
Abstract
Thyroid cancer is the most common endocrine cancer in the United States. The primary treatment of thyroid cancer is partial or complete thyroidectomy in patients in whom the cancer is discovered preoperatively, and is often followed by radioactive iodine ablation. After the initial therapy, patients are followed up regularly, most commonly by measurement of serum thyroglobulin (Tg) levels and high-resolution neck ultrasound. As Tg is only produced within the thyroid gland, it has long been recognized as an excellent biomarker for the presence of residual disease after treatment. A number of immunoassays are in common use to measure serum Tg levels. Unfortunately, irrespective of which method is chosen, there is a major potential artifact, in that the presence of autoantibodies binding to Tg (ATG) may bias the results to the point where they are clinically unreliable.
This article describes a liquid chromatography-tandem mass spectrometry (LC-MS/MS) method for the measurement of serum Tg after tryptic digestion of serum samples. The method is compared to Tg analyses using both a Food and Drug Administration–approved immunometric assay (IMA) and a well-respected, clinically used radioimmunoassay. In the absence of ATG, the new LC-MS/MS assay demonstrates equivalency compared to the IMA. However, in ATG-positive patients, the IMA Tg results are lower than the LC-MS/MS assay and the radioimmunoassay Tg results are typically higher. These studies demonstrate the accuracy and validity of the measurement of Tg by LC-MS/MS. This assay will permit the accurate determination of Tg levels even in patients with ATG.
Thyroid cancer is the most common endocrine cancer in the United States, with an estimated 56,000 new cases projected in 2012. 1 Although a number of distinct histological types exist, papillary thyroid cancer and follicular thyroid cancer account for more than 90% of differentiated thyroid cancer (DTC). These thyroid cancer types express a variety of differentiated products, including thyroid peroxidase, thyroid-stimulating hormone (TSH) receptor, and thyroglobulin (Tg). The measurements of these elements have been used in the follow-up of patients with DTC.
The primary treatment of thyroid cancer is total or near-total thyroidectomy in patients in whom the DTC is discovered preoperatively. Depending on the extent of involvement, lymph node dissection may be performed as well. Depending on risk stratification, patients receive radioactive iodine to ablate remaining thyroid tissue and to eradicate any residual tumor. Those with continued or recurrent disease are treated with high doses of radioactive iodine.2–4 After thyroid resection, all patients receive thyroid hormone replacement to treat hypothyroidism and to achieve adequate suppression of TSH in high-risk patients.3,5,6
After the initial therapy, patients are followed up every 6 to 12 months, most commonly by measuring serum Tg levels and high-resolution neck ultrasound. Thyroglobulin, a large glycoprotein, is produced only within the thyroid epithelial cells and has been recognized for some time as an excellent biomarker for the presence of residual thyroid tissue after treatment. In initial stages of assessment, Tg levels are typically measured after either withdrawal of thyroid hormone replacement or after stimulation with recombinant TSH. In patients considered to be free of disease at first evaluations, sequential measurements of unstimulated Tg are recommended. 3
Because Tg is such a useful marker for this disease state, many diagnostic assays to measure Tg have been developed. The most common form is the noncompetitive immunometric assay (IMA) which is typically performed on a fully automated autoanalyzer. The advantages to this type of analysis are its speed, ease-of-use, and low cost-per-test. In the 2-stage IMA, the Tg in serum is first captured by an excess of antihuman Tg monoclonal antibody bound to a solid support (most often beads). This binding is followed by a washing step, which removes unbound components. In the final step, the quantity of bound Tg is measured by incubation with a second anti-Tg monoclonal antibody tagged with a chemiluminescent label. As with all autoanalyzers, the ease-of-use can come with some loss of specificity.
The more traditional and specific methodology is the radioimmunoassay (RIA). In this assay, a radiolabeled Tg tracer competes with endogenous Tg in the patient sample for a limited amount of high-affinity, polyclonal rabbit anti-Tg antibody. A second antibody (antirabbit IgG) is then used to precipitate the Tg-antibody complex and the amount of radioactivity precipitated in the complex is inversely proportional to the amount of serum Tg present in the sample. Although the RIA is more specific than most IMAs, it suffers from requiring larger sample volumes, a high operator skill level (because it is manually intensive) leading to higher potential variability, is less sensitive than an IMA, and requires the use of a radioactive tracer.
Whichever of the 2 methods is chosen, both are susceptible to a major potential artifact, in that the presence of autoantibodies that bind to Tg (ATG) can bias the results of the immunoassays to the point where they are clinically unreliable. Because as many as 25% of all thyroid cancer patients are estimated to have measurable autoantibodies, the most generally available, reliable biomarker of recurrence, Tg, is unreliable. In ATG-positive patients (ATG+), Tg results may be either falsely low in the case of the IMAs (due to shielding of the Tg by the autoantibodies) or falsely low OR high in the case of the RIAs (shielding or bridging).
