
Abstract
Background
Several studies have suggested that inflammation and infection may be important for accelerated progression of atherosclerosis, but few data are available on subjects with early stages of atherosclerosis.
Methods and Results
We included, in a prospective 5-year follow-up study, 150 patients with subclinical carotid atherosclerosis, evaluating at baseline all established traditional cardiovascular risk factors (eg, older age, male sex, obesity, hypertension, diabetes, smoking, family history of coronary artery disease, and dyslipidemia); 2 markers of inflammation, fibrinogen, and high-sensitivity C-reactive protein (CRP); and the seropositivity to Helicobacter pylori, Chlamydia pneumoniae, and cytomegalovirus. After follow-up, cardiovascular and cerebrovascular events were registered in the 19% of patients, and the increment in CRP levels (in quintiles) was significantly associated with ischemic stroke (P = 0.0253), acute myocardial infarction (P = 0.0055), cardiovascular or cerebrovascular death (P = 0.0145), and the presence of any event (P = 0.0064). Most traditional cardiovascular risk factors (eg, older age, hypertension, diabetes, and dyslipidemia) were significantly associated with the events but only in the unadjusted analysis; in fact, at logistic regression analysis, among all baseline variables, only elevated CRP levels showed a predictive role (odds ratio, 7.0; 95% confidence interval, 2.2-18.4; P = 0.0247).
Conclusions
Our findings suggest that elevated CRP concentrations may significantly influence the occurrence of cerebrovascular and cardiovascular events in patients with baseline subclinical carotid atherosclerosis. Notably, null findings were obtained by viral and bacteria titers, suggesting a greater role of inflammation (and not of infection) in the progression of atherosclerosis in our cohort. However, further studies are needed to evaluate the therapeutic implications in this category of patients.
Introduction
In recent years, several studies have used the measurement of carotid intima-media thickness (IMT) as a marker of early atherosclerosis: IMT has been shown to correlate significantly with the presence of coronary artery disease (CAD) and to predict fatal and nonfatal cerebrovascular and cardiovascular events.1–7 These findings highlight the importance of recognition and management of early stages of atherosclerosis for an effective cardiovascular prevention.
Beyond traditional established cardiovascular risk factors, inflammation has been shown to be crucial throughout the time course of atherosclerosis from endothelial dysfunction to plaque rupture and thrombosis. 8 Several studies have shown the existence of a strong relation between CAD and fibrinogen or C-reactive protein (CRP) levels,9,10 and their predictive role has been examined through stratifications or multivariable statistical analyses: levels of these markers of inflammation have been independently associated with the incidence of coronary events after adjusting for traditional cardiovascular risk factors.11,12 Based on these evidences, the National Cholesterol Education Program identified, in the Adult Treatment Panel III, these markers of inflammation as emerging risk factors for coronary heart disease, 13 suggesting that their measurement may adjust the estimations of absolute risk obtained using traditional risk factors. 14 A number of studies have also addressed the possible role of infectious agents in the pathogenesis of cerebrovascular and cardiovascular diseases. 8 In the last years, 1 virus (Cytomegalovirus) and 2 bacteria (Chlamydia pneumoniae and Helicobacter pylori) have gained interest as potential pathogens causing clinical manifestations of atherosclerosis, based on experimental, seroepidemiological, or pathological evidences.15–17
However, even if the role of infection and inflammation in CAD development and progression has been extensively tested, very few studies were performed on patients with early stages of atherosclerosis.7,18–20 Therefore, we included, in a prospective 5-year follow-up study, 150 patients with subclinical carotid atherosclerosis, evaluating at baseline all the established traditional cardiovascular risk factors (eg, older age, male sex, obesity, hypertension, diabetes, smoking, family history of CAD, and dyslipidemia), as well as levels of CRP and fibrinogen and the seropositivity to H. pylori, C. pneumoniae, and cytomegalovirus.
Patients and Methods
Patients
We studied 150 subjects with subclinical carotid atherosclerosis (see “Echo Color Doppler Examination of Carotid Arteries” section), 93 male and 57 female subjects, selected from a total number of approximately 1100 patients, all referred for a clinical evaluation in our Unit of Cardiovascular Prevention. Subjects were physician referred and self-referred to our unit. According to the clinical inclusion/exclusion criteria (see next paragraph), we came up to a total number of 613 subjects potentially eligible for our study; of them, we included in the present study those with subclinical carotid atherosclerosis (n = 150), as assessed by carotid echo color Doppler (see below in “Echo Color Doppler Examination of Carotid Arteries”).
