1 Platelet Granzyme B Induces Contact-Dependent End-Organ Apoptosis during Murine Sepsis
Matthew Sharron1,2, Andrew A. Wiles1, Claire E. Hoptay2, Kanneboyina Nagaraju1,2, Robert J. Freishtat1,21Children's National Medical Center, Washington, DC, United States. 2George Washington University School of Medicine, Washington, DC, United States.
Purpose of Study: The objective of this study is to define the site(s) of and mechanism(s) by which platelet GzmB induces end-organ apoptosis in sepsis, and evaluate the effect of GzmB knockout on sepsis progression, mortality and MODS.
Methods Used: End-organ apoptosis in a murine cecal ligation and puncture (CLP) model of sepsis was analyzed by immunohistochemistry. Platelet cytotoxicity was measured by flow cytometry following 90-minute ex vivo co-incubation experiments with healthy murine splenocytes. Progression of sepsis was measured by a validated preclinical murine sepsis score.
Summary of Results: There was evident apoptosis in spleen, lung, and kidney sections from septic wild type mice. In contrast, there was a lack of TUNEL staining in lungs and spleens from septic GzmB null mice [Apoptotic index per mm2 (Wild Type (WT) vs. GzmB null) for lung = 3776+/-139 vs. 678+/-181 (p<0.001) and for spleen =2,682+/-191 vs. 622+/-120 (p<0.001)] despite similar levels of endotoxin and platelet aggregation. GzmB null mice had lower sepsis scores at all time points post-CLP than WT mice. At 24 hours post-CLP, the mortality rate of the GzmB null mice was 0% while the mortality rate of the WT mice 100%. Kaplan-Meier survival analysis showed that GzmB null mice survived longer following CLP than WT mice (P=0.0019 by Cox Proportional Hazard Regression). In cell culture co-incubation experiments, physical separation of septic platelets from healthy splenocytes by a semi-permeable membrane reduced splenocyte apoptosis to a rate indistinguishable from negative controls. Chemical separation by the platelet GPIIb/IIIa receptor inhibitor eptifibatide decreased apoptosis by 66.6+/-10.6% (p=0.008).
Conclusions: In sepsis, platelet granzyme B-mediated apoptosis occurs in lung and spleen, and absence of granzyme B slows sepsis progression. This process proceeds in a contact-dependent manner that is inhibited ex vivo by platelet GPIIb/IIIa receptor inhibition. If confirmed in vivo, the GPIIb/IIIa inhibitors and other classes of anti-platelet drugs may be protective against MODS in sepsis.
2 Low Spinal Bone Mineral Density in Men with Isolated Gnrh Deficiency is Related to the Degree of Pubertal Activation of Hypothalamo-Pituitary-Gonadal Axis
Edward Horton1, Rohanna Wright2, Flavia Costa Barbosa1, Lacey Plummer1, Jennifer Kaina1, Cassandra Buck1, Ning Jiang1, Richard Quinton2, William F. Crowley Jr1, Ravikumar Balasubramanian11Reproductive Endocrine Unit, Massachusetts General Hospital, Boston, MA, United States. 2Department of Endocrinology, Royal Victoria Infirmary, Newcastle upon Tyne, United Kingdom.
Purpose of Study: Men with isolated gonadotropin-releasing hormone (GnRH) deficiency (IGD) present with hypogonadism and exhibit secondary osteoporosis. Although long term hormonal replacement normalizes serum testosterone levels in these subjects, restoration of adult bone mineral density (BMD) is incomplete and the reasons for this observation remain unclear. As males with IGD display variable degrees of pubertal development and harbor mutations in several genes, we hypothesized that (i) degree of pubertal maturation at presentation will determine adult BMD upon hormone replacement (ii) adult BMD will be variably affected by mutations in specific genes.
Methods Used: Cross-sectional study of men with IGD (n=102; age 18-65 years) on optimal hormonal treatment. BMD was determined using dual-energy x-ray absorptiometry (DXA). Pubertal maturation was graded as: absent puberty, partial puberty, and normal puberty [adult-onset IGD]. Mutational analysis of KAL1/FGF8/FGFR1/PROK2/PROKR2/ GNRH1/GNRHR/KISS1R genes was performed.
Summary of Results: Adult spinal BMD was the most affected in IGD men (62% with T-Score < -1). Duration of hormonal treatment did not correlate with adult BMD but testicular volume at presentation was positively correlated to adult spinal BMD (r=0.4; p=0.049). Although mean T-Scores at the spine and hip did not differ between the absent and partial pubertal groups, overt spinal osteoporosis was more common in subjects with absent puberty than partial pubertal subjects (20 vs. 0%, P=0.0155). IGD subjects with pulsatile LH secretion were more likely to normalize their spinal BMD than apulsatile subjects (55% vs. 22%, p=0.016). In 37 IGD men with positive gene mutations, we found no correlation between specific genetic mutations and adult BMD.
Conclusions: (1) Restoration of spinal BMD is incomplete in IGD men even after prolonged hormonal therapy. (2) Degree of pubertal maturation at diagnosis and neuroendocrine activity at baseline are strong determinants of adult spinal BMD (3) Genetic etiology of IGD is not a critical determinant of adult BMD in these men.
3 Diastolic Function and Survival in Patients with Severe Aortic Stenosis and Normal Left Ventricular Ejection Fraction
Omar K. Khalique1, Robert N. Belkin1, Yat Wa Li1, Wilbert S. Aronow2, Chul Ahn3, Cesare Russo1, Mala Sharma21Cardiology, Columbia University Medical Center, New York, NY, United States. 2Cardiology, New York Medical College, Valhalla, NY, United States. 3 Clinical Sciences, University of Texas Southwestern, Dallas, TX, United States.
Methods Used: We identified 74 patients with echocardiographic aortic valve area < 1 cm2 and LVEF ? 50% in whom echocardiograms were available from which to perform measurements of echocardiographic parameters.
Summary of Results: There were 52 and 22 survivors and non-survivors, respectively. Survivors were more likely to have undergone aortic valve replacement (p = 0.016). Non-survivors had higher left atrial volume index (p = 0.020), E/E'septal (p = 0.044), and peak transmitral inflow velocity (p = 0.021). E/E'average > 15 was significantly associated with the occurrence of death by receiver operating characteristic analysis (p = 0.03). In the group of patients as a whole, E/E'average was a significant independent risk factor for time to death by Cox regression analysis (p = 0.0009). In those patients who did not receive aortic valve replacement (n = 45), E/E'lateral was a significant independent risk factor for time to death (p = 0.0283). There were no significant differences in any Doppler or tissue Doppler parameter of diastolic function, or in left atrial volume index, when comparing patients with high vs. low gradients or when comparing patients with high vs. low flow.
Conclusions: Among patients with severe AS and normal left ventricular ejection fraction, non-survivors had higher LA volume index, mitral E velocity, and E/E'septal. E/E'average was significantly associated with the occurrence of death and was an independent predictor of time to death. E/E'lateral was an independent predictor of time to death in patients who did not receive aortic valve replacement.
4 Prognostic Value of Cardiac Troponin I in Hospitalized Patients with Pneumonia
Nivas Balasubramaniyam1, Wilbert S. Aronow2, Hoang M. Lai2, Chandrasekar Palaniswamy2, Aileen Lorenzo1, Sahil Khera1, Arun Patil21Internal Medicine, Westchester Medical Center/ New York Medical College, Valhalla, NY, United States. 2Cardiology, Westchester Medical Center/New York Medical College, Valhalla, NY, United States.
Purpose of Study: The prevalence of increased cardiac troponin I and its association with in-hospital mortality in hospitalized patients with pneumonia needed investigation.
Methods Used: We investigated the prevalence of an increased cardiac troponin I level and its association with in-hospital mortality in 220 patients hospitalized for pneumonia who had no other causes for an increased cardiac troponin I level. A cardiac troponin I level >0.4 ng/ml was considered increased.
Summary of Results: Of the 220 patients, 35 (16%) had an increased cardiac troponin I level. Patients with increased cardiac troponin I levels had a lower prevalence of smoking (14% versus 35%, p =0.02), a higher prevalence of hypotension (43% versus 20%, p <0.01), a higher use of inotropes (40% versus 17%, p <0.01), and a higher in-hospital mortality (46% versus 17%, p <0.001). Stepwise multiple regression for mortality showed that an increased cardiac troponin I level (p =0.02) and use of inotropes (p<0.0001) were significant independent predictors of in-hospital mortality.
Conclusions: An increased cardiac troponin I level and use of inotropes were significant independent predictors of in-hospital mortality in hospitalized patients with pneumonia and no other cause for an increased cardiac troponin I level.
5 FUNCTIONAL GONADOTROPIN-RELEASING HORMONE DEFICIENCY IN MEN
Hilana Lewkowitz-Shpuntoff1,2, Ravikumar Balasubramanian1, Niraj Chavan1, Jennifer Kaina1, Andrew Dwyer3, Stephanie Seminara1, Lacey Plummer1, Francis Hayes1, William F. Crowley Jr.1, Nelly Pitteloud3Massachusetts General Hospital, Boston, MA, United States. 2Albert Einstein College of Medicine, Bronx, NY, United States. 3Centre Hospitalier Universitaire Vaudois, Lausanne, Switzerland.
Purpose of Study: Pulsatile secretion of gonadotropin-releasing hormone (GnRH) is the master regulator of human reproduction. Hypothalamic amenorrhea (HA) represents a well-characterized GnRH deficient state in women that is secondary to changes in body weight and/or energy intake and is typically reversible following lifestyle correction. A counterpart to HA in male patients subjected to weight loss or excessive exercise is yet to be defined.
Methods Used: Retrospective study of 12 adult men (17-36 yrs) with normal puberty who presented with severe hypogonadism in the presence of either: excessive exercise (>10 hrs/wk) and/or weight loss (>10% of body wt). Thirty-five healthy adult subjects served as controls. All hypogonadal subjects discontinued hormonal treatment and underwent biochemical assessment of their hypogonadism. In 10 men, 12h overnight frequent sampling for leutinizing hormone [LH] secretion was performed. Whenever possible, subjects were re-evaluated weight gain and/or reduction of exercise.
Summary of Results: At diagnosis, mean testosterone levels (161 ± 17 vs. 534 ± 130 ng/dL; p < 0.05), body weight (66.6 ± 2.1 vs. 79.9 ± 14 kg; p< 0.05), and BMI (19.9 ± 0.8 vs. 24.9 ± 3.5 kg/m2; p < 0.05) were significantly lower in the hypogonadal men compared to the healthy controls. Of the 10 men with baseline neuroendocrine assessment, 6 subjects displayed normal adult pattern of LH secretion with inappropriately normal gonadotropin levels given the hypogonadal testosterone levels. Three subjects displayed nocturnal entrained LH pulses characteristic of mid puberty while 1 subject showed apulsatile LH secretion. Seven subjects were reevaluated for recovery following lifestyle intervention and 4/7 showed recovery of testosterone levels while 3/7 remained hypogonadal. Interestingly, in all three subjects with persistent hypogonadism lifestyle correction remained suboptimal.
Conclusions: In men, reversible hypothalamic GnRH deficiency can occur in the setting of weight loss or reduced energy intake and represents a distinct clinical entity analogous to HA in women.
6 Antiphospholipid Antibody Elevation is Associated with “Silent Strokes” in Patients with Patent Foramen Ovale
Ferdinando Buonanno, Ran Meng, Kathleen Feeney, Jing Cao, Eng H. Lo, Mikaela Elia, Molly Thayer, MingMing Ning11Neurology, Mass Gen Hosp/Harvard Med School, Boston, MA, United States.
Purpose of Study: Patent foramen ovale (PFO) related strokes patients have been reported to have higher frequency of hypercoagulable state, but its relationship with isolated antiphospholipid antibody elevation is not clear. We hypothesize that paradoxical embolic events may trigger subclinical infarcts in the setting of this prothrombotic state and lead to subclinical vascular brain lesions. We examined antiphospholipid antibody titer that does not fit the criterion for antiphospholipid syndrome, and its association with white matter lesions (WMLs) in PFO related stroke patients.
Methods Used: Consecutive prospectively recruited PFO-related stroke patients underwent FLAIR sequence MRI and anticardiolipin antibody IgG and IgM measurement (n=69). Subclinical (or clinically “silent”) white matter lesions (WMLs) were inspected by investigators blind to clinical information using two scales (Fazekas and Scheltens) to insure inter-rater reliability and accuracy.
Summary of Results: Patients with elevated anticardiolipin titer had similar clinical characteristics compared to those with normal titers. Overall, total WML burden is statistically significantly increased in PFO stroke patients with positive anticardiolipin antibody compared to those with negative titers. This difference remains statistically significant after adjusting for major confounders associated with WML such as diabetes, hypertension, and smoking status.