Mass spectrometry has been used in the field of protein analysis and quantitation for many years.7–9 During that time, many different approaches have been used to measure high molecular mass proteins such as Tg. The most common approach has been to enzymatically digest the protein of interest into smaller peptides through the use of digestive enzymes, most commonly trypsin. Trypsin digests proteins in a predictable manner, allowing users to measure proteins outside the measurable mass range of their mass spectrometers through the use of unique surrogate protein-specific peptides. These peptides are chosen to represent the intact protein and if chosen correctly give a direct 1:1 stoichiometry with their parent protein in a totally specific manner. In this way highly specific, sensitive and quantitative assays can be developed and used both in basic research and commercially in diagnostic laboratories.
In the context of the application of protease digestion and mass spectrometry to measure Tg, a major secondary benefit becomes apparent, as the use of trypsin to digest the Tg protein into manageable sized peptides also destroys any ATG that may be present. In this way, after the complete protease digestion of untreated patient serum samples with trypsin, the tryptic peptide of interest can be captured and measured quantitatively with a mass spectrometer. Because of the complete trypsin digestion of the sample, the measurement of Tg levels is independent of the concentration and type of ATG that may be present. The process of preparing the sample for measurement by liquid chromatography-tandem mass spectrometry (LC-MS/MS) thus circumvents the issue of autoantibodies and clinicians will be able to use measurements of Tg from ATG+ thyroid carcinoma patients to the same degree as Tg measurements in patients without ATG (ATG−).
In the present article, we present a study using this approach of tryptic digestion of serum samples followed by LC-MS/MS to measure Tg with comparisons to both a Food and Drug Administration–approved IMA and a well-respected, clinically used RIA. We will show that in the absence of autoantibodies the new LC-MS/MS assay performs identically with 2 IMAs. Furthermore, we demonstrate that in ATG+ samples, the IMA results are lower than the LC-MS/MS assay and that the RIA results are typically higher. We also show that the titer of ATG is not a consistent predictor as to whether a patient sample will be biased in either the IMA or RIA; although in most samples, there is an affect. This is in agreement with similar observations in previously reported literature and confirms that simple measurement of Ab titers cannot be used in place of Tg levels for Ab+ patients.
Materials and Methods
Purified human Tg was obtained from Fitzgerald Industries International (North Acton, MA). Mass spectrometry-grade purified trypsin (Trypsin-Gold) was obtained from Promega Corporation (Madison, WI). All other standard reagents were obtained from Fisher Scientific (Pittsburgh, PA) or Sigma-Aldrich (St. Louis, MO).
Anti-Tg Autoantibody Assay
Anti-Tg was measured on the Siemens IMMULITE 2000 (Siemens Healthcare Diagnostics Inc, Los Angeles, CA) using the Anti-TG Ab assay. This is a solid-phase, enzyme-labeled, chemiluminescent sequential IMA. Limit of quantitation (LOQ) is 20 IU/mL. ATG-positive (ATG+) sera have concentrations of ATG greater than or equal to 20 IU/mL. ATG-negative (ATG−) sera have undetectable concentrations of ATG, less than 20 IU/mL.
Immunometric Tg Assay
The Siemens IMMULITE 2000 Tg Assay (Siemens Healthcare Diagnostics Inc)
This assay is a solid-phase, chemiluminescent IMA and was used as the primary IMA for comparison to the LC-MS/MS assay in this study. The solid phase (bead) is coated with antiligand. The reagent contains ligand-labeled anti-Tg murine monoclonal antibody and alkaline phosphatase (bovine calf intestine) conjugated to sheep polyclonal anti-Tg antibody in buffer. The patient samples and reagents are incubated simultaneously with the bead for 60 minutes. Thyroglobulin from the sample forms an antibody sandwich complex with ligand-labeled anti-Tg and alkaline phosphatase conjugated anti-Tg. The antibody sandwich complex, in turn, binds to antiligand on the solid phase. Unbound conjugate is then removed before chemiluminescent substrate is added to the bead. The signal is generated in directly proportional to the Tg present. The clinical reportable range is 0.2 to 300 ng/mL.
Beckman Coulter (Beckman Coulter, Brea, CA) DxI 800 Tg Assay
The method is a chemiluminescent immunoassay for the quantitative determination of Tg levels in human serum using the Beckman Coulter DxI 800 and was used as a secondary IMA for comparison in ATG− sera. This Tg assay is a simultaneous 1-step immunoenzymatic (“sandwich”) assay. A sample is added to a biotinylated mixture of 4 monoclonal anti-Tg antibodies, streptavidin-coated paramagnetic particles, and alkaline phosphatase conjugated monoclonal anti-Tg antibody. The biotinylated antibodies bind to the solid phase and the serum Tg binds to these bound antibodies as well as the conjugated antibody. Unbound material is removed and chemiluminescent substrate is added. The light generated is directly proportional to the concentration of Tg in the sample. The clinical reportable range is 0.05 to 500,000 ng/mL.
