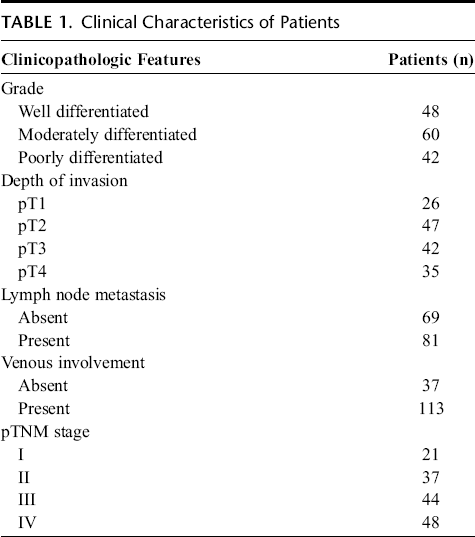
In this study, 150 samples of rectal cancer and adjacent normal tissues were obtained from inpatients undergoing surgical operation between October 2005 to September 2010 at the II. General Surgery Department, Haseki Research and Education Hospital, Istanbul and Yuzuncu Yil University Medical Faculty, Van. These inpatients did not undergo any chemotherapy or radiotherapy before the operation. This study was approved by the institutional review board, and all patients provided written informed consent. Cancerous rectal tissues and normal rectal tissues were allocated to cancer and control groups, respectively. The samples of rectal cancer and adjacent normal tissues were obtained away from regions of obvious inflammation and necrosis. All dissected specimens were cut in 5-mm cubic blocks, immediately snapped frozen in liquid nitrogen, and stored at −80°C. Tumor grade of differentiation was described according to the World Health Organization criteria. 19 The clinical and pathological stages were defined according to pTNM stage. The histopathological examination was translated by the Department of Pathology, Haseki Research and Education Hospital and the Yuzuncu Yil University Medical Faculty. Clinical characteristics of patients are given in Table 1.
Clinical Characteristics of Patients
Determination of DKK-1
Serum and tissue levels of DKK-1 were measured by commercially available ELISA kits (R&D Systems, Minneapolis, MN). In this study, 96-well plates were coated overnight at room temperature with monoclonal mouse antihuman DKK-1 capture antibodies (R&D Systems) in phosphate-buffered saline (PBS). The plates were washed with PBS/Tween and blocked with 1% bovine serum albumin in PBS for 1 hour at room temperature. The samples were added to the plates and incubated for 2 hours. Goat antihuman detection antibodies (R&D Systems) were added, and the plates were incubated for another 2 hours. Streptavidin-horseradish peroxidase was added and incubated for 20 minutes. After the plates were washed with PBS, the substrate reagent (R&D Systems) was added for another 20 minutes. The substrate reaction was stopped upon addition of 1-mol/L sulfuric acid, and extinction was measured at a 450-nm wavelength using a multiplate ELISA reader (Anthos Microsystems, Krefeld, Germany). All measurements were performed in duplicate for each sample, and the mean value was calculated.
Statistical Analysis
Shapiro-Wilk normality tests, Lilliefors-corrected Kolmogorov-Smirnov test (Kolmogorov-Smirnov with Lilliefors significance correction), and leaf and histogram graphs were evaluated by steam. The mean and standard deviation, median and IQR values were specified for variables with normal distributions. Comparison of variables between 2 groups of independent samples was performed using t tests, and the Mann-Whitney U test distributed data for groups of 3 or more were compared using one-way analysis of variance and Tukey honestly significant difference test was used for bilateral comparisons. For non-normally distributed groups, the Kruskal Wallis one-way analysis of variance and binary comparisons (post hoc), and the Bonferroni-corrected Mann-Whitney U test were used. The relationships between serum and tissue variables were assessed by the Pearson correlation test. The significance limit P < 0.05 was used. Analyses were performed using the SPSS 15.0 statistical package.
Results
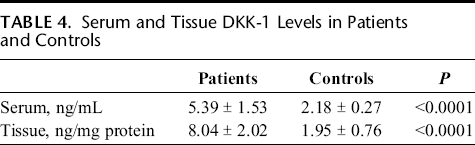
The relationships between serum and tissue DKK-1 levels and clinicopathological characteristics were analyzed (Tables 2 and 3). Total serum and tissues DKK-1 levels are given in Table 4.
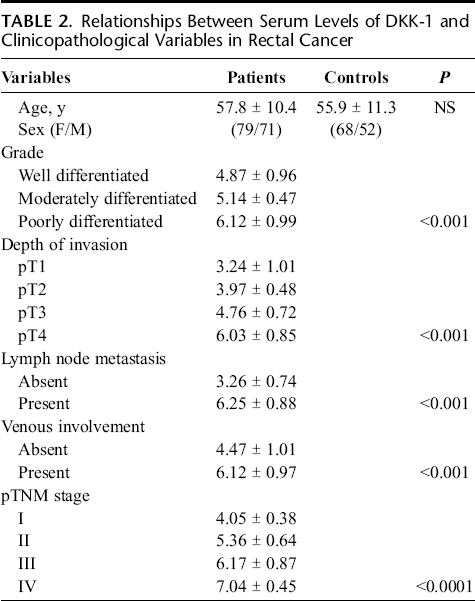
Relationships Between Serum Levels of DKK-1 and Clinicopathological Variables in Rectal Cancer
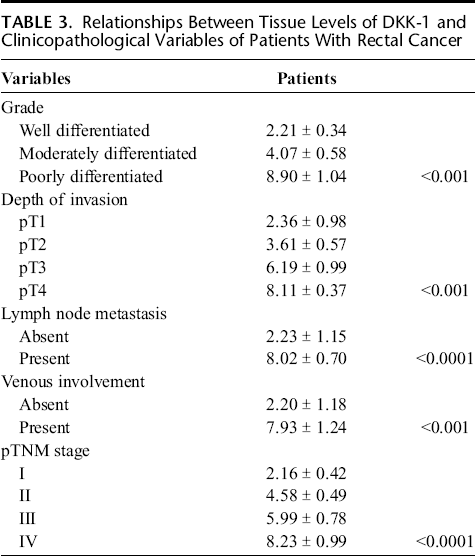
Relationships Between Tissue Levels of DKK-1 and Clinicopathological Variables of Patients With Rectal Cancer
Serum and Tissue DKK-1 Levels in Patients and Controls
Serum DKK-1 levels are found to be significantly higher in controls, in poor differentiation, depth of invasion (in pT3 and pT4), present lymph node metastasis, and TNM stage (in pT3 and pT4) as compared to good differentiation, depth of invasion (in pT1 and pT2), absent lymph node metastasis, and TNM stage (in pT1 and pT2; P < 0.001 and P < 0.0001, respectively).