Conclusions: Antiphospholipid antibody positivity may contribute to global burden of subclinical disease in patients with PFO related stroke, independent of conventional risk factors for WML. Since PFO is highly prevalent, in one out of four normal individuals, better strategies to identify and stratify stroke risks are direly needed. The combination of blood hypercoagulability testing and the presence of MRI subclinical embolic events can potentially be used to follow disease progression and triage more aggressive stroke prevention strategy in this cohort of patients. Further study with a larger disease cohort and other hypercoagulable states are needed to explore these preliminary findings.
7 Inhibition of Platelet Gpiib/Iiia Decreases Platelet Aggregation but Has No Effect on Granule Release
Claire E. Hoptay1, Andrew A. Wiles1, Matthew Sharron1, Kanneboyina Nagaraju1, Robert J. Freishtat11Children's National Medical Center, Washington DC, DC, United States.
Purpose of Study: Platelets both aggregate and release granules as part of activation. This is enhanced when the GPIIb/IIIa receptor is bound to a ligand. The adhesive function of GPIIb/IIIa allows for aggregation while the outside-in signaling function propagates signals to the inside of the platelet to release granules. GPIIb/IIIa inhibitors are a class of drugs used clinically to inhibit platelet aggregation in prothrombotic states. We hypothesize that in addition to reducing aggregation, platelet granule release is decreased by inhibition of the GPIIb/IIIa receptor.
Methods Used: Citrated human blood was exposed to compounds that selectively reduce platelet aggregation or outside-in signaling. Eptifibatide was used to specifically inhibit GPIIb/IIIa. Platelets were subsequently activated. Antibodies to CD62p, CD63, and LAMP1 were used as markers for ?, dense, and lysosomal granule release, respectively, by flow cytometry. Synthetic beads were used to comparatively measure the size of platelet aggregates.
Summary of Results: Exposure to eptifibatide led to a decrease in platelet aggregation by 70%, with no change in surface expression of CD62p, CD63, or LAMP1. Samples exposed to poloxamer 188, a surfactant known to reduce cell aggregation, showed a 36% reduction in aggregation but no detectable difference in surface expression of the antibodies. Latrunculin A and concanamycin A (CMA) are known to decrease granule release. Latrunculin A-exposed samples showed a 52% reduction in CD62p surface expression and a 27% reduction in CD63 surface expression. CMA-exposed samples showed complete abrogation of CD62p surface expression and an 85% reduction in CD63 surface expression. There was no detectable change in aggregation following exposure to either compound.
Conclusions: Our preliminary experiments show that eptifibatide has similar effects on activated platelets as poloxamer 188; aggregation is reduced with no change in granule release. Both latrunculin A and CMA reduce the release of ? and dense granules with no effect on aggregation. These data suggest that eptifibatide selectively reduces platelet aggregation but has no effect on granule release. Delineation of the effects of different GPIIb/IIIa inhibitors on platelet activation and granule release has important laboratory and clinical ramifications.
8 the Effects of Simvastatin on Human Airway Epithelial Cell Viability and Morphology
Amir A. Zeki1, Saeid Ghavami2, Andrew Halayko2, Reen Wu11Pulmonary, Critical Care, & Sleep Medicine, University of California, Davis School of Medicine, Sacramento, CA, United States. 2Section of Respiratory Medicine, University of Manitoba, Winnipeg, MB, Canada.
Purpose of Study: To determine if simvastatin causes airway epithelial cytotoxicity and if this is dependent on mevalonate (MA); i.e. MA is the immediate product of HMG-CoA reductase (HMGR), the enzyme inhibited by statins.
Methods Used: The normal human bronchial epithelial cell line (HBE1), and primary normal human bronchial epithelial (NHBE) cells were used (in vitro), grown to 90% confluence, then treated with simvastatin (Sim) ± MA (2 mM) in standard serum-starved cell culture conditions. After treatment with low- (2.5, 5, 10 ?M) vs. high-dose Sim (20 ?M) for 24, 48, 72, &/or 96 hrs, we assessed for (1) cell viability using the Alamar blue & MTT assays, (2) cell death using Trypan blue exclusion & total live cell counts, & (3) cell morphological changes using light microscopy.
Summary of Results: Low-dose Sim treatment of HBE1 cells (24 & 48 hrs) did not decrease cell viability, whereas high-dose Sim treatment decreased cell viability in a MA-dependent manner without causing cell death or reduced total cell counts. High-dose Sim treatment (24 and 48 hrs), altered cell morphology (decreased cell size, development of multiple cellular projections, & reduced cell-cell contact), in a MA-dependent manner. In primary NHBE cells there was a time- & dose-dependent decrease in cell viability. After 24 hrs of Sim treatment there was no significant decline in cell viability at any statin dose. However, after 48, 72, & 96 hrs treatment, there was a dose-dependent decrease in cell viability at all statin doses (the greatest decrease at 20 ?M). Both low- & high-dose Sim treatment (40 or 96 hrs) altered cell morphology (changes in cell size and shape/volume, the development of multiple cellular projections, reduced cell-cell contact, & cellular elongation).
Conclusions: Simvastatin may be cytotoxic to human airway epithelial cells at the micromolar doses used. Although there was no detectible cell death at the time points observed, Sim reduced cell viability and altered cell morphology. Some of these statin effects were MA-dependent, indicating that HMGR inhibition mediated some of these effects. Future studies are needed to determine the optimal therapeutic statin dose that preserves cell viability and barrier integrity.
9 Unable to be Published
10 Pediatric Forearm Fractures: Factors Associated with Orthopedic Follow-Up after Discharge from the Emergency Department
Nazreen Jamal1, Sabah Iqbal1, Leticia M. Ryan11Children's National Medical Center, Washington, DC, United States.
Purpose of Study: Children with public insurance are less likely than children with private insurance to obtain follow-up care after Emergency Department (ED) care. The objective of this study is to determine if demographic and clinical factors are associated with aftercare compliance in a population of publicly insured pediatric ED patients with orthopedic injuries. Such information may enable targeted strategies to facilitate compliance in high risk groups.
Methods Used: Retrospective chart review of Washington, DC children ages 0-17 years with public insurance discharged with isolated forearm fracture from the Children's National Medical Center ED from 2003-2006. Bivariable analyses and multivariable logistic regression were performed to measure the association between sociodemographic variables and failure to follow-up.
Summary of Results: 600 children with public insurance met inclusion criteria. The overall cohort was 63.7% male, 81.7% African-American, with a mean age of 8.8 (±3.9) years. Overall, 85.7% of patients went to a follow-up orthopedic appointment and 68.2% of patients had timely orthopedic follow-up, defined as ?14 days after discharge from the ED. Treatment with orthopedic reduction [Adj OR 1.886 (95% CI 1.273-;2.795)] was positively associated with timely orthopedic follow-up, while older age [Adj OR 0.927 (0.886-0.971)] was significantly associated with failure to follow-up. In the subset of patients who required orthopedic reduction in the ED, older age was also significantly associated with failure to follow-up [Adj OR 0.814 (0.670–0.990)].
Conclusions: Mild fracture severity is associated with lack of orthopedic follow-up for patients with public insurance. Older age is associated with lack of follow-up, even in the subgroup of patients with severe fractures. This is concerning because older patients have less bone remodeling potential. Targeted interventions to improve orthopedic aftercare compliance should focus on older patients with severe forearm fractures.
11 Elevated Cerebrospinal Fluid Metalloproteinase-9 is Associated with Poor 6-Month Outcome following Subarachnoid Hemorrhage
Sherry H. Chou1,4,2, Steven K. Feske1,4, Suzanne L. Simmons1, Susannah Orzell1, Rose Du3,4, Andrea Marckmann2, Eng H. Lo2,4, MingMing Ning2,4,11Neurology, Brigham and Women's Hospital, Boston, MA, United States. 2Neurology, Massachusetts General Hospital, Boston, MA, United States. 3Neurosurgery, Brigham and Women's Hospital, Boston, MA, United States. 4Harvard Medical School, Boston, MA, United States.
Purpose of Study: There is growing evidence supporting the role of inflammation in early brain injury (EBI) and vasospasm (VSP) following subarachnoid hemorrhage (SAH). Matrix metalloproteinases (MMP) are released by inflammatory cells and can mediate EBI via disruption of the extracellular matrix and mediate VSP by cleaving endothelin-1 into vasoactive fragments. We hypothesize that MMP-9 in human cerebrospinal fluid (CSF) is associated with VSP and SAH outcome.
Methods Used: We enroll consecutive SAH subjects, bank serial CSF samples, and evaluate their 6-month outcome using modified Rankins score (mRS). VSP is defined as >50% vessel caliber reduction on angiography 6-8 days post SAH. Poor outcome is defined as mRS>2. We compared CSF MMP-9 by ELISA on post-SAH days 0-1, 2-3, 4-5, 6-8, and 10-14 in a SAH cohort (N=35) with and without VSP and poor outcome at 6-months. Continuous variables were compared using t-test or Wilcoxan rank sum test depending on data normality. Repeated measurements were analyzed using longitudinal regression.
Summary of Results: The study cohort has a mean age of 53 years, 54% developed VSP, and 21% had poor 6-month outcome. Elevation of CSF MMP-9 throughout post-SAH days 0-14 was associated with poor 6-month outcome (p=0.007). Specifically, CSF MMP-9 elevation on post-SAH day 0-1 was associated with poor 6-month outcome (p=0.02). After adjustment for SAH clinical severity (HH grade), neither CSF MMP-9 levels nor HH grade were independently associated with 6-month outcome. CSF MMP-9 did not show strong association with VSP.
Conclusions: Early elevation of CSF MMP-9 is associated with poor 6-month outcome but not with VSP in SAH. CSF MMP-9 may mediate EBI in SAH via mechanisms independent of VSP. Incorporation of CSF MMP-9 removes the predictive effect of HH grade on SAH outcome, suggesting that CSF MMP-9 may be in the mechanistic pathway that mediates the effect of high HH score on SAH outcome. Further studies are necessary to determine the source of CSF MMP-9, the mechanism by which it mediates SAH outcome, and to validate CSF MMP-9 as a predictive biomarker for SAH outcome.
12 Bone Mineral Density and Vitamin D Status in African American Children with Forearm Fractures
Leticia M. Ryan1, Stephen Teach1, Cinzia Brandoli1, Steven Singer1, Rachel Wood1, Robert J. Freishtat1, Joseph Wright1, Laura Tosi1, James Chamberlain11Children's National Medical Center, Washington, DC, United States.
Purpose of Study: Pediatric forearm fractures are increasing in incidence and result in substantial costs. Among adults and healthy Caucasian children, bone health deficiencies contribute to forearm fracture risk. Although African American (AA) children may be at higher risk for bone health deficits, the relationship between forearm fracture risk and bone health, including bone mineral density (BMD) and vitamin D status, has not been investigated in this population. Our objective is to determine if AA children with forearm fractures have decreased BMD and an increased prevalence of vitamin D insufficiency (serum 25-hydroxy vitamin D level < 20 ng/mL) compared to fracture-free controls.
Methods Used: This case-control study included cases (AA children, ages 5-9 years, with forearm fracture) and AA fracture-free controls. Evaluation included measurement of BMD, serum 25-hydroxy vitamin D level, body mass index and diet, including calcium intake. Bivariable and multivariable analyses were used to test the association of bone health indices with fracture status, while controlling for confounding variables.
Summary of Results: The final study sample included 78 cases and 74 controls. Cases had significantly lower total body z-scores for BMD [adj OR 0.6 (95% CI: 0.4-0.9)] and were significantly more likely to be vitamin D insufficient [adj OR 3.1 (1.1-8.7)] in comparison to controls. Cases were also significantly more likely to have a body mass index ? 85th percentile [adj OR 4.1 (1.4-12.2)] than controls. There were no significant differences between cases and controls in mean age, proportion who were male, parental education level, season of enrollment, sun exposure, mean dietary calcium nutrient density or mean dietary vitamin D intake.
Conclusions: These data support an association between risk for forearm fracture in AA children and lower BMD and vitamin D insufficiency. These results also provide additional rationale for addressing obesity although further study is needed to determine the mechanism(s) by which obesity increases forearm fracture risk. Because suboptimal bone health in childhood also negatively impacts adult bone health, early identification and evaluation of at-risk children with forearm fractures may allow early intervention with both important short and long term benefits.
13 Early Disease Characteristics of Enthesitis-Related Arthritis Reveals Elevated Transforming Growth Factor-Beta
Hemalatha Srinivasalu1,2, Michael G. Barnes3, Gerlinde Layh-Schmitt1, Michael M. Ward1, Robert A. Colbert11NIAMS, NIH, Bethesda, MD, United States. 2Pediatric Rheumatology, Nemours/Alfred I duPont Hospital for Children, Wilmington, DE, United States. 3Cincinnati BioBank, Cincinnati Children's Hospital, Cincinnati, OH, United States.