Commercial RIA to Measure Serum Tg Levels
The competitive RIA was performed at the USC Endocrine Laboratory. 10 Thyroglobulin in the patient's serum competes with a trace amount of 125I-lableled human Tg for a limited amount of high affinity polyclonal rabbit anti human Tg antibody. The Tg-antibody complex is precipitated with an antirabbit IgG second antibody and unbound radioactivity washed away. The amount of radioactivity precipitated in the complex is inversely proportional to the Tg concentration in the patient's specimen. The clinical reportable range is 0.5 to 100 ng/mL.
LC-MS/MS Tg Assay
Patient samples underwent a series of steps consisting of reduction, alkylation, and tryptic digestion after which a selected specific Tg peptide was captured from the mixture using proprietary antipeptide antibody (IgY) beads raised against the peptide of interest. The enriched peptide was released from the beads and analyzed on a LC-MS/MS system using multiple-reaction monitoring (MRM) mode for detection.
Internal Standard Peptides and Analytical Peptide
T129 (VIFDANAPVAVR) and its stable isotope–labeled internal standards (T129-IS1 (+12Da), VIFDANAPV*AV*R), and T129-IS2 (VIFDANAPV*AVR) (where V* represents 13C5, 14N-labeled valine) were synthesized by Pi Proteomics (Huntsville, AL). The purity of both isotope-labeled peptides was greater than 98%.
Antipeptide Antibody Beads
The selected Tg peptide T129 (12 amino acid, VIFDANAPVAVR) was used to generate chicken anti-T129 peptide IgY antibodies (Genway Biotech, San Diego, CA). The antibodies were purified and conjugated to beads by Genway Biotech. A stable isotope labeled T129-IS2 peptide cross-linked on beads was used to purify anti-T129 peptide IgY antibodies without risk of contaminating the purified Ab with T129 peptide, thereby increasing assay sensitivity.
Matrix Sera Pool
The matrix sera pool (matrix sera pool) was obtained by pooling human sera with Tg less than 0.2 ng/mL and ATG less than 20 IU/mL. The matrix sera pool was used as the matrix for making the calibration sample series. The matrix sera pool was stored in 1- or 2-mL aliquots at −80°C.
Serum Sample Reduction, Alkylation, and Trypsin Digestions
Serum (0.1 mL) was diluted with 0.4 mL reduction buffer containing 125 mM NH3HCO3, 0.0086% Tween 20 and 12.5 mM dithiothreitol. The reduction was performed in a 37°C oven for 1 hour with rotation. Samples were alkylated in the dark with −005 mL of 200 mM iodoacetamide for 60 minutes with gentle shaking at room temperature.
Two sequential tryptic digestions were undertaken: the first digestion used 0.006 mg of trypsin for 4 hours at 37°C while rotating. The second digestion was effected with 0.02 mg of trypsin for 16 hours at 37°C while rotating.
Affinity Purification of Tg Peptides
Antibody beads (0.03 mL; 1 mg antibody/mL beads) and 0.05 mL of 1.25 fmol/μL T129 internal standard peptide were added to each well in a Captiva 96-well filter (20 μm pore size) plate (Varian, Palo Alto, CA). Digested serum sample was transferred to the filter well, followed by incubation at room temperature for 2 hours with moderate rotating/shaking. The plate was centrifuged to remove unbound serum peptides. The beads were washed twice with 0.9 mL 1× TBS buffer and the plate was centrifuged after each wash. Bound peptides were eluted with 60 μL of 2% formic acid in 100 mM glycine at room temperature with shaking for 15 minutes and then centrifuged. The elution procedure was repeated one more time. The total elution solution was combined to obtain 0.12 mL final solution.
Two-Dimensional LC-MS/MS
A 0.1-mL final solution was loaded on a 2-dimensional LC-MS/MS system, gradients were applied, and the peptides of interest were eluted and detected by MS/MS in MRM mode. The 2-dimensional LC system is a Cohesive Aria TX-4 system. Waters Oasis HLB extraction column (Waters Corporation, Milford, MA) with relative large particle size (25 μm, 2.1 × 20 mm) was used. This extraction column can eliminate large peptides and undigested proteins getting into the analytical column but retain the peptide of interest. The analytical column is a Luna C8, 2.0 × 50 mm (Phenomenex, Tustin, CA). Peptides retained by extraction column are eluted by 40% methanol (MeOH) in 0.2% acetic acid. The MeOH percentage is reduced before reaching the analytical column and the peptide is retained on the C8 analytical column. A gradient (24% to 60% MeOH) is then applied to elute the peptide of interests in 4 minutes.