Tissue DKK-1 levels are found in patients with rectal cancer than in control tissues (P < 0.0001).
Dikkopf-1 correlated significantly with depth of invasion (P = 0.009), lymph node metastasis (P = 0.028), venous involvement (P = 0.019), and advanced pTNM stage (P = 0.001). There was no correlation of DKK-1 with age and sex (P > 0.05).
Discussion
In our study, we provided evidence that circulating DKK-1 is a key mediator involved in rectal cancer and clinicopathological variables. In rectal cancer, DKK-1 was correlated with clinicopathological features and also with disease severity. We demonstrated that serum and tissue DKK-1 significantly correlated with clinicopathological variables such as depth of invasion, lymph node metastasis, venous involvement, and advanced pTNM stage (P < 0.05). Depth of invasion, lymph node metastasis, and pTNM stage of rectal cancer has potential predictive value for prognosis. 20 This suggests that DKK-1 is involved in the progression of rectal cancer and can serve as a marker of the disease.
Takahashi et al. 16 reported that expression of DKK-1 enhanced pancreatic ductal adenocarcinoma. Serum levels of DKK-1 were directly proportional to the severity of the disease. Expression of DKK-1 may also significantly stimulate the growth of breast cancer cells. 21 However, experimental metastasis studies may also have limitations in reflecting the entire process of metastasis, as the effects on malignancy growth before metastasis cannot be determined. Thus, extrapolation of DKK-1 with a metastasis assay was essential so as to identify the specific regulation mechanism.
Dikkopf-1 plays a specific role in breast, lymphoma, ovarian, lung, esophageal, colon, and pancreatic cancers.5–8,10,16 At the same time, DKK-1 is a key mediator of the tumor growth and angiogenesis, 13 thereby promoting invasion and metastasis.
Dikkopf-1 is a 35-kd protein that contains a signal peptide sequence and 2 cysteine-rich domains. 22 This secreted protein functions as a negative regulator of Wnt signaling and plays an important role in head formation in vertebrate development.22–25 Dikkopf-1 is an endogenous secreted inhibitory factor in the Wnt signaling pathway that binds the Wnt coreceptor low-density-lipoprotein-receptor-related-co-receptor 5/6. 25 Furthermore, DKK-1 was reported to be a downstream target of β-catenin/T-cell factor and to participate in a negative feedback loop in Wnt signaling in colon cancer cells.9,10
DKK-1, DKK-2, DKK-3, and DKK-4, together with a special DKK-3-related protein termed Soggy (Sgy), compose a family of DKK-related genes. Dikkopf-1, DKK-2, DKK-3, and DKK-4 contain 2 discrete cysteine-rich domains, in which the positions of 10 cysteine residues are supremely conserved among family members. Dikkopf-1 and DKK-4, but not DKK-2, DKK-3 or Sgy, have been shown to suppress the Wnt-induced secondary axis induction in Xenopus embryos.8,26 Dikkopf-4 was found to show high specificity for gastric cancer. 27 Other studies have shown that DKK-1 is expressed in Wilms tumor, hepatoblastoma, and hepatocellular carcinoma.28,29 Dikkopf-1 protein, Wnt inhibitory factor-1, and Frizzled-related protein are known to be secreted molecules that have been indicated to bind to Wnt proteins and inhibit their activity.30,31 These 2 proteins were associated with human cancers, including colorectal carcinoma. 32 Dikkopf-1 appears likely to have a possible role in the development or progression of crucial types of human tumor, 33 although it was indicated as a negative feedback factor for the activated Wnt signaling pathway in colon cancer.33,34
In our study, we showed that expression of DKK-1 was enhanced in rectal cancer serum and tissues. Although the detailed function of DKK-1 in rectal carcinogenesis is unknown, our results showed that DKK-1 expression could facilitate the dissemination of tumors by stimulating cell invasion.
The spread of malignant tumors from a primary tumor to form metastasis at distant sites is the most life-threatening complication of cancer and is why rectal cancer can be treated with high success rates; there is a correlation between tumor progression upon diagnosis and probable survival rate.
In conclusion, we have shown that DKK-1 is a possible biomarker for the diagnosis of rectal cancer. Dikkopf-1 was expressed in most of the rectal cancer tissues we examined, and its serum levels of DKK-1 were evaluated in the patients. Dikkopf-1 could promote sensitivity of cancer diagnosis, but it may also contribute to the development of cancer cells.