Purpose of Study: Examine an inception cohort of enthesitis-related arthritis and analyze serum cytokines to better understand the disease pathogenesis.
Methods Used: Thirty-seven patients satisfying ILAR criteria for ERA were included for study. Relevant clinical, laboratory and radiological data were collected at baseline visit. Serum cytokine assay by ELISA were performed from healthy controls and at the baseline visit from patients. Mann-Whitney U tests, one-way ANOVA, and Tukey's multiple comparison tests were performed for statistical analyses.
Summary of Results: Seventy eight percent were males with median age of 12 years and median disease duration of 5.4 months. HLA-B27 positivity was 59%. The median active joint count and enthesitis count were 1 and 4 respectively. Only one patient had radiographic sacroiliitis. More than 90% of patients were on NSAIDs and 33% had GI complaints at their baseline visit. Our cohort did not differ from other retrospective cohorts with respect to disease characteristics such as enthesitis and joint count, HLA-B27 status. Sacroiliitis was lower and percentage of patients with enthesitis was higher in our cohort. TGF-beta1 was elevated in ERA patients compared to controls. Further, levels of TGF-beta1 were significantly elevated in patients with a history of GI complaints when compared to healthy controls and to patients without GI complaints. Levels of TGF-beta1 were elevated in patients without arthritis when compared to controls. There was no difference in TGF-beta1 levels on comparing patients by presence of enthesitis, HLA-B27 status and inflammatory markers.
Conclusions: This study informs us on the early disease characteristics of ERA. TGF-beta1 has been reported to be elevated in the serum of patients with ankylosing spondylitis. This is the first study reporting elevated TGFb1 in ERA. This finding supports earlier studies we have published on evidence for a TGF-beta1 peripheral blood gene expression signature in ERA patients. Additionally, TGF-beta is known to be elevated in chronic gut inflammation; its elevation in patients with GI complaints seen in our cohort suggests a role of gut inflammation in early ERA.
14 Developing a Directional Airway Secretome in Asthmatic Epithelium Using An in Vitro Wound Repair Model
Dinesh Pillai1,2, Binu-John Sankoorikal1,2, Kristy J. Brown1,2, Mary C. Rose1,2, Yetrib Hathout1,21Division of Pulmonary and Sleep Medicine, Children's National Medical Center, Washington, DC, United States. 2George Washington University School of Medicine and Health Sciences, Washington, DC, United States.
Purpose of Study: Airway epithelium must have intact directional signaling, including secreted proteins (secretome), for normal lung homeostasis. In inflammatory diseases, an altered response to injury can lead to dysfunctional epithelial repair. Establishing an in vitro airway epithelial secretome model in asthma would be a valuable tool to study these diseases.
Methods Used: Asthmatic and non-asthmatic primary nasal epithelial cell cultures (NECs) were differentiated to a respiratory tract epithelium and then scratch-wounded in serum-free media. Secretions were collected 24 hrs after wounding and processed for label free proteome profiling using SDS-PAGE and high resolution LC-MS/MS analysis. Proteins with a spectral count >5 or >5-fold change during repair were analyzed using Ingenuity Pathways Analysis to generate protein networks.
Summary of Results: 576 proteins were present in conditioned media (467 in normal and 511 in asthmatic unwounded cultures). In baseline cultures 6 apical and 14 basal proteins were unique to the non-asthmatic culture and 16 apical and 18 basal proteins were unique to the asthmatic culture. At baseline, non-asthmatic secreted protein networks involved molecular transport/cell-cell signaling (apical) and cellular movement (basal); asthmatic networks involved disease states/free radical scavenging (apical), tissue development (basal), and inflammatory disease (apical and basal). During repair, non-asthmatic networks consisted of protein synthesis/repair (apical) and cellular growth/proliferation (basal); asthmatic networks consisted of cell signaling/proliferation (apical), tissue development (basal) and inflammatory disease (apical and basal).
Conclusions: Proteomic analysis of apical and basal airway epithelial secretomes can generate protein networks specific to wound repair. We found that repairing normal epithelium is intrinsically characterized by unique apical and basal protein networks suggesting a homeostatic environment while repairing asthmatic epithelial networks suggest an overall inflammatory and hyper-proliferative state. This directional secretome model may lead to candidate biomarkers related to abnormal repair in future lung disease studies.
15 Age at Cancer Diagnosis Depends on Parent of Origin of Brca Mutation
Simi George1, Iuliana Shapira1, Daniel Budman1, Meredith Akerman1, Thomas Bradley1, Cinderella Chavez1, Christi Hayes1, Lora Weiselberg1, Vincent Vinciguerra1, Sabeen Mekan1, Kit Cheng1, Sharona Cohen11Hofstra North Shore LIJ School of Medicine, Lake Success, NY, United States.
Purpose of Study: Genetic diseases may display parent-of-origin effects. In such cases, the risk depends on the specific parental allele. Imprinting effects evident in autosomal dominant hereditary paraganglioma lead to tumors only if inherited from paternal germline. Cancer penetrance in carriers of BRCA mutation may be determined by the parental origin of mutation.
Methods Used: From 2007-2010 we analyzed 1889 consecutive (136 ovarian + 1753 breast) breast or ovarian cancer patients presenting for treatment at our outpatient facility. In 130 patients with BRCA 1 or 2 mutations the parent of origin for the mutation was known. Of the 130 patients 2 had both BRCA1 and BRCA2 mutated paternally inherited and were excluded from this analysis.
Summary of Results: In carriers of BRCA mutations the mean age at diagnosis for ovarian cancer was 51 (range 21-70) and for breast cancer was 43 (range 24-78). Two-sample t-test was used to compare the mean age at diagnosis in patients with BRCA 1 or 2 mutations of paternal or maternal inheritance. Significantly younger age at breast cancer diagnosis was observed in paternal vs. maternal inheritance of BRCA1 mutation (36 vs 46, respectively, p<0.0020) and BRCA2 mutation (42 vs 51 respectively, p<0.0008). There was no significant difference between paternal and maternal age of ovarian cancer diagnosis of BRCA1 (p<0.1415) or BRCA2 mutation (p<0.3470).
Conclusions: The restrospective nature of the study may introduce ascertainment bias. However, the breast and ovarian cancers cases in BRCA1 & 2 carriers with maternal or paternal inheritance mirror the Mendelian autosomal dominant pattern in our unselected consecutive cohort of patients. Maternal and paternal inherited BRCA alleles may not be exchangeable. Women with paternally inherited mutations in BRCA gene mutations develop breast cancer at younger age compared with women who inherit the gene mutations from their mothers. In this small sample, clear differences at age of cancer diagnosis are apparent in paternal inheritance of BRCA gene mutation. If this observation duplicates in larger cohorts, the results will have important implications for recommendation of surgical risk reduction in BRCA mutation carriers.
P1 Prognostic Significance of Frequency and Morphology of Premature Ventricular Complexes during Ambulatory Holter Monitoring
Georges Ephrem1, Michael Levine2, Patricia Friedmann3, Paul Schweitzer21Medicine, Beth Israel Medical Center, New York, NY, United States. 2Cardiology, Beth Israel Medical Center, New York, NY, United States. 3Cardiovascular and Thoracic Surgery, Albert Einstein College of Medicine, New York, NY, United States.
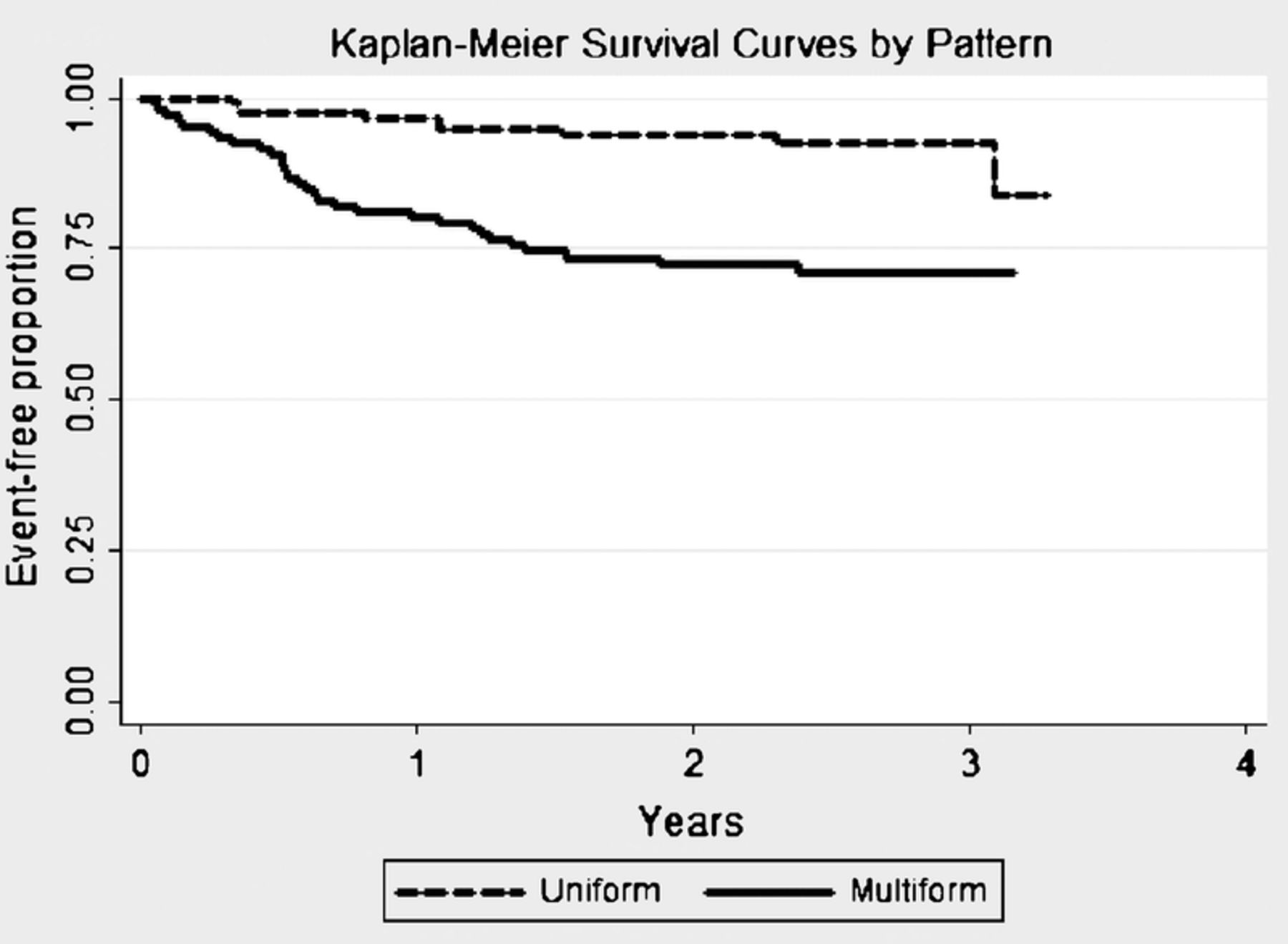
Purpose of Study: Multiform premature ventricular complexes (PVCs) are associated with an adverse prognosis in patients with structural heart disease. Very frequent PVCs are associated with ventricular dysfunction. Our hypothesis is that multiform PVCs confer an adverse prognosis in the general population.
Methods Used: We performed a retrospective cohort study of patients > 18 years-old referred to our institution for 24-hour ambulatory Holter monitoring between July 1, 2008 and December 31, 2009. Holters without PVCs or with more frequent ectopy (couplets, triplets, or non-sustained ventricular tachycardia) were excluded. Clinical and adverse event (AE) data (‘major adverse cardiovascular event’ or new/worsening heart failure) were gathered from chart and database review. Data was analyzed by PVC frequency (rare, occasional, or frequent) and pattern (uniform or multiform).
Summary of Results: 222 patients (43% male, mean age 55 ± 16 years) were evaluated (median follow-up 2.3 years (IQR 2.0-2.6)). Median frequency was 2 PVC/hr (IQR 1-13). Multiform PVCs were noted in 48%. Patients with multiform PVCs were older, and had a higher prevalence of CAD, CHF and previous MI. During follow-up, 39 AE were noted. Patients with an AE were younger, had a higher prevalence of HTN, diabetes, CAD, CHF, and previous MI. The multiform group had a higher incidence of AE (28%) compared to the uniform group (8%) (p<0.001) (Figure 1). Increasing PVC frequency was associated with a higher incidence of AE (8% vs 24% vs 35% respectively). In a Cox regression analysis, the multiform pattern but not frequency predicted AE.
Conclusions: Multiform PVCs were associated with AE.