The mass spectrometer used was an Agilent Technologies (Santa Clara, CA) 6490 Triple Quadruple Mass Spectrometry with Jet Stream and iFunnel Technology. The quantitation was completed using Mass Hunter software (Agilent Technologies). The peptide of interest was detected in MRM mode with the m/z transitions for T129 from 636.42+ to daughter ion 1059.6 1+ and for T129-IS1 (the internal isotope labeled peptide) from 642.32+ to daughter ions of 1071.41+. T129 peptide peak areas were normalized to the peak area of the internal standard peptide (IS1). Normalized peptide peak areas were then converted to Tg concentrations using a calibration curve generated from external human Tg standard (Fitzgerald Industries International, North Acton, MA) in matrix sera pool.
Study Sample Source
All patient samples used in this validation study were anonymized, discarded sera submitted to the Quest Diagnostics Nichols Institute. The scope and nature of this study was reviewed and considered exempt by the Western IRB (Olympia, WA).
Results
Two-Dimensional LC-MS/MS Assay Parameters
Initial experiments focused on determining the limits of detection, precision, and linearity of the 2-dimensional LC-MS/MS assay.
Sensitivity—The limit of detection was determined by running a serum pool (ATG < 20 IU/mL and Tg by IMA < 0.2 ng/mL and undetectable by LC-MS/MS) 20 times in 1 assay. The counts associated with the Tg peak region were averaged and the mean (4SD) value was then back-calculated as a concentration from the standard curve; the limit of detection was determined to be 0.3 ng/mL. The LOQ was set as the point where replicate values have a CV of less than or equal to 20%. Serum pools containing 5 different levels of Tg (0.8–12.5 ng/mL) were run in 3 separate assays and the mean and SD determined to calculate the CV (11.4% to 0.8%, respectively). Extrapolation of the %CV versus Tg concentration curve to 20% gave an LOQ for the Tg by LC-MS/MS assay of 0.4 ng/mL.