The project design included a medical examination, biochemical analyses, and the echo color Doppler of carotid arteries. The adopted procedures were in agreement with the Helsinki Declaration of 1975 as revised in 1983 and were approved by the Ethic Council of the Department of Internal Medicine of the University of Palermo. All subjects gave their informed consent to participate to the study. At admission, all subjects underwent a medical examination and also answered a questionnaire on personal and medical items, including age, medical history, and use of medications. Subjects were included in the study if their age was in the range of 40 to 80 years, whereas they were excluded if they had a history of atrial fibrillation, peripheral artery disease, coronary revascularization, angina pectoris, myocardial infarction, carotid surgery, or cerebrovascular event. None of the subjects included in the study had clinical evidence of connective tissue disease, liver dysfunction, or renal failure or received treatment with antibiotics or steroids shortly before commencing the study.
Among the main cardiovascular risk factors, the presence of family history of CAD (in a first-degree relative before 55 years), hypertension (systolic or diastolic blood pressure respectively higher than 140 and 90 mm Hg or pharmacological therapy with antihypertensive drugs), diabetes (fasting glucose plasma concentrations higher than 126 mg/dL or pharmacological therapy with antidiabetic drugs or insulin), and smoking habits were considered. Height and weight were recorded, and body mass index (BMI) was expressed as kilograms per square meter. Participants were categorized as having obesity if BMI was 30 kg/m2 or greater.
Biochemistry
A blood sample was drawn in the morning, before the medical examination, after a 12 to 14 hours of overnight fast. Total cholesterol, triglycerides, and high-density lipoprotein (HDL) cholesterol were quantified by standard enzymatic-colorimetric methods, 21 and low-density lipoprotein (LDL) cholesterol was calculated by the Friedewald formula. High-sensitive (hs) CRP was determined by the nephelometric method (Beckman Instrument APS), 22 and we considered high levels those greater than 3 mg/L, as previously reported.7,23 Fibrinogen determination was rapidly performed according to the coagulative method of Clauss 24 ; using this method, the reference laboratory values range between 200 and 350 mg/dL, and we considered high levels those greater than 350 mg/dL, as reported.7,25 Immunoglobulin G (IgG)-specific antibodies for C. pneumoniae, cytomegalovirus, and H. pylori were measured by immunoenzymatic methods (enzyme-linked immunoassay). 7 As already reported, we considered positive anti-C. pneumoniae IgG titers of 1.1 or greater, 26 anti-cytomegalovirus IgG titers of 11 U/mL or greater, 16 anti-H. pylori IgG concentrations of 30% or greater, 27 or anticytotoxic H. pylori titers of 7.5 U or greater. 28
Echo Color Doppler Examination of Carotid Arteries
B-mode real-time ultrasound was performed in blind in all 613 subjects potentially eligible for our study, evaluating the arterial wall thickness in the carotid arteries with a machine Toshiba 270 SS and a probe of 7.5 to 10.0 MHz (Toshiba, Tokyo, Japan). As already reported,7,29 patients were examined in the supine position, and each carotid wall or segment was examined to identify the thickest intimal-medial site. Each scan of the common carotid artery began just above the clavicle, and the transducer was moved until the carotid bifurcation and along the internal carotid artery. Three segments were identified and measured in anterior and posterior planes on each side: the distal 1.0 cm of the common carotid proximal to the bifurcation, the bifurcation itself, and the proximal 1.0 cm of the internal carotid artery. At each of these sites, we detected any possible plaque and determined the IMT defined as the distance between the echogenic line representing the intima blood interface and the outer echogenic line representing the adventitia junction. According to the most recent guidelines of the joint European Society of Hypertension/European Society of Cardiology, 30 we distinguished our 613 subjects potentially eligible for our study in 3 groups by carotid echo color Doppler: “subjects with normal IMT” (with IMT below 0.9 mm, n = 187), “subjects with subclinical carotid atherosclerosis” (with IMT between 0.9 and 1.5 mm, n = 150), and “subjects with carotid plaques” (with IMT above 1.5 mm, n = 276). We included in the present study the 150 subjects with IMT.
Follow-up
We performed a 5-year follow-up study in all patients to evaluate cerebrovascular and cardiovascular morbidity and mortality and to assess if baseline clinical and laboratory variables were predictive of these clinical events. Regarding the use of cardiovascular medications, during the follow-up, patients received treatment with β-blockers (24%), angiotensin-converting enzyme inhibitors (28%), calcium entry blockers (28%), diuretics (16%), statins (45%), and antiplatelet drugs (35%). The protocol included that none of the patients had to receive antibacterial or anti-inflammation therapy during the follow-up. However, we cannot exclude that persons took such therapies in 5 years; this fact, however, did not lead us to drop out patients from follow-up because we were observing the investigated population during their normal life and activity.