Log Rank p<0.001
P2 Red Blood Cell Distribution Width as a Predictor of Readmission in Patients with Unstable Angina Or Non St-Elevation Myocardial Infarction
Georges Ephrem11Medicine, Beth Israel Medical Center, New York, NY, United States.
Purpose of Study: Three quarters of rehospitalizations (yearly estimated cost $44 billion) may be avoidable. A screening tool for the detection of potential cases is necessary to make further case management more efficient. The hypothesis is that an elevated red blood cell distribution width (RDW) is an independent predictor of hospital readmission in patients with unstable angina (UA) or non ST-elevation myocardial infarction (NSTEMI).
Methods Used: This was a retrospective observational cohort study of adults admitted in 2007 with UA or NSTEMI and undergoing coronary angiography. Clinical, outcome, and lab data were gathered by review of inpatient charts and databases. Rate of 30-day non-elective readmission and time to non-elective readmission were recorded till November 1, 2011 and compared by RDW group using the 95th percentile (16.3%) as a cutoff.
Summary of Results: Median follow up time of the 503 subjects (average age 65 ± 13 years, 56% male) was 3.8 years (IQR 0.3-4.3). Those readmitted within 30 days were older, had more comorbidities, higher RDW and creatinine levels, and were more likely to have had an intervention. Subjects with any readmission were also likely to be African-American or Hispanics and Medicaid or Medicare beneficiaries. At 3.8 years of follow up subjects with normal RDW (?16.3%) were more likely to be readmission-free compared to those with high RDW (>16.3%) (40.05% versus 27.72%; p = 0.003). In multivariable analyses (Cox proportional hazard and logistic regression respectively) high RDW was a statistically significant predictor of readmission in general (HR 1.41 (1.08-1.83); p = 0.010) but not of 30-day rehospitalization (OR 1.28 (0.69-2.37); p = 0.437). Its sensitivity and specificity at predicting readmission were 23% and 85% respectively with an area under the receiver operating characteristic of 56%.
Conclusions: An elevated RDW was an independent predictor of hospital readmission but not of 30 day-rehospitalization in patients with UA or NSTEMI. While accounting for its sensitivity and specificity RDW may be considered as an inexpensive, readily available, additional tool for detecting patients who may require more elaborate case management with the aim of preventing readmission.
P3 INDUCING MITOTIC DYSSYNCHRONY IN NORMAL AIRWAY EPITHELIUM LEADS TO PRODUCTION OF TGF-β1
Sarah Alcala1,2, Robert J. Freishtat11Children's National Medical Center, Washington, DC, United States. 2The George Washington University, Washington, DC, United States.
Purpose of Study: Immune-mediated inflammation is considered the cause of remodeling in asthmatic airways. However, anti-inflammatory treatment with corticosteroids do not alter remodeling. We have shown that asthmatic airway epithelium is mitotically dyssynchronous and this induces basolateral secretion of TGF-?1, important in fibroblast recruitment and a key component in the airway stress response pathway. Because we consider mitotic synchrony to be a fundamental biological process, we hypothesize that disruption of normal mitotic synchrony will lead to inappropriate secretion of TGF-?1.
Methods Used: Normal primary bronchial epithelium from a single donor was grown in parallel in collagen I coated T-75 culture flasks. At -24 hours, flasks were serum starved for 12 hours in a staggered fashion. At 0 hours, cells from one flask were labeled with membrane dye, PKH-67. The cells were mixed and grown in complete medium and continuously exposed to bromodeoxyuridine (BrdU). An aliquot of PKH-67 and unlabeled cells were reserved and separately plated as synchronous controls. Cells and media were collected at 0, 18, 24, 30, 42 and 48 hours. Mitotic phase was analyzed by flow cytometry for 7-AAD DNA staining in BrdU+ cells. Supernatants were analyzed by ELISA for TGF-?1.
Summary of Results: The mixed culture was mitotically dyssynchronous at 0 and 18 hours. The labeled and unlabeled cells began to spontaneously resynchronize at 24 hours and were fully resynchronized by 48 hours. The 24 and 48 hour controls remained synchronous. Baseline TGF-? was measured at 0 hours. Percentage of baseline was calculated for 18 (-9.4%), 24 (-10.3%), 42 (+2.7%) and 48 (+1.8%) hours in the mixed population. In the control flasks, TGF-?1 percentage of baseline remained low at 24 hours (-10.50%, -8.60%) and 48 hours (-1.81%, -6.45%).
Conclusions: Our data show successful induction of mitotic dyssynchrony in normal cells in which dyssynchrony induces inappropriate secretion of TGF-?1. These data support our previous finding that TGF-?1 secretion is the downstream effect of mitotic dyssynchrony. Additionally, normal cells spontaneously resynchronize. Because asthmatic cells do not spontaneously resynchronize, this suggests the existence of an important cellular regulatory signal in normal airway mitosis that is impaired in asthma.
P4 Relationship between Pediatric Early Warning Score and Emergency Department Disposition
Kristen Breslin1, Julie Marx2, Ryan McBeth3, Padmaja Pavuluri41Division of Emergency Medicine, Children's National Medical Center, Washington, DC, United States. 2Goryeb Children's Hospital, Atlantic Health System, Morristown, NJ, United States. 3Department of Emergency Medicine, University of Rochester Medical Center, Rochester, NY, United States. 4Division of Pediatric Hospital Medicine, Children's National Medical Center, Washington, DC, United States.
Purpose of Study: To determine the association between the Pediatric Early Warning Score [PEWS] at time of Emergency Department [ED] disposition and level of care (discharge, acute care, or intensive care). The PEWS is a 13-point clinical severity score.
Methods Used: This was a prospective study of a convenience sample of patients aged 0-21 years evaluated in the ED of an urban, tertiary care children's hospital between November 2010 and July 2011. Patients were identified via the electronic tracking system at the time of disposition and information to calculate the PEWS was obtained. Demographics, clinical data, and disposition at 12 and 24 hours were obtained from the medical record. Bivariable and multivariable analyses were performed to determine the association of PEWS with level of care. We also sought to identify PEWS that maximized sensitivity and specificity for admission and intensive care.
Summary of Results: The sample of 383 patients included 239 discharged home, 126 admitted to acute care, and 18 admitted to intensive care. Assigned PEWS ranged from 0 to 9. After adjusting for triage level and insurance type, a one-point increase in PEWS increased the odds of admission to any level of care by a factor of 1.54 (95% CI 1.29-1.83) and the odds of acute care admission by a factor of 1.49 (1.25-1.78) relative to discharge. Adjusted for triage level, a one-point increase in PEWS increased the odds of intensive care admission by a factor of 2.09 (1.61-2.71) relative to discharge and by a factor of 1.40 (1.12-1.75) relative to acute care. Area under the receiver operator characteristic [ROC] curve was 0.68 (0.62-0.74). PEWS ?3 demonstrated 31% sensitivity and 91% specificity for admission. PEWS ?5 had 28% sensitivity and 96% specificity for intensive care. Among 97 patients with respiratory complaints, the area under the ROC curve was 0.80 (0.71-0.89).
Conclusions: PEWS is a rapid, easy-to-use score that is associated with the level of care at ED disposition. It does not provide adequate discriminant ability to be used in isolation to predict ED disposition.
P5 Proteomic Analysis of Bronchial Casts from Patients with Sickle Cell Disease Or Congenital Heart Disease
Joi Lucas1, Diego Preciado2,3, Kristy J. Brown2,3, Dinesh Pillai1,2,3, Mary C. Rose2,31Division of Pulmonary and Sleep Medicine, Children's National Medical Center, Washington, DC, United States. 2Center for Genetic Medicine Research, Children's National Medical Center, Washington, DC, United States. 3Departments of Integrative Systems Biology, George Washington University, Washington, DC, United States.
Purpose of Study: Plastic Bronchitis is a rare lung condition characterized by the formation of bronchial casts that may occlude the airway leading to respiratory compromise, morbidity, and mortality. Current classification of casts is based upon clinical and histological findings. Type I casts exhibit inflammatory cell phenotypes with fibrin and are associated with bronchial diseases. Type II casts are acellular with mucins and typically associated with congenital heart disease (CHD) patients that undergo palliative surgery. Recent studies have recognized predominately fibrinous casts in sickle cell disease (SCD) patients with acute chest syndrome. Proteomic evaluation of bronchial casts has not been reported and may give a greater biochemical understanding of cast formation associated with specific diseases.
Methods Used: Bronchial casts were collected by bronchoscopy or spontaneous expectoration from patients with SCD (n=3), CHD (n=2), and control patients without SCD or CHD (previously healthy children with current respiratory infection; n=2). After solubilizing casts, proteins were processed for label-free proteome profiling using a combination of polyacrylamide gel electrophoresis, tryptic digestion, and high resolution LC-MS/MS analysis.
Summary of Results: Several proteins were common to all three cohorts; fibrinogen peptides were abundant. Peptides specific to MUC5AC and MUC5B identified these major lung mucins in bronchial casts. Additional samples are being analyzed by histology, proteomics and Western blot analysis. Data for each of the three cohorts will be presented.
Conclusions: The abundance of fibrinogen in all bronchial casts indicates that fibrinogen is critical in the formation of casts. Isolating proteins unique to casts of certain disease types may ultimately facilitate preventative treatment measures for plastic bronchitis.
P6 Analysis and Outcomes of Abnormal Ecgs in a Cohort of Patients Seen at An Urban Academic Pediatric Emergency Department
Shilpa Patel1, Elizabeth Anne Greene2, Mohsen Saidinejad11Emergency Medicine, Children's National Medical Center, Washington, DC, United States. 2Cardiology, Children's National Medical Center, Washington, DC, United States.
Purpose of Study: To describe the follow-up outcomes for patients whose emergency department(ED) ECG is read as abnormal.
Methods Used: Cross sectional analysis of all pediatric patients with an abnormal ECG, between January 8, 2010 and January 8, 2011, from the emergency department (ED) of an urban academic pediatric hospital. Abnormal ECGs were identified from cardiology communication logs to the ED. Abnormal was defined as any ECG for which cardiology recommended follow-up. Data were abstracted by chart review. Exclusion criteria included age greater than 18 years, prior known cardiac disease, or grossly abnormal ECG. A database of all patients who had an ECG recorded during the study period was created from MUSE, the ECG electronic recording system.
Summary of Results: A total of 1923 patients had an ECG in the ED during the study period. The mean age was 12.0 ± 9.0 (s.d.) years, 52% were female and 62% were black. An abnormal ECG was reported in 577/1923 (30%) patients. Of these, 137/577 (24%) patients were excluded. Analyses were performed on the remaining 440 patients. The three most common indications for an ECG were: chest pain 129(29%), transient loss of consciousness 109 (25%), and possible arrhythmia 59 (13%). The most common abnormalities were: left ventricular hypertrophy 120 (27%), prolonged QTc 89 (20%), and nonspecific ST changes 39(9%). 261/440 (59%) were discharged and 179/440(41%) were admitted. Urgent follow-up (24-48hours) was recommended for 46/440 (10%) and routine follow-up (2-4 weeks) for 394/440(90%). In the urgent group, 31/46 (67%) had documented follow-up, compared to 234/394 (59%) in the routine follow up group. This resulted in 177 cardiology visits, 86 cardiology consults, 270 repeat ECGs, 166 echocardiograms, 39 holter monitors, 23 stress tests, 3 event monitors and 2 tilt tests, with an approximate total of $750,000 in estimated charges based on our institutional billing rates for additional work up.
Conclusions: Approximately one third of our patients had an abnormal ECG requiring follow-up. The decision to perform an ECG as part of the ED evaluation of children has important implications for further follow-up if a minor abnormality is discovered. The cumulative cost of these investigations is significant.
P7 Estrogen Inhibits Tgfβ1-Induced Epithelial-Mesenchymal Transition in Asthmatic Airway Cells
Asha S. Payne1,2,4, Andrew A. Wiles1, Sarah Alcala5, Kanneboyina Nagaraju1,3,4, Robert J. Freishtat1,2,31Center for Genetic Medicine Research, Children's National Medical Center, Washington, DC, United States. 2Emergency Medicine and Trauma Center, Children's National Medical Center, Washington, DC, United States. 3Integrative Systems Biology, George Washington University School of Medicine and Health Sciences, Washington, DC, United States. 4Department of Pediatrics, George Washington University School of Medicine and Health Sciences, Washington, DC, United States. 5Microbiology, Immunology, and Tropical Medicine, George Washington University, Washington, DC, United States.
Purpose of Study: Estrogen may exacerbate the gender disparity in asthma, perhaps through changes to epithelial morphology. Recent literature highlights the structural changes occurring in asthmatic epithelium, including epithelial-mesenchymal transition (EMT). TGF?1 has been reliably shown to induce EMT in human bronchial epithelial cells (HBE) in vitro. We propose that the pro-inflammatory actions of estrogen will promote TGF?1 induced EMT in asthmatic airway epithelium.