Precision—Three levels of QC (Tg concentrations, 7.1, 23.7, and 57.4 ng/mL) were run 7 times in 1 assay and the mean, SD, and CV calculated for each level. The intra-assay CV for each level was determined to be 7.7%, 7.4%, and 7.6%, respectively.
Reproducibility—Three levels of QC (Tg concentrations, 7.1, 23.7, and 57.4 ng/mL) were run at least twice in 12 separate assays on 7 days. The reproducibility (interassay variation) was determined by calculating the mean, SD, and CV for each level of QC. The interassay variations determined were 13.0%, 13.1%, and 9.8%, respectively.
A stock solution of purified human Tg [200 ng/mL in control serum (Tg and ATG negative)] was serially diluted in control serum (Tg and ATG negative) 7 times to give a range of Tg concentrations from 3.1 to 100 ng/mL. These sample were run in triplicate and the observed versus expected results were used to assess recovery. Recoveries varied from 91.6% to 114.1% with an r2 of 0.997 and a slope of 0.998 and intercept of 0.12.
Tg Recovery from Autoantibody Positive (ATG+) and Negative (ATG−) Patient Sera
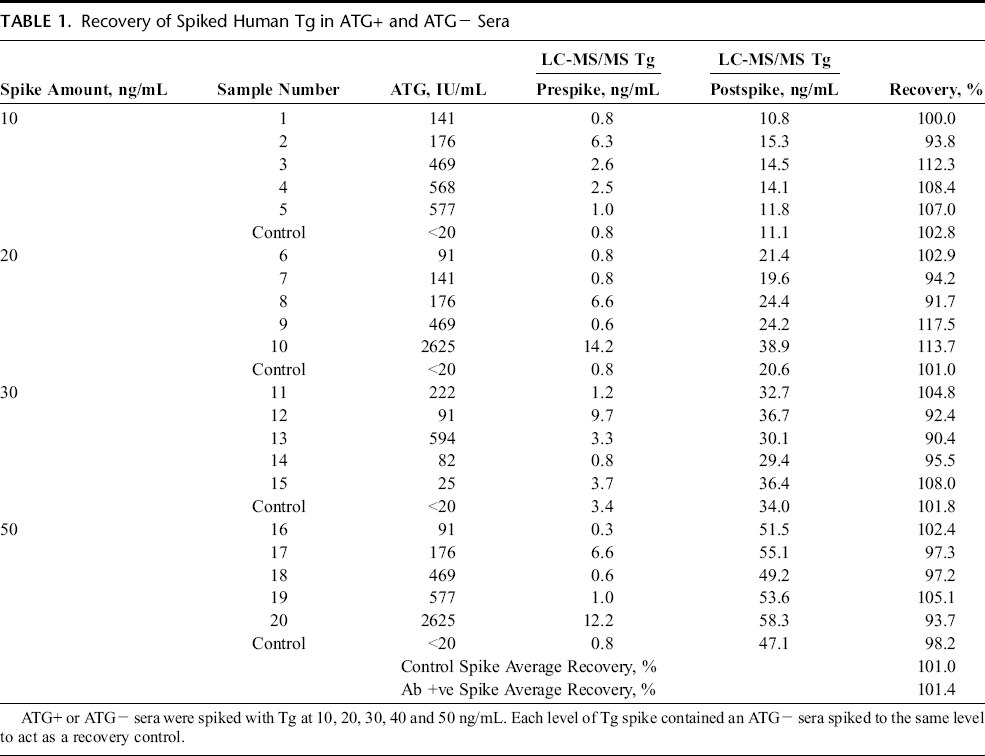
A prerequisite to developing this method was the necessity of demonstrating the efficiency of Tg recovery from serum samples. This is problematic in sera containing anti-Tg antibodies (ATG+) because the existing immunometric methods show significant biases that may or may not be linear with increasing Tg concentration and may well be patient specific. To this end, a series of Tg “spike and recovery” tests were undertaken using both ATG− and ATG+ sera. ATG+ sera were assayed both before and after spiking with known concentrations of purified human Tg. Results for ATG+ sera are shown in Table 1. Recoveries were determined by comparing the measured difference in Tg values in the spiked samples versus the unspiked samples and converting these into a percentage of the amount of purified Tg added. A similar approach was undertaken with ATG− sera. From these experiments, it was determined that the LC-MS/MS assay efficiently recovered (90%–117.5%) Tg from ATG+ samples, average recovery 101.4% (range, 90%–117%). The recoveries were similar to those measured for ATG− sera, average recovery 101.0% (range, 98%–103%) (Table 1).