Clinical events were registered in the 19% of patients and included the following: transient ischemic attack, stroke, effort or unstable angina, acute myocardial infarction (AMI), peripheral arterial disease, cerebrovascular and cardiovascular death. Transient ischemic attack was defined as a brain deficit caused by vascular disease that clear completely in less than 24 hours. Effort angina was defined by the presence of chest pain upon walking that was relieved within 10 minutes after stopping or by ST segment downsloping in a standard 12-lead electrocardiogram during chest pain or by positive stress testing. Acute myocardial infarction was defined by a pronged episode of chest pain with electrocardiogram and/or specific myocardial enzyme changes, involving hospitalization. Peripheral arterial disease was defined by the self-reported presence of pain in the lower extremities while walking that was relieved within 10 minutes after standing still, with an ankle/brachial pressure index of less than 0.90 and a positive treadmill test. All clinical events were captured by clinical visits in our Unit of Cardiovascular Prevention; complete follow-up was performed for every subject, with the exception of 5 patients who died during the follow-up. The causes of death were retrieved directly from the families and were confirmed in all cases by the general practitioners on the basis of their own records (that may include hospital records).
Statistical Analysis
Statistical analysis was performed using the Statview Program (Abacus Concepts Inc, Berkeley, CA). Relationships between baseline parameters and quintiles of hs-CRP levels were assessed using test for trend. Univariate analysis (with Student t test or χχ2 test) was used to investigate the differences in values or in the prevalences of baseline parameters in patients with clinical events versus those without clinical events. Logistic regression analysis was performed to evaluate possible independent associations of baseline parameters (including male sex; age (×10 years); smoking; hypertension; diabetes; obesity; dyslipidemia; family history of CAD; elevated levels of fibrinogen and hs-CRP; and seropositivity to H. pylori, C. pneumoniae, and cytomegalovirus) with the occurrence of clinical events, as registered in the follow-up. Correlation analysis was performed using the Spearman rank correlation method.
Results
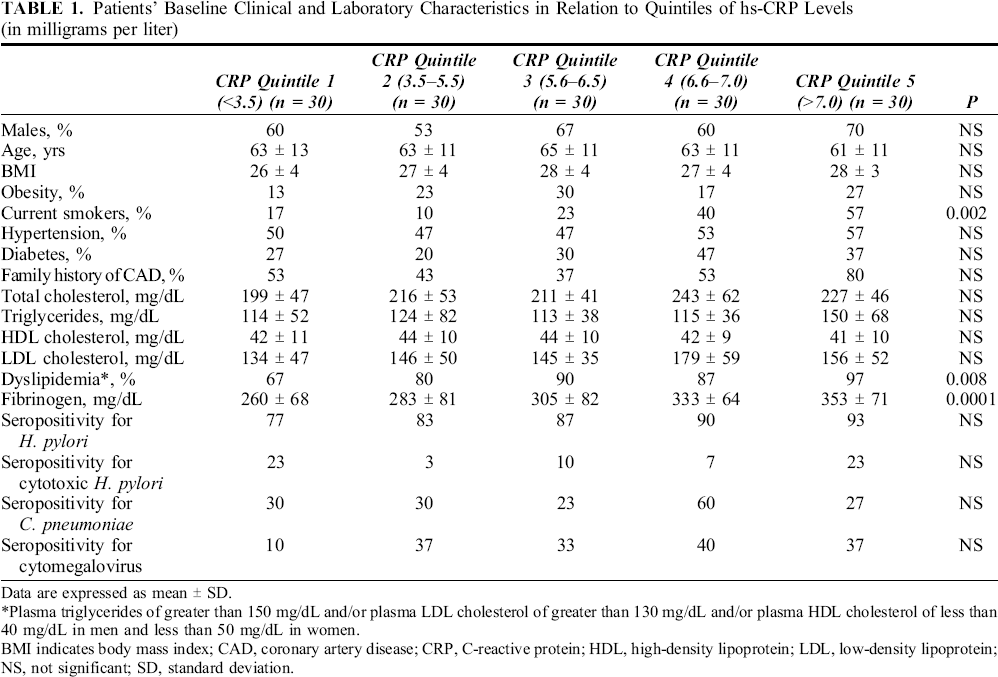
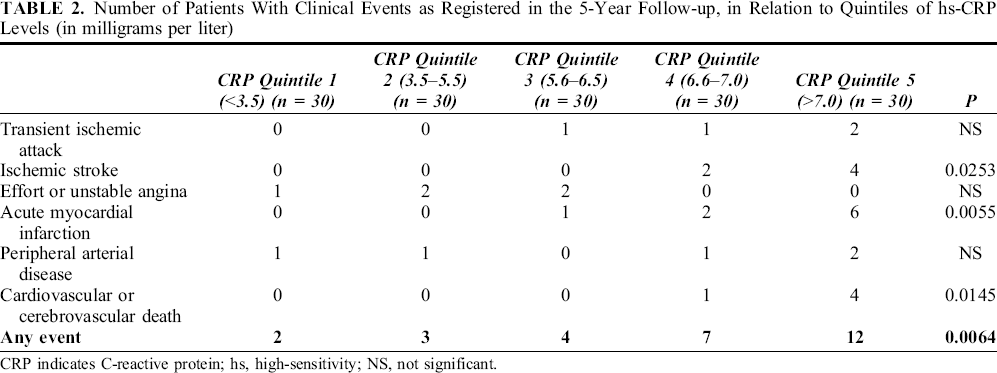