Methods Used: Commercially available asthmatic HBE cells (n=2) were grown and fully-differentiated at ALI. After a 24hr equilibration in steroid free media, epithelia were then exposed continuously to 17? estradiol (0.01, 0.1, or 1nM). After 24 additional hrs, epithelia were additionally exposed to TGF?1 (10ng/mL) and TNF-? (10ng/mL). 48 hours later, cells were harvested and RNA assayed for epithelial and mesenchymal marker transcripts via qRT-PCR.
Summary of Results: TGF?1-exposed asthmatic epithelia demonstrated a dose response to estrogen. Increasing the estrogen concentration down-regulated fibronectin mRNA expression (fold change 0.1nM vs non-exposed = 1.024 [95%CI: 1, 1.048] and fold change 1nM vs non-exposed=0.933 [0.925, 0.941]). In addition, the same estrogen concentrations up-regulated e-cadherin expression (fold change 0.1nM vs non- exposed = 0.971 [0.952, 0.990] and fold change 1nM vs. non-exposed = 1.176 [1, 1.352]) and beta-catenin expression (fold change 0.1nM vs non-exposed = 1.089 [1.006-1.172]). Vimentin expression was not altered by any concentration of estrogen exposure.
Conclusions: Contrary to our hypothesis, estrogen did not enhance TGF?1 induced EMT in asthmatic epithelium. Rather, estrogen showed a dose-dependent preservation of the epithelial phenotype. Additional investigations are needed to define the mechanisms by which estrogen may inhibit EMT in airway epithelial cells.
P8 Achieving Quality Improvement in Patient Care on Labor and Delivery
Diana P. Broomfield1, Edom Yared1, Nuru Robi1, Tiffany Wilson1, Long Duc Nguyen11OB/GYN, Howard University Hospital, Washington, DC, United States.
Purpose of Study: Triage is defined as sorting patients and setting priorities for their treatment in urgent care settings, emergency rooms, clinics, hospitals and health maintenance organizations. A pregnant woman who comes to the Labor & Delivery area should be evaluated in a timely fashion.” ACOG recommends the evaluation of a patient on labor and delivery should be made within 30 minutes. In the 2008-2009 academic year, a small scale performance review at Howard University Hospital by the residents noted a marked delay in the triage times in excess of 120 minutes on Labor & Delivery.
Methods Used: 16 residents were divided into 4 CQI teams. Data was collected by reviewing the charts of patients who presented to Labor & Delivery during each of the four 3 month periods assigned to each team. After reviewing the data from each of the groups, interventions to improve the triage times were implemented. Some of those interventions included: For scheduled procedures, prepare the H & P, labs in the office Evaluation of patients on arrival by nurse and physician together Utilize triage & LDR rooms appropriately Improve early notification, MD is notified as soon as patient arrives on the unit.
Summary of Results: Over the course of the year, we were able to improve the triage time from an average of 124 minutes during the first quarter of the year to 30.17 minutes by the beginning of the 2010-2011 academic year. The goal of a 30 minute triage time is one that is attainable as long as all parties involved are committed to the goal. The use of continuous quality improvement and the PDSA/ PDCA cycle allows for the assessment of implemented changes, and gives all parties involved an equal opportunity to contribute to the desired outcome.
Conclusions: Significance/Implications/Relevance: The goal of a 30 minute triage time is one that is attainable as long as all parties involved are committed to the goal. This standard is in accordance with improved patient safety. The use of continuous quality improvement and the PDSA/ PDCA cycle allows for the assessment of implemented changes, and gives all parties involved an equal opportunity to contribute to the desired outcome.
P9 Reproductive Options for Hiv Positive Patients in the United States
Lisa J. Green1, Tiffany Hailstorks1, Diana P. Broomfield11Obstetrics and Gynecology, Howard University Hospital, Washington, MD, United States.
Purpose of Study: The CDC estimates 1.2 million people in the United States (US) are currently living with HIV infection and the largest group affected (86%) are within reproductive age (15-44 years old). A study by Chen et all showed that 28% percent of HIV positive adults desire to have biologic children. There are a few options, provided by fertility centers, that are available to HIV positive or HIV discordant couples who wish to conceive. IVF-ICSI and IVF-IUI may not completely eliminate all the risks involved, but they are a safer option than sexual intercourse. Our current study aims to determine the number of fertility centers across the nation who has standardized protocols and offer such services to HIV positive and discordant couples. We also seek to understand what are the prohibitive factors involved in providing fertility services to this population.
Methods Used: We conducted a cross-sectional study using telephone and fax based survey.
Summary of Results: Only about 25-30% of centers in the U.S. allow or offer discordant couples that are HIV positive (or other infectious diseases such as hepatitis)to undergo in vitro fertilization procedures. Smaller centers are most unlikely to offer in vitro services to HIV positive patients.
Conclusions: HIV-discordant Couples undergoing IVF illicit many of ethical questions. If the mother is treated during labor, vertical transmission of HIV from mother to baby is now very low. Many of the estimated six million people in the US infected with HIV, Hepatitis B (HBV) or Hepatitis C (HCV) are of reproductive age. Those desiring to have children and minimize the possibility of passing their virus to their offspring need access to specialized advanced reproductive technologies, and to deny them only increases the unnecessary risk of exposing children to the virus.
P10 Assessment of Use of Implantable Cardioverter- Defibrillator in African American Patients with Advanced Systolic Heart Failure
Selomie M. Kebede1, Thaslim A. Kassim1, Sirikarn Napan1, Steve Singh2,11Howard University Hospital, Washington, DC, United States. 2Veteran Affair Hospital, Washington, DC, United States.
Purpose of Study: The use of Implantable Cardioverter-Defibrillator (ICD) in patients with advanced systolic heart failure with ejection fraction <= 35% has been shown to improve survival and decrease the incidence of sudden cardiac death. African American (AA) patients have a higher incidence of ischemic and non-ischemic cardiomyopathy. Assessment of use of ICD in AA patients with advanced heart failure is limited. The purpose of this study is to assess the use of ICD in AA patients with advanced systolic heart failure who are on optimal medical therapy.
Methods Used: Two hundred ninety nine AA patients with advanced systolic heart failure with New York Heart Association class II and III who were admitted to Howard University Hospital for decompensated heart failure from January 2006 to January 2011 were included in the study. Data on use of ICD were obtained from the medical records and chart reviews. Data on mortality was obtained from Social Security Death Index.
Summary of Results: Out of the eligible 299 patients, only 118 (39.5%) received ICD. Among males, 58% received ICD therapy compared with only 42% among the females. The median Left ventricular ejection fraction was 24%. The cause of heart failure was ischemic cardiomyopathy in 61.5% and non ischemic in 38.5%. There were a total of 27 (23.3%) deaths in patients who received ICD versus 60(33.9%) in those who did not receive ICD. (P= 0.052).
Conclusions: The rate of use of ICD therapy in eligible African American patients was 39.5% in the observed population with a lower rate of ICD use in AA women compared to AA men. Further research should explore factors contributing to low ICD utilizations in this population group.
P11 Knowledge of Appropriate Sizing and Defibrillator Pad Position Placement among Emergency Medical Care Providers for Children
Kiesha Fraser1, Maybelle Kou1, John Howell1, Kaidi Fullerton1, Charles Sturek11Pediatric Emergency Deparmtment, Inova Health Systems, Falls Church, VA, United States.
Purpose of Study: Upwards of 14,000 pediatric out-of-hospital arrests occur annually. With such significant numbers and variation in training backgrounds of medical providers, dissemination of information about the importance of correct weight-based defibrillator pad selection for children and proper anatomic positioning of defibrillator pads by medical caretakers would theoretically ensure optimal survival by the patient.
Methods Used: This prospective comparison education intervention study sought to determine the knowledge of the proper sizing of defibrillator pads, the ideal anatomic placement and the retention of this knowledge amongst medical care providers for pediatric patients. This study protocol entailed recruiting, emergency medical care providers for children from 6 medical fields, Emergency Medicine Attending (EM), Emergency Medicine Residents (EMR), Pediatric Residents (PR), Pediatric ER Nurse (PERN), Adult ER Nurses (AERN) and pre-hospital personnel (EMS)) for a total of 152 participants. All subjects were given two simulated clinical scenarios of different weighted subjects in ventricular tachycardia, then put through a series of questions to ascertain their knowledge of resuscitation and finally an intervention with correct placement and choice related education.
Summary of Results: Assessments were made of choice and placement of pads for each participant. For the 10kg mannequin PR accurately chose the right size pads 100% (Confidence Interval (CI): 88-100%), EMR chose correctly 96% (CI: 80-100), PERN 100% correctly (CI: 73-100), EM 96% (CI: 79-100), EMS 97% (CI: 82-100%), AERN 100% (CI: 83-100%). For the 20kg mannequin PR chose accurately 49% of the clinical scenarios (CI: 33-64) EMR 37% (CI: 22-56), PERN 92% (CI: 65-100), EM 32% (CI: 17-52), EMS 27% (CI: 14-45), AERN 18% (CI: 7-39). The overall correct placement by weight in the 10kg mannequin was 9.2% (CI: 5.5-15) and in the 20kg mannequin 25.7% (CI: 19.4-33.2).
Conclusions: Pediatric care providers identified the correct size pads for both mannequin scenarios, but were not as knowledgeable as their adult contemporaries in pad placement. Education regarding choice and placement of pediatric defibrillator pads should be provided to all health care providers involved in the medical care of children.
P12 Utility of Flexypnea Induction in the Echocardiographic Assessment of Heart Failure
Ofer Sagiv1, Michael Vitellas1, Gila Perk1, Izhak Kronzon11Cardiology, Lenox Hill Hospital, New York, NY, United States.
Purpose of Study: “Flexypnea’ refers to positional dyspnea associated with bending forward. Given the dependence of standard echocardiographic parameters on loading conditions, assessment of echocardiographic indices with the “flexypnea” maneuver may provide insight into the mechanism of flexypnea.
Methods Used: 19 subjects with heart failure and 19 control subjects were enrolled in the study. The major exclusion criteria were severe left sided valvular disease and atrial fibrillation. In addition to a baseline echocardiogram, additional echocardiographic acquisitions were obtained from an apical window while the patient was sitting down and leaning forward. An apical 4-chamber and 2-chamber views were obtained, and attention was focused on obtaining mitral inflow parameters including mitral E velocity, E/A ratio, and E/E’ ratio. These parameters were used to estimate left atrial pressure. Measurements of blood pressure, oxygen saturation and heart rate were also performed.
Summary of Results: Baseline characteristics were similar based on age, race, heart rate, blood pressure and BSA. The heart failure group had significantly lower EF (35% vs. 63%, p<0.0005), more males (84% vs. 42%, p<0.007), diabetics (42% vs.10%, p <0.027) and hypertensives (90% vs. 42%, p<0.002). Flexypnea occurred in 25% of heart failure patients vs. 0% in the control group (p=.016). Primary outcome analysis showed that E/A ratio change was -21.2% vs. +8.3% in controls and subjects, respectively (p=.047). E/E’ ratio change (which estimates LA pressure) was +15% in controls vs 1.2% in the heart failure group (P=NS). When comparing patients with flexypnea vs asymptomatic patients, no difference was found with regard to E/A % change or E/E’ % change. Among all patient in the study, E/E’ ratio increased by an average of 10% while performing the maneuver.
Conclusions: Although the flexypnea maneuver is thought to cause patients to be short of breath from increased LA pressure, the most reliable echocardiographic index of LA pressure (E/E’ ratio) did not correlate with patients symptoms in this study but did increase with the maneuver among all patients. The flexypnea maneuver predictively changes diastolic parameters (i.e E/A ratio) and may be used to distinguish patients with normal vs. pseudonormal diastolic profile as the latter patients will increase their E/A ratios.
P13 Relationship among Fibromyalgia and Rhinitis
Marianne Frieri1, Antigone Argyriou21Medicine, Nassau Univ. Medical Ctr., East Meadow, NY, United States. 2Physical Medicine & Rehabilitation, Montefiore Medical Center, Bronx, NY, United States.
Purpose of Study: Fibromyalgia (FM), a common chronic pain disorder characterized by diffuse musculoskeletal pain has several unrelated symptoms, a broad variety of complaints and lack of tests to accurately identify the disease. FM has significant overlap with several other systemic diseases including those of sensory hypersensitivity, autonomic deregulation, rhinitis and neurological dysfunction. A relationship among chronic rhinitis and the pathogenesis related to aberrant pain processing, immunoregulatory abnormalities may occur in autoimmune disorders with increases in immunological signalling molecules such as cytokines, NGF, TNFa, L-selectin.