Recovery of Spiked Human Tg in ATG+ and ATG− Sera
Comparison of the Tg by LC-MS/MS Assay with IMAS in ATG− and ATG+ Sera
Initial studies were performed to compare the performance of the LC-MS/MS TG assay with existing immunometric methods (2 IMAs) in ATG− sera. This analysis permitted us to confirm that the LC-MS/MS assay was behaving as anticipated and highlight any methodological issues when applied to patient samples. Thyroglobulin levels were initially quantitated in ATG− sera using the primary IMA and LC-MS/MS assay. The results of this comparison are shown in Figure 1A. Good correlation was observed in all cases with Deming regression providing correlations of LC-MS/MS = 1.06 * IMA − 0.53. This correlation was confirmed on a second, unrelated immunoassay platform and gave a similar slope and intercept (LC-MS/MS = 0.97 * IMA + 0.59, data not shown). The residual plot (Fig. 1B) shows equal scatter around zero indicating little bias or method dependency between the 2 methods. Correlation data were unavailable for the LC-MSMS compared to a Tg RIA assay in ATG− sera.
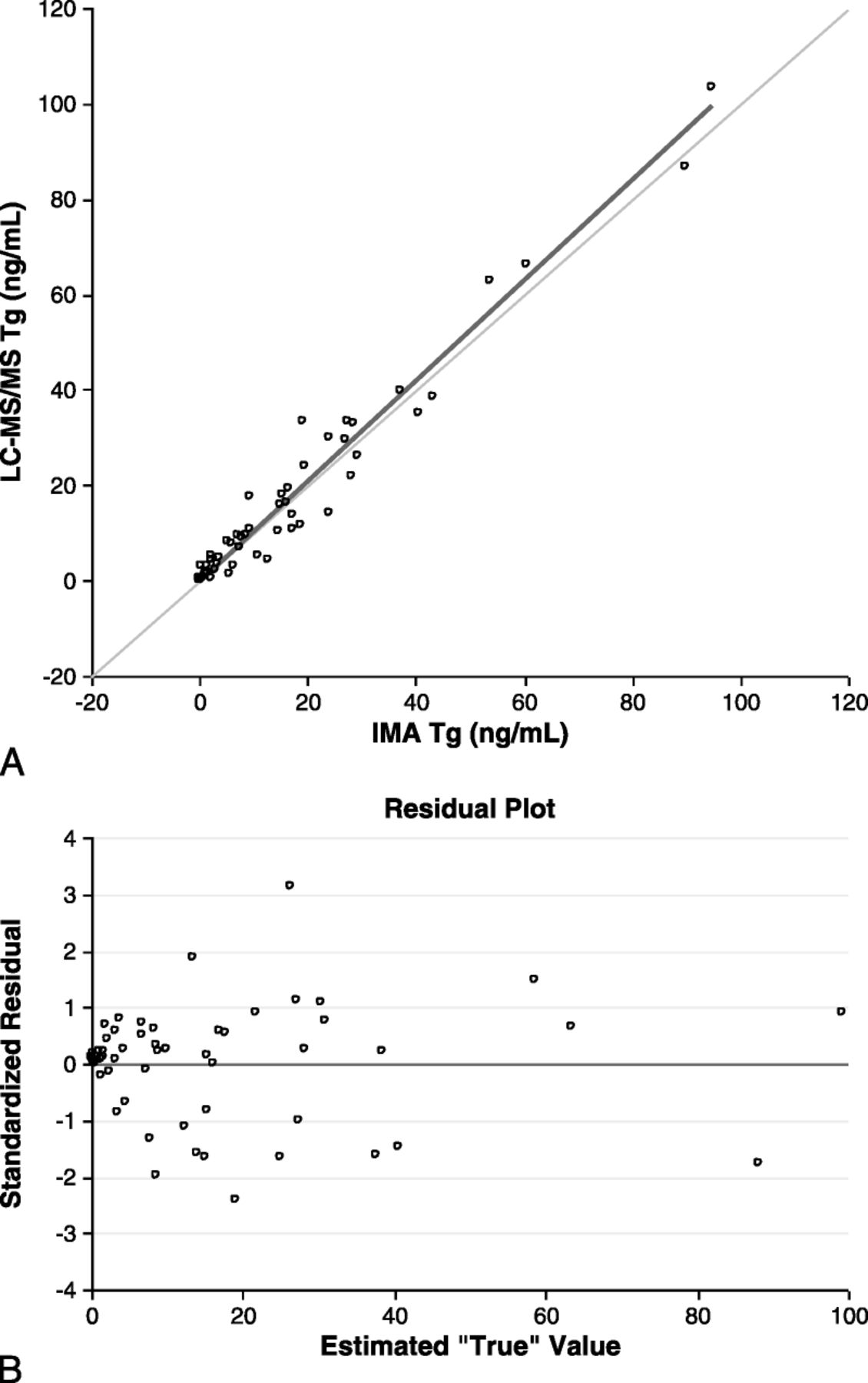
Comparison of the measurement of Tg by the LC-MS/MS assay with the primary IMA in ATG− sera. A, Deming regression of the IMA versus the LC-MS/MS Tg measurements. B, The residual plot of the IMA versus LC-MS/MS comparison.
In a similar manner, the LC-MS/MS Tg assay was used to measure Tg in ATG+ sera and compared to the IMA and RIA. A comparison between the results obtained using the primary Tg IMA and the LC-MS/MS assay are displayed in Figure 2A and B. As expected, the LC-MS/MS results were significantly higher than those obtained with the IMA (Fig. 2A, LC-MS/MS = 4.48 * IMA − 0.42). In fact, there were no samples in which the IMA results were higher than the MS/MS results and only 2 patients had the same results by both methods.
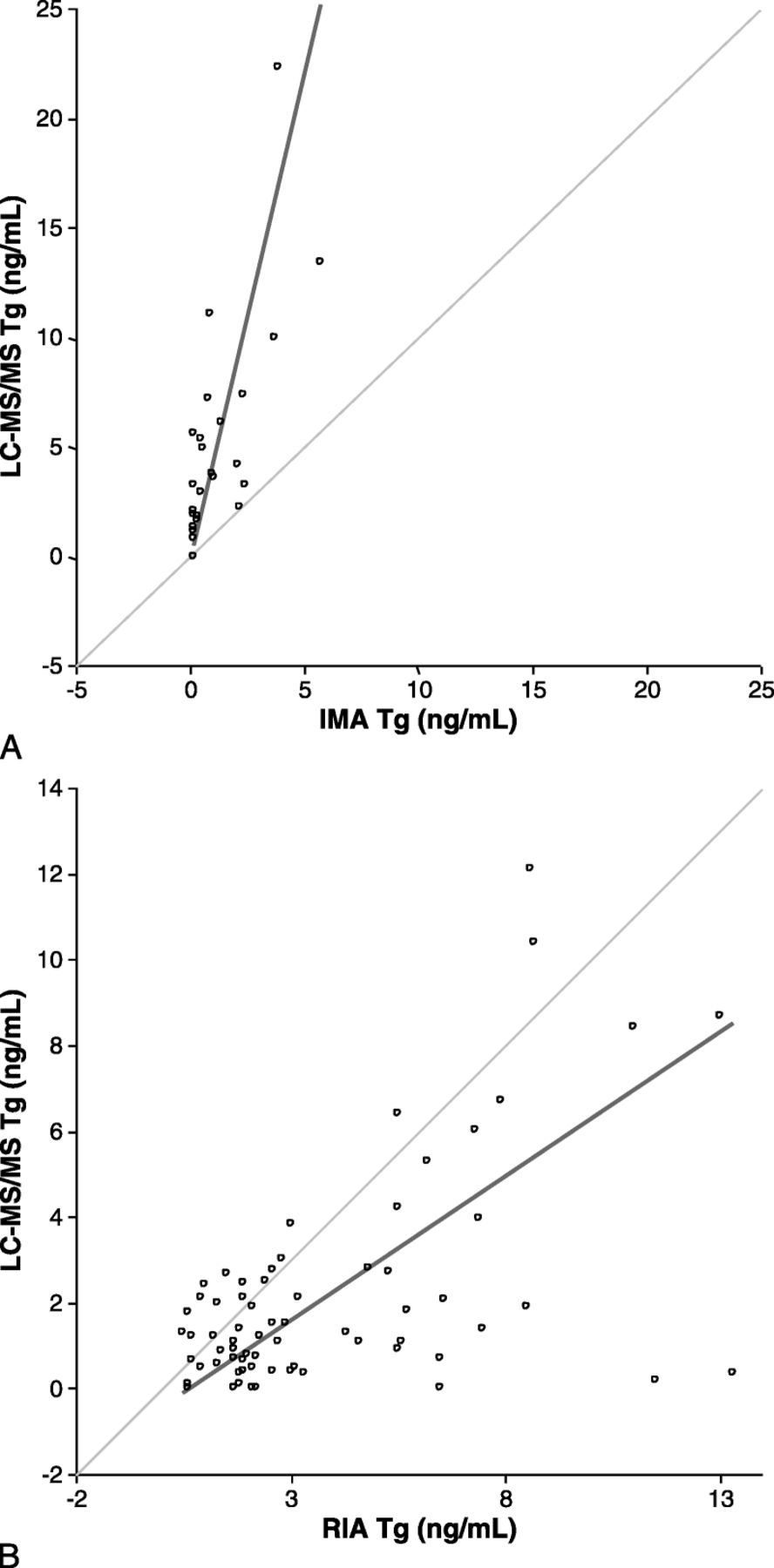
Comparison of the Tg by LC-MS/MS assay with immunoassays in ATG+ Sera. A, Deming regression analysis of the primary IMA versus LC-MS/MS Tg comparison. B, Deming regression plot of RIA versus LC.MS/MS.
Figure 2B shows the results from the comparison of samples measured with the RIA and the LC-MS/MS Tg assays. It is clear that although there is a significant bias in a large portion of the sample population, a significant number had comparable results to the MS assay, highlighting the improved performance of the RIA versus the IMA. However, there is still a very high proportion (>50%) of patients which exhibit a very high positive bias compared with the MS/MS results. The overall correlation was found to be LC-MS/MS = 0.68 * RIA − 0.5.
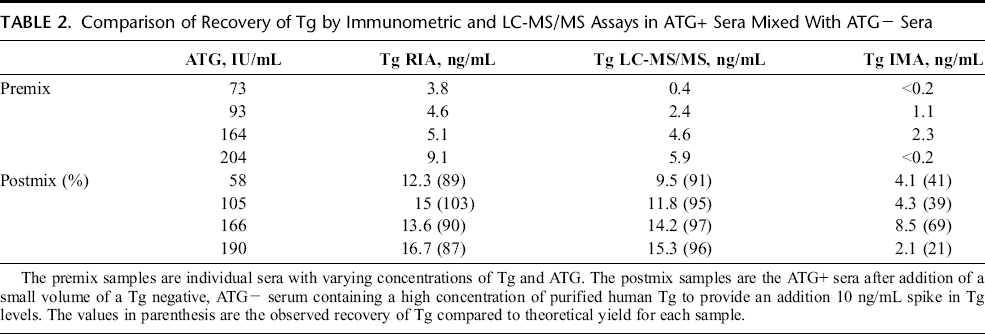
To address the question of whether there was any correlation between Tg measurement and ATG concentration, 4 separate sera covering a range of ATG autoantibody concentrations (73–204 IU/mL) were obtained and split into 2 aliquots. One aliquot of each serum sample was spiked with a final additional Tg concentration of 10 ng/mL using an ATG− patient sample containing very high Tg concentration (to minimize the dilution of the ATG+ sera). After allowing the samples to equilibrate, the 8 samples (1 spiked and 1 native per ATG+ sera) were analyzed on the LC-MS/MS, IMA and RIA platforms. The results are shown in Table 2. As predicted, in the unspiked samples, the IMA gave results lower than the LC-MS/MS which in turn gave results lower than the RIA. Of greater interest, the spiked samples clearly show a very significant low bias in the IMA compared to the expected values (21%–69% recovery), with the LC-MS/MS producing results close or identical to the expected values (95%–97% recovery) and the RIA producing similar but more varied recoveries than the LC-MS/MS (87%–103%).