Methods Used: A case report and review of the literature. A 45 year old woman was diagnosed with FM at age 25 with compliants of fatique, myalgias, migraine, sinusitis, and asthma. An ANA had a speckled pattern but rheumatologic evaluation was negative for SLE, Physical examination revealed non-tender sinuses, boggy nasal turbinates, clear lungs. Skin tests were consistent with non-allergic rhinitis. Family history was significant for Hashimoto thyroiditis, migraine and asthma.
Summary of Results: The pathophysiology is an inflammatory response, cytokine activation through viral neurotropism and glial activation as a possible mechanism. By better understanding the pathophysiology of FM, physicians may be able to more accurately diagnose and treat debilitated and often stigmatized patients, the complexity of the disease by a multidisciplinary approach of this multifaceted syndrome. Baraniuk has discussed an overlap with systemic hyperalgesia, autonomic dysfunction, irritable bowel syndrome, migraine headaches, sensory hypersensitivity, dyspnea, congestion, rhinorrhea (Baraniuk JN, Allergy Asthma Proc 31:169 -178, 2010.) Neurological dysfunction may account for the overlap of CFS with idiopathic nonallergic rhinopathy and sinusitis.
Conclusions: The overlap between fibromyalgia and several other diseases of immunological dysfunction and rhinitis suggest a link between the immune system and the body's pain response. The inflammatory molecules used as chemical signals throughout the nervous system have provided much insight into altered levels of pain sensation.
P14 Unusual Presentation of Facial Angioedema
Marianne Frieri1, Reenal Patel11Medicine, Nassau Univ. Medical Ctr., East Meadow, NY, United States.
Purpose of Study: To describe angioedema, a type I IgE-mediated allergic reaction which can also include allergic contact dermatitis, a delayed type of induced sensitivity from cutaneous contact with numerous agents. Identification and avoidance of contact is the key to success and patch testing is the gold standard. Latex allergy is a type I reaction and can also be a component of rubber, which can induce a type IV contact dermatitis. It is still an occupational exposure, has an atopic tendency which is higher in patients sensitized to other allergens and those with additional findings of eczema.
Methods Used: We describe a 44 year old African American female, with history of chronic rhinitis, sinusitis, asthma, eczema, dyslipidemia, and hypertension, with complaints of resolved face and neck swelling, seen 2 days prior by her dentist for placement of a Valplast denture with no use of analgesics or noted complications. Two days after placement she noted swelling of her face and neck. There was no difficulty in breathing, tongue, throat swelling, or erythema. After removal of her dentures, there was mild reduction in her face and neck swelling. She reported an allergy to latex which had caused her itching, erythema, and hand swelling. Environmental history was significant as a home health aide. Medications were not new and she was never hospitalized for asthma or an allergic reaction. On physical examination her vitals were normal with positive findings of mild frontal sinus tenderness, bilateral nasal mucosla congestion. Lung examination was clear with no wheezing or stridor. Skin examination had no angioedema, rash or dermatitis. Pulmonary lung function testing was normal.
Summary of Results: sIgE was positive only to cockroach, but negative to latex. A patch test for type IV reactions for 29 allergens, showed negative reactions to all rubber products, but showed a slight reaction to p-tert-butylphenol formaldehyde resin.
Conclusions: Latex allergy was considered but results by sIgE and patch testing for rubber compounds were negative. Valplast, is a nylon thermoplastic with a base resin and the adhesive material could have contained cyanoacrylate. The limited patch test did not contain acrylates. The patient did not return but could be sent for the Finn chamber patch to another site for acrylics and anti-IgE for-formaldehyde and acrylics.
P15 Erdheim-Chester Disease (Ecd): Natural History
Juvianee I. Estrada-Veras1, William A. Gahl1, Bernadette Gochuico11National Human Genome Research Institutes, National Institutes of Health, Bethesda, MD, United States.
Purpose of Study: ECD is a rare non-Langerhans cell histiocytosis of unknown etiology. It has been reported mainly in adult males over 40 years of age. No causative gene has been identified; family studies have not been performed due to the sporadic nature of the disease. The clinical characteristics of ECD range from asymptomatic to multisystemic. ECD affects the bones, kidneys, retroperitoneal space, skin and brain. After diagnosis, the disease progresses rapidly without treatment, causing fatal outcomes due to severe lung disease, chronic renal failure and cardiomyopathy. The diagnosis of ECD relies upon imaging studies and pathologic findings in biopsies of affected organs, i.e., fibrosis and infiltration of the affected tissues with foamy histiocytes, lymphocytes, and plasma cells. Immunohistochemistry reveals cells positive for CD68 and negative for CD1a and S-100. There is no standard treatment for ECD, although alpha-interferon, steroids and monoclonal antibodies have been proposed. A systemic proinflammatory cytokine signature has been described which has encouraged the use of interferon. Symptomatic improvement has been reported with these therapies, but death remains the expected outcome.
Methods Used: The longitudinal progression and natural history of ECD has not been well documented. Its etiology and pathogenesis are poorly understood. We will evaluate patients with ECD at the NIH Clinical Center under NHGRI study 11-HG-0207 “Clinical and Basic Investigations into Erdheim-Chester disease” (clinicaltrials.gov id: NCT01417520). Participants will be admitted to the NIH Clinical Center for 1 week. During this period, cells, plasma, urine, DNA and RNA will be obtained and other basic studies will be performed in order to understand the pathogenesis. Clinical manifestations will be studied to define the clinical spectrum.
Summary of Results: Participant evaluations are in progress.
Conclusions: ECD is a rare orphan disease that is still poorly understood. In the last years there has been an increase in the number of new cases, but research studies are still needed for better characterization of this disease. Through our study we intend to further describe this disorder and provide a foundation for genetic and metabolic studies that can help identify the basic defects in ECD. This new understanding could lead to more effective treatments.
P16 Successful Therapy of Cold Agglutinin Disease Utilizing Rituximab
Michelle Cholankeril1, Thomas Bradley1, Craig Devoe1, Cristina Ghiuzeli1, Jonathan Kolitz1, Steven Allen11Hematology and Oncology, North Shore University Hospital, Lake Success, NY, United States.
Purpose of Study: Cold agglutinin disease is an autoimmune hemolytic anemia mediated by cold reactive autoantibodies triggering complement mediated hemolysis. This condition, when not associated with infection, is characterized by clonal proliferation of CD20+ B cells that produce monoclonal IgM cold agglutinins. Conventional therapies for primary cold agglutinin disease (CAD) are ineffective. Case reports suggest that rituximab, an anti-CD20 monoclonal antibody, may be effective.
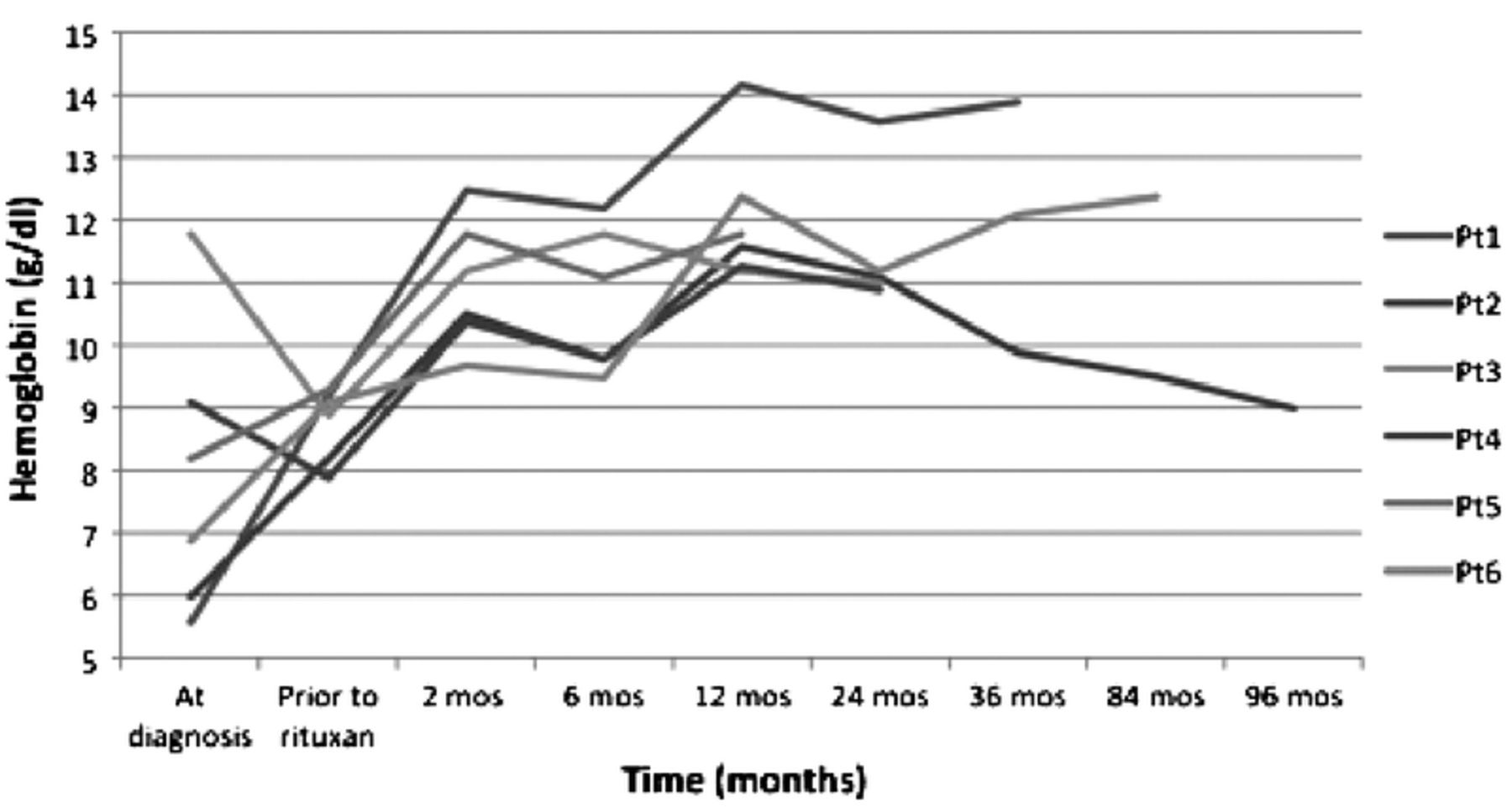
Methods Used: We evaluated the use of rituximab therapy in 6 patients (pts) [1M, 5F; median age 70 years (range 62 - 89)] in a retrospective single institution study. 3 pts had primary CAD, 2 pts had mixed CAD and warm AIHA, and 2 pts had CAD in the setting of CLL. 5 pts had received steroid therapy, 2 pts IVIG, 1 pt azathioprine, and 5 pts PRBC transfusion (2-10 units). 5 received induction therapy with rituximab 375 mg/m2 IV weekly × 4 weeks and 1 for 7 weeks. 4 pts received maintenance rituximab 375 mg/m2 IV every 2 months (4+ to 12 cycles).
Summary of Results: All responded to therapy with a median rise in hgb of 1.8 g/dl at 2 months from initiation of induction with further improvement over time (Image 1). Re-induction was performed in 2 pts; both had an initial 1 year duration of response and both responded following re-treatment. Median duration of response is 3+ yrs (range 1-8+ yrs); the 8+ yr response was in pt 2 who received only induction therapy. 2 pts have completed 2 years of maintenance therapy and remain in remission at 4 months and 2 years post, respectively. Cold agglutinin titers decreased by 4 fold in 2 patients, 1 fold in 1 pt and remained stable in 1. Despite the improvement in hgb in all pts, laboratory evidence of low grade hemolysis persisted in 4 pts. All pts were able to be tapered off steroids and all remain transfusion free.
Conclusions: Rituximab appears to be a well tolerated and effective therapy for CAD. The utility of maintenance rituximab requires further evaluation.
Hgb response to rituximab
P17 Unable to be Published
P18 the Influence of Race on Mortality and Morbidity following Cardiac Surgery
Joshua Langert1,2, Gregory Trachiotis1,2, Michael Greenberg2, Richard Amdur1,21The George Washington University, Washington, DC, United States. 2VA Medical Center, Washington, DC, United States.
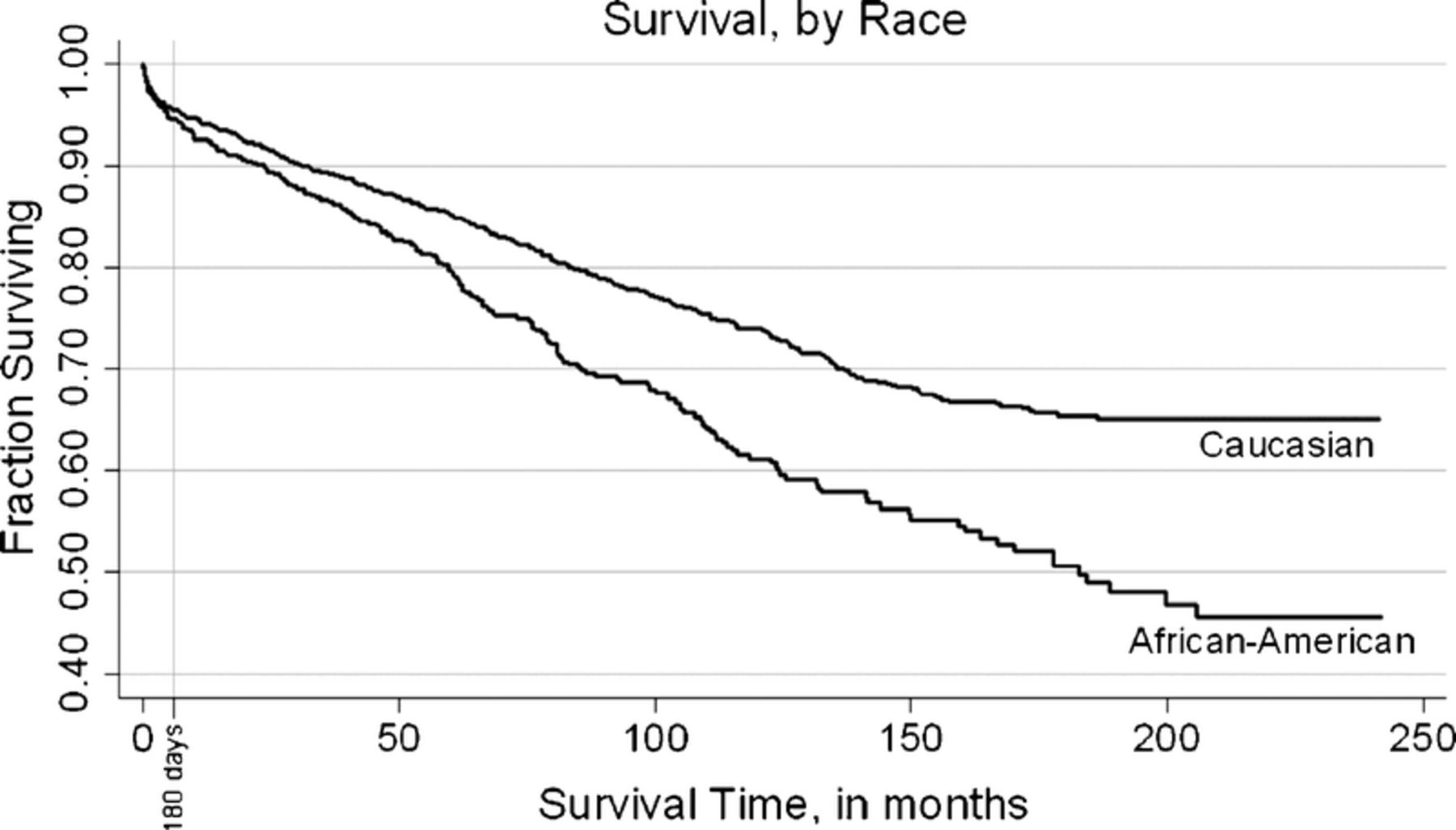
Purpose of Study: Current models of morbidity and mortality following cardiac surgery do not take into account patient race. We aim to determine if race is an independent predictor of mortality and postoperative complications after undergoing cardiac surgical procedures.
Methods Used: Data from the Continuous Improvement in Cardiac Surgery Program (CICSP) Database were obtained. These data were prospectively collected on all patients undergoing cardiac surgical procedures at the Washington, DC VA Hospital from November 1990 to February 2009. These data were statistically analyzed to determine if race is a predictor of mortality or postoperative complications, independent of preexisting risk factors.
Summary of Results: Of 2205 patients, 1599 were classified as Caucasian, 569 classified as African-American, and 37 were other (Native American, Hispanic, or other groups). There was no significant difference in 180-day mortality between groups (?2=0.45, p=0.50). However, deaths during the entire study period, show a significantly increased risk in the African-American group (?2=18.85, p=0.00001). The Cox proportional hazards model gives a significant hazard ratio=1.44 (95% CI: 1.08-1.91). Of the preoperative risk factors evaluated, only PVD (?2=78.04, p<0.00001) and diabetes (?2=16.52, p=0.00005) were significant. This is corroborated by the Cox analysis, which showed a hazard ratio=1.47 (95% CI: 1.24-1.74) and 1.42 (95% CI: 1.20-1.69), respectively. None of the postoperative morbidities showed significant ?2 values for either the Caucasian or African-American groups.
Conclusions: Immediately following cardiac surgery, race is not a significant influence on mortality or postoperative complications. However, over time, there is a significant risk to survival for the African-American group. The presence of peripheral vascular disease and diabetes are additional risk factors, and careful consideration of these should be given when planning cardiac surgery for these patients.
P19 HIV IN THE NATION'S CAPITAL: PREVALENCE OF ANTIRETROVIRAL RESISTANCE IN TREATMENT-NAÏVE PATIENTS, 2007-2010
Matthew J. Swierzbinski1, Virginia Kan3, David M. Parenti21Internal Medicine, The George Washington University Medical Center, Washington, DC, United States. 2Infectious Diseases, The George Washington University Medical Center, Washington, DC, United States. 3Infectious Diseases, Veterans Affairs Medical Center, Washington, DC, United States.
Purpose of Study: HIV treatment has been greatly impacted by transmitted antiretroviral (ARV) resistance, and baseline resistance testing before ARV initiation has been recommended since 2007. Several studies have documented resistance in naïve individuals and estimates of transmitted drug resistance mutations range from <5% and as high as 24%. Washington, D.C. has the highest HIV prevalence (3.2%) in the United States, but data regarding the frequency of major mutations and ARV resistance is limited.
Methods Used: A retrospective review of the medical records at 2 facilities in Washington, D.C, The George Washington University Medical Center (GWUMC) and the Veterans Affairs Medical Center (VAMC), were queried for ARV-naïve adults with HIV genotype testing during 2007-2010. Data collection included age, sex, race/ethnicity, CD4, HIV RNA, mutations based on the 2010 IAS-USA list, and interpreted ARV resistance.
Summary of Results: Of the 407 ARV-naïve patients, 277 were in care at GWUMC and 130 at VAMC. The characteristics of our patient population and results are revealed in the table below. In patients found to have resistance, the majority had resistance in a single ARV class, but dual class resistance was seen in 5 patients (1.2%) and triple class in 1 patient (0.2%). There was a gradual increase in NNRTI resistance between 2008-2010.
Conclusions: The prevalence of transmitted RT and Pr mutations (17.4%) and ARV resistance (8.6%) at our study sites was high but similar to rates reported by other areas of the United States. Given the HIV prevalence of 3.2% in the District of Columbia, this has important implications for treatment of these ARV-naïve patients.
P20 towards a Ctsa-Wide Exchange of Experiences and Applets: The Ru-Berd Evaluation Tools Suite
Aparna Junuthula1, Knut M. Wittkowski11Biostatistics, Epidemiology & Research Design, The Rockefeller University, New York, NY, United States.
Purpose of Study: Successful grant writing, optimal resource allocation, and efficient fulfillment of CTSA reporting requirements all require data about current and past CTSA activities to be easily available in a variety of formats: Current use of laboratory or computational facilities, publications by category of CTSA affiliates (clinical scholars, faculty, affiliated centers,) and time period (12 months, 5 years,), yet the technology to bring this information to the fingertips of CTSA investigators and administrators is mostly ill-suited and/or expensive.
Methods Used: Inspired by the often time-consuming experience during the recent renewal process, the RU CCTS has begun an effort to develop tools for gathering and displaying data for CTSA-specific needs. These tools are being developed using an open-source Business Intelligence Reporting Tool, which is designed to facilitate the exchange of applets with users at other institutions. The architecture combines Web services that are already being used across CTSA institutions for C&T science with open source tools (BIRT) designed to facilitate sharing of reporting and evaluation components.
Summary of Results: The DashBoard interacts with other BERD tools, such as WISDOM and µStat to turn extracting CTSA-specific tables, lists, and metrics from data gathered at different CTSA resources from a conundrum into a streamlined process.
Conclusions: At the 2010 ACTS meeting, ACTS members initiated a collaboration, which let to a position paper, published Feb 11, 2011, in Statistics in Medicine, on the contribution of BERD practitioners to the evaluation process. Novel BERD approaches, such as µStat, advance both C&T research and the development of evaluation metrics. The interactive system presented here, combines existing and novel BERD tools (μStat and WISDOM on the one and the DashBoard on the other hand) to turn the published principles into practical tools for supporting the evaluation process.
P21 from Snps to Epistatic Regions: Translating Gwas into a Tool for Personalized Medicine
Knut M. Wittkowski1, Martina Durner2, Martin P. Seybold3, Vikas Sonakya1, Hiroshi Mitsui41Biostatistics, Epidemiology & Research Design, The Rockefeller University, New York, NY, United States. 2Department of Psychiartry, Mount Sinai School of Medicine, New York, NY, United States. 3Institute for Visualization and Interactive Systems, Stuttgart University, Stuttgart, Germany. 4Investigative Dermatology, The Rockefeller University, New York, NY, United States.
Purpose of Study: Genome Wide Association Studies have had limited success when applied to complex disease. Analyzing SNPs individually requires several large studies to integrate the often contradictory results. In the presence of epistasis, multivariate approaches based on the linear model often have low sensitivity and generate artifacts. Novel statistical approaches are needed to turn GWAS into a powerful tool for translational science.
Methods Used: The recent advances in distributed and parallel processing spurred methodological advances in non-parametric statistics. U-statistics for multivariate data are not confounding the results by relying on unrealistic assumptions. Applied to GWAS, this computational biostatistics approach can detect epistasis by integrating data from neighboring SNPs with HapMap information to identify sections of disease pathways and pinpoint functionally relevant intragenic regions. The tools are made available to CTSA trainees and investigators as a Web service at http://mustat.rockefeller.edu.
Summary of Results: Here, we present recent results from studies combining new and publicly available data. In one study, only 185 children and publicly available controls sufficed to confirm, integrate, and extend previous findings and generate biologically plausible hypotheses about the interplay of the genetic risk factors involved in a complex disease. In another study, the same computational biostatistics tools let to novel strategies for the treatment of cancer.
Conclusions: For comparative effectiveness research and personalized diagnostics to live up to their full potential, cases and controls need to be closely matched to the population involved or the patient seeking a diagnosis. Many complex diseases are influenced by both genes and environment, and adequately controlling for these influences when selecting appropriate cases and controls is essential to tease out predictive factors. This goal is much easier to achieve if only a few hundred cases and controls, rather than several thousands need to be matched to the patient.
P22 Postoperative Seizure Outcomes When Interictal Magnetoencephalography Concordant with Ictal Depth Electroencephalography
Kristen Upchurch1, J. Stern2, N. Salamon3, S. Dewar2, D. Eliashiv4,21University of New Mexico, Albuquerque, NM, United States. 2Neurology, UCLA, Los Angeles, CA, United States. 3Radiology, UCLA, Los Angeles, CA, United States. 4Neurology, Cedars-Sinai, Los Angeles, CA, United States.
Purpose of Study: Interictal magnetoencephalography (iiMEG) is often done to localize the likely epileptogenic zone in patients (pts) w/medically intractable epilepsy (mie) undergoing evaluation for surgical treatment. We compared iiMEG results w/intracerebral depth EEG ictal onsets (idEEG) in the context of postoperative seizure (sz) control.
Methods Used: 45 mie cases w/implantation of intracerebral depth electrodes at 1 center between 5/00 & 10/05 were retrospectively reviewed; 30/45 had iiMEG. We evaluated the concordance of iiMEG epileptiform dipoles w/idEEG, classified as intralobar (group A), lobar (B), lateralized (C), bilateral homotopic (D1), bilat homotopic iiMEG with unilat depth (D2), non-concordant unilat MEG & bilat depth (D3), non-concordant multifocal MEG & depth (D4), contralat non-concordant (E). The lack of depth lateralization or localization was classified as (F), the lack of MEG dipoles as (G).
Summary of Results: 22/30 presurgical pts w/both iiMEG & idEEG studies subsequently had resection (rsx); 20 resected pts had postop sz outcome follow-up w/durations ranging 10-96 months (mean 50). Sz outcomes corresponded to our MEG-depth EEG concordance classification as follows. The concordant groups (A, B, C, D1, D2) comprised 22/30 pts; 17 had rsx, w/postop sz outcomes of: Engel class I (11 pts) & class IV (6). The non-concordant groups (D3, D4, E) comprised 2/30 pts; 1 had rsx, w/Engel class IV outcome. The groups in which 1 of the 2 tests yielded no information (F, G) comprised 6/30 pts; 2 had rsx, w/sz control outcomes of Engel class I for the 1 resected pt w/no iiMEG dipoles & Engel class II for the 1 resected pt w/no lateralizing or localizing idEEG findings.