Comparison of Recovery of Tg by Immunometric and LC-MS/MS Assays in ATG+ Sera Mixed With ATG− Sera
Discussion
In the management of thyroid cancer, successful treatment is confirmed by the absence of detectable Tg in sera and serum Tg measurements are then monitored over time. The detection of Tg in a patient previously negative for serum Tg or an increase in Tg concentrations in successive measures is a good indicator of recurrence or progression of DTC. The monitoring of Tg in a substantial number of patients with DTC (approximately 25%) is complicated by the presence of anti-Tg autoantibodies, which are known to interfere in the accurate measurement of Tg. 10 How these autoantibodies affect immunoassays varies depending on the type of assay. In 2-site IMAs, such antibodies typically give artificially low Tg concentrations. In competitive RIA assays, they may cause falsely increased Tg concentrations. Furthermore, there is no certain way of determining whether an autoantibody has had an effect on the result of an individual assay, making any measurement of Tg in patients with anti-Tg autoantibodies potentially unreliable. An additional concern is the fact that the available ATG assays all recognize different aspects of the interaction of the autoantibody with Tg. 11 This raises the additional possibility that apparently negative ATG sera may contain undetected autoantibodies that might influence individual Tg assay results.
To address these shortcomings, we have developed and validated the first LC-MS/MS method capable of measuring Tg accurately and precisely in both ATG negative and ATG positive sera. The measurement of Tg using this method is unaffected by autoantibodies, as all serum proteins—including Tg and ATG—are completely digested by trypsin in the earliest phases of the assay. The isolation of a unique Tg-specific peptide and an exogenously added internal standard using an antibody specific for this unique Tg peptide permits the enrichment and measurement of these Tg peptides in all sera, down to a detection limit of 0.4 ng/mL.
To confirm that we are able to measure Tg accurately, we compared it to 2 commercial IMAs in ATG− sera. We were able to demonstrate good correlation of the Tg LC-MS/MS assay with an IMA: primary IMA, LC-MS/MS = 1.06 * IMA − 0.53, secondary IMA LC-MS/MS = 0.97 * IMA + 0.59. However, as expected this correlation was lost in ATG+ sera. The LC-MS/MS assay compared to the primary IMA showed low Tg concentrations In the IMA (LC-MS/MS = 4.48 * IMA – 0.42). Compared to the LC-MS/MS, the RIA showed predominantly elevated levels (LC-MS/MS = 0.44 * RIA – 0.43).
To confirm that the LC-MS/MS was indeed detecting Tg accurately and that the differences between the immunoassays and LC-MS/MS assays was not a reflection of the differences in methodology, we performed “spike and recovery” experiments to demonstrate that the LC-MS/MS was measuring the true concentration of Tg in the presence of autoantibodies. In these studies, we were able to show an average recovery of spiked Tg of 101.0% and 101.4% in ATG− and in ATG+ sera containing various titers of ATG, respectively. Furthermore, in comparison with the IMA and RIA method on a series of ATG+ samples mixed with an ATG− pool, the LC-MS/MS gave an average recovery of Tg of 95.8% (1.0%) [mean (SD)] and was therefore not affected by the concentration of ATG present in the sera. The IMA under recovered in all samples {average recovery [42.5% (21.2%)]}, whereas the RIA showed similar recovery [92.2% (7.9%)] to the LC-MS/MS, but was more varied. Overall, these data indicate that the LC-MS/MS assay is capable of accurately measuring Tg concentrations in both ATG− and ATG+ sera.
Conclusions
We present a novel mass spectrometry–based Tg assay which accurately and precisely measures Tg concentrations in both the presence and absence of Tg autoantibodies. The data analyzed in these experiments suggest that the titer of autoantibody present is of little significance-rather it is more likely that the affinity of the antibody(ies) in individual patient samples may influence the final result obtained if the antibodies are not digested before analysis. We believe this new assay to be superior to the current standard-of-care testing as it quantifies Tg after autoantibodies have been digested in advance of any measurement. The application of this method to the clinical measurement of Tg levels may lead to early identification of cancer reoccurrence in patients with Tg autoantibodies, potentially permitting improved treatment and improved outcomes. Because different automated platforms may be discordant when identifying presence/absence of autoantibodies to Tg in individual patients, it is possible that the mass spectrometry assay as defined in this article may become the assay of choice for all determinations of Tg in patients with thyroid cancer.
Footnotes
Acknowledgments
The authors thank Michael McPhaul and Michael Caulfield for the large amount of help, hard work, editing, and suggestions provided in the preparation of this article.