Conclusions: Clinical use of MEG is becoming increasingly routine & is supported by clinical research results & professional guidelines; yet standardized use has not developed. In our results, the majority of the presurgical pts had some degree of concordance of iiMEG epileptiform dipoles & idEEG. Our results suggest that the significance of concordance of iiMEG w/idEEG in presurgical evaluation for resective epilepsy surgery is complex & requires further analysis. A larger case series may be needed to address this question.
P23 Screening for Hepatocellular Carcinoma in Veteran Population has Negligible Impact on Mortality When Cirrhosis Diagnosis and Liver Transplantation Rates are Low
Alyson McGhan3, David E. Kaplan2,11GI, University of Pennsylvania, Philadelphia, PA, United States. 2Philadelphia VAMC, Philadelphia, PA, United States. 3University of Pennsylvania SOM, Philadelphia, PA, United States.
Purpose of Study: Screening for hepatocellular carcinoma (HCC) is recommended for high-risk cirrhotic patients but little evidence of efficacy in improving overall survival exists. We hypothesized that screening for HCC among cirrhotic US veterans would be associated with improved detection of early stage HCC and improved overall survival relative to unscreened.
Methods Used: Demographics, pre-HCC cirrhosis diagnosis, Child-Pugh score, initial BCLC tumor staging, treatments, survival, and type of pre-HCC screening were extracted from the electronic medical records of veterans diagnosed with and treated for HCC at the Philadelphia VAMC from 2008-2010 under an IRB-approved protocol. Screening was defined as within or outside of AASLD guidelines: imaging with or without AFP every 6-12 months for two years prior to diagnosis. Cox logistic regression and Kaplan-Meier methods were used to evaluate the significance of screening class on survival. Sensitivity analyses were done to determine the transplantation rates for BCLC A patients required for screening to impact survival.
Summary of Results: 93 male veteran patients with HCC were identified with initial BCLC stage distribution of 0(n=3), A(n=42), B(n=21), C(n=24), and D(n=3). Median follow-up was 346 days. 61 (66%) carried a diagnosis of cirrhosis of whom 18 (30%) were screened by AASLD guidelines, 29 (47%) had haphazard screening, and 14 (23%) had no screening. Median survival for patients with and without AASLD screening was not significantly different in univariate (496 vs 516 d, ?2=0.51 p=0.48) or multivariate analysis controlling for age, CTP, and MELD score. 4 (9.5%) BCLC A patients were transplanted. Adding 7 simulated AASLD-screened transplanted BCLC A patients (transplant rate of 22.4%) was required to give screening a survival advantage (?2=4.27 p=0.039).
Conclusions: In this study, screening patients with known cirrhosis for HCC was not associated with a survival benefit largely due to low transplantation rates. A large number of patients with HCC were excluded from screening due to non-diagnosis of cirrhosis. Future studies of HCC screening efficacy must account for both population-specific cirrhosis diagnosis and liver transplantation rates.
P24 Renal Cyst Growth in the Post-Nephrectomy Population
Ron Golan1, Christina Pasick1, Woojin Kim1, Parvati Ramchandani11Radiology, University of Pennsylvania Medical Center, Philadelphia, PA, United States.
Purpose of Study: Benign renal cysts are a frequent incidental finding on cross-sectional imaging studies in middle aged and older adults. The etiology for cyst development remains unclear. The literature indicates that benign renal cysts can grow approximately 1.6 mm/year (1). Although malignant transformation of cysts is uncommon, an unexpectedly large increase in cyst size raises the worrisome possibility of malignant change in the cyst wall and necessitates imaging directed at determining whether such change has occurred. We undertook this study to determine if loss of renal mass, as after radical nephrectomy, influences the rate of growth of cysts on the remaining kidney, as there was an anecdotal belief in our institution that simple cysts in the remaining kidney grow at more accelerated rates than in patients with intact kidneys.
Methods Used: Our study population was derived from a search of a radiology reports within our radiology information system after institutional IRB approval was obtained. Computed tomography (CT) scans and magnetic resonance imaging (MRI) images of 47 patients who had undergone radical nephrectomy for malignancy, had renal cysts, and had serial imaging were reviewed to determine the rate of cyst growth in the remaining contralateral kidney. The mean number of serial images per patient was three, with a mean follow-up period of 18 months.
Summary of Results: The mean yearly rate of change for all simple renal cysts in the contralateral kidney of our post-nephrectomy patient population was an average of 2.57 mm/year compared to the 1.6 mm/year in patients with bilaterally functioning kidneys. Cysts larger than 2 cm in diameter grew at a slightly faster rate than cysts less than 2 cm (2.94 vs. 2.18 mm/year, respectively).
Conclusions: Our findings suggest that surgical nephrectomy affects growth in size of simple renal cysts in the contralateral kidney to some extent. Further diagnostic testing to characterize the cyst, such as contrast enhanced scans, should be reserved for patients with very rapid increase in cyst size, to exclude malignancy or other pathologies. Reference: N. Terada, Y. Arai, et al. The 10-year natural history of simple renal cysts. Urology, 71 (2008), pp. 7-11.
P25 Etiology of Syncope in Patients Hospitalized with Syncope and Predictors of Mortality and Readmission for Syncope at 17- Month Follow-Up: A Prospective Study
Sahil Khera1, Sachin Sule1, Wilbert S. Aronow1, Chandrasekar Palaniswamy1, Chul Ahn2, Sreedhar Adapa1, Stephen J. Peterson1, Nivas Balasubramaniyam1, Christopher Nabors11Internal Medicine - Cardiology, New York Medical College, Valhalla, NY, United States. 2Clinical Sciences, University of Texas Southwestern Medical Center, Dallas, TX, United States.
Purpose of Study: To investigate etiologies and risk factors for mortality and rehospitalization in patients admitted for syncope.
Methods Used: We designed this prospective study to investigate the etiologies of syncope and risk factors for mortality and rehospitalization in 242 patients (mean age: 68±17, men 53% and women 47%) at 17-month follow-up.
Summary of Results: The etiologies of syncope included the following: vasovagal syncope in 49 patients (20%), volume depletion in 39 patients (16%), orthostatic hypotension in 13 patients (5%), primary cardiac arrhythmias in 25 patients (10.3%), structural cardiac disease in 6 patients (2%), and drug overdose in 5 patients (2%). The etiology of syncope could not be determined in 84 patients (35%). Of the 242 patients, 6 (2%) were rehospitalized for syncope, and 12 (5%) died. Stepwise logistic regression analysis showed a significant independent prognostic factor for rehospitalization for syncope was drug overdose (odds ratio [OR]: 11.506; 95% CI: 1.083 - 22.261). Stepwise logistic regression analysis showed significant independent prognostic factors for time to mortality were undetermined etiology of syncope (OR: 4.665; 95% CI: 1.002 - 21.727), San Francisco Syncope Score (OR: 3.537; 95% CI: 1.472 - 8.496), hypertension (OR: 0.099, 95% CI: 0.019 - 0.504), and glomerular filtration rate (OR: 0.964; 95% CI: 0.937 - 0.993).
Conclusions: In our study, SFSR was independently associated with mortality on multivariate logistic regression analysis. Drug overdose was significantly associated with rehospitalization for syncope. The offending drugs in the study included narcotics, benzodiazepines, and non-benzodiazepine hypnotics (zolpidem). In our study, higher GFR was a significant independent negative predictor of time to mortality.
P26 the Greater Metropolitan Medical Alumni Council (Gmmac): The Realization of a Need
Elise Belilos1, James M. Oleske2, Norman B. Medow3, Richard Sadovsky4, Christopher L. Campese5, Jacqueline A. Bello3, Kenneth G. Swan21Winthrop University Hospital, Mineola, NY, United States. 2UMDNJ/New Jersey Medical School, Newark, NJ, United States. 3Montefiore Medical Center/AECOM, Bronx, NY, United States. 4SUNY Downstate Medical Center, Brooklyn, NY, United States. 5North Shore University Hospital, Manhasset, NY, United States.
Purpose of Study: The greater New York metropolitan area includes eight medical schools. Their Alumni Association (AA) Presidents formed a council five years ago, meeting three times a year to share ideas and identify best practices to solve mutual problems challenging students and alumni.
Methods Used: A survey of the eight medical AA was conducted; all responded and the results constitute the data reported in this abstract.
Summary of Results: Mean AA membership was 2,509 or 33% of mean alumni populations (7,489). Two AA conferred membership at graduation; hence 100% of alumni were AA members. Omitting these two AA reduced mean participation to 1,722 or 23%. AA support staff averaged 3.8 persons (range 1-7). The two most frequently cited AA challenges were membership & fundraising. All AA had annual or biennial reunions and considered the reunion to be a major commitment of resources. Despite this commitment, mean reunion attendance was only 242 alumni (range 40-500) or 7.3% of alumni in anniversary years (5 year intervals). The average number of alumni who contributed annually to their alma mater through its AA was 1,936 (range, 500-3,500), or 26% (range, 5-47%). Medical AA reported mean assets of $2,755,000 (range, $6,475-$11,000,000). Mean AA budget was $298,750, of which 65% (range 13-100%) was devoted to ‘Medical Student Support’. The most frequently cited student activities were “Career Night”(100%), “White Coat Ceremonies”(63%), medical equipment (stethoscopes, etc., 50%), and alumni host programs (38%). Eleven additional medical student activities received financial support from the eight AA in varying proportions.
Conclusions: Each AA in GMMAC has derived significant benefit from the application of best practices to its individual problem set. In particular, a nascent AA developed significant momentum in its formation and development by its participation in GMMAC. Additionally, these data provide a foundation for the development of best practices within medical school AA for optimizing support of student programs and alumni participation. We urge formation of similar medical AA organizations in other metropolitan areas.
P27 Prostaglandin (Pg)D2 Receptor Ligation Counters Atherogenic Effects of Celecoxib and Restores Cholesterol Efflux Pathways in Thp-1 Human Macrophages
Nicholas Famigletti1, Iryna Voloshyna1, Michael Littlefield1, Steven E. Carsons1, Allison B. Reiss11Department of Medicine, Winthrop University Hospital, Mineola, NY, United States.
Purpose of Study: Celecoxib (Cx), a cyclooxygenase (COX)-2-specific inhibitor, acts by limiting expression of PGs such as PGD2. Cx is an analgesic, anti-inflammatory agent, but has cardiovascular (CV) toxicity. We previously demonstrated that COX-2 inhibition by Cx is pro-atherogenic through suppression of cholesterol efflux [downregulation of cholesterol 27-hydroxylase (27-OHase) and ATP binding cassette transporter 1 (ABCA1)], and enhancement of influx [scavenger receptors (SR)]. Here we determine whether activation of the PGD2 receptor in THP-1 human macrophages can abrogate atherogenic effects of Cx.
Methods Used: Differentiated THP-1 macrophages (phorbol dibutyrate, 100nM, 48h) were incubated 18h in the presence/absence of: Cx (10 μM); Cx (10 μM)/18h PGD2 agonist [DP epitope] BW245C (1 μM); Cx (10 μM)/18h PGD2 agonist [CRTH2 epitope] 13,14dkPGD2 (1 μM). 1μg of total RNA/condition was used for (QRT)-PCR to assess message for 27-OHase and ABCA1, and SR CD36 and LOX1. Foam cell formation (FCF) in lipid-loaded (25 μg/ml oxidized LDL, 48h) macrophages was quantified as percentage oil red O stained cells by light microscopy. Studies were done in triplicate.
Summary of Results: Incubation of THP-1 macrophages with Cx decreased 27-OHase and ABCA1 mRNA (by 30.2±7.1% and 24.6±5.6% of control, respectively [P<0.01]). Cx augmented expression of SR CD36 (167.4±8.78%, P<0.01) and LOX1 (165.15±21.29%, P<0.01). Pro-atherogenic changes induced by Cx elevated FCF by 62.2±5.2% above control. In Cx-treated cells activation of the PGD2 receptor (either epitope) upregulated 27-OHase and ABCA1 to the level of control. SR expression remained elevated despite PGD2 receptor ligation. However, activation of the PGD2 receptor limited FCF to the level of control.
Conclusions: COX-2 inhibitors increase risk of heart attack and stroke. Here we report that pro-atherogenic shift in cholesterol metabolism induced by Cx is partially reversed by activation of the PGD2 receptor. PGD2 agonists restore cholesterol efflux and prevent macrophage FCF. PGD2 receptor agonists could provide a novel approach to improving the CV safety profile of COX-2 inhibitors.