We preliminary found a strong relationship between CRP levels and IMT in our cohort (Fig. 1). Table 1 shows the baseline clinical and laboratory characteristics in all patients in relation to quintiles of plasma hs-CRP levels. The increment in hs-CRP concentrations was significantly associated with smoking (P = 0.002), dyslipidemia (P = 0.008), and plasma fibrinogen concentrations (P = 0.0001). At the end of the 5-year follow-up, we registered clinical events in the 19% of patients, and the number of patients for each individual event in relation to quintiles of hs-CRP levels is shown in Table 2. We found that the increment in hs-CRP concentrations was significantly associated with ischemic stroke (P = 0.0253), AMI (P = 0.0055), and cardiovascular or cerebrovascular death (P = 0.0145) and with the presence of any event (P = 0.0064).

Spearman correlation between C-reactive protein (CRP) levels and carotid intima-media thickness. hs indicates high-sensitivity.
Patients’ Baseline Clinical and Laboratory Characteristics in Relation to Quintiles of hs-CRP Levels (in milligrams per liter)
Number of Patients With Clinical Events as Registered in the 5-Year Follow-up, in Relation to Quintiles of hs-CRP Levels (in milligrams per liter)
We also used logistic regression analysis (Table 3) to search for possible independent associations of any of the evaluated baseline parameters with the occurrence of cardiovascular events, as registered in the follow-up. We included in the multivariate model the following variables: male sex; age; smoking; hypertension; diabetes; obesity; dyslipidemia; family history of CAD; elevated levels of fibrinogen and hs-CRP; and seropositivity for H. pylori, cytotoxic H. pylori, C. pneumoniae, and cytomegalovirus.
Multivariate Analysis of Independent Associations of Baseline Clinical and Laboratory Variables With Cardiovascular Events, as Registered in the 5-Year Follow-up
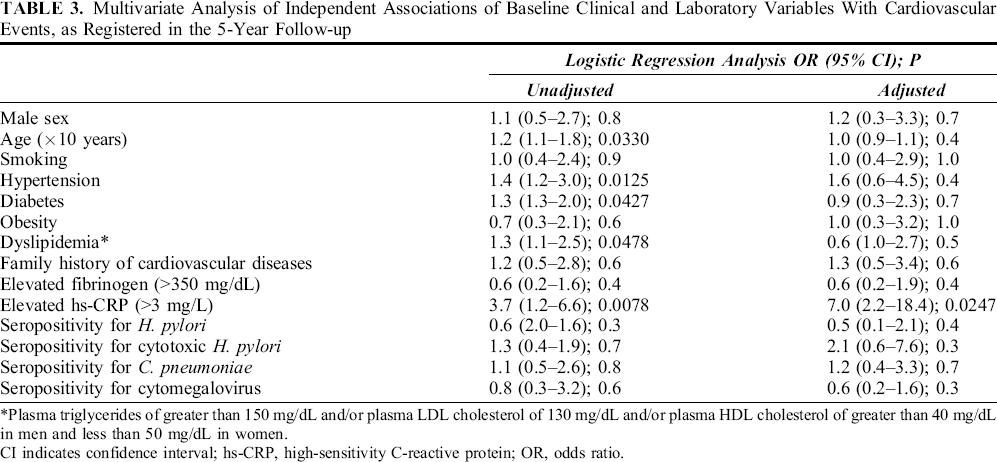
Most traditional cardiovascular risk factors (eg, older age, hypertension, diabetes, and dyslipidemia) were significantly associated with the events but only in the unadjusted analysis; in fact, at logistic regression analysis, among all baseline variables, only elevated CRP levels showed a predictive role (OR, 7.0; 95% CI, 2.2-18.4; P = 0.0247). The box plots of plasma hs-CRP levels in patients with (n = 122) and without (n = 28) events are shown in Figure 2. We also performed the same logistic regression analysis, as previously described, entering CRP levels as the upper quintile versus the first quintile (rather than CRP of >3 mg/L), and we still found (data not shown) a predictive role only for the CRP (OR, 5.5; 95% CI, 1.8-15.1; P = 0.0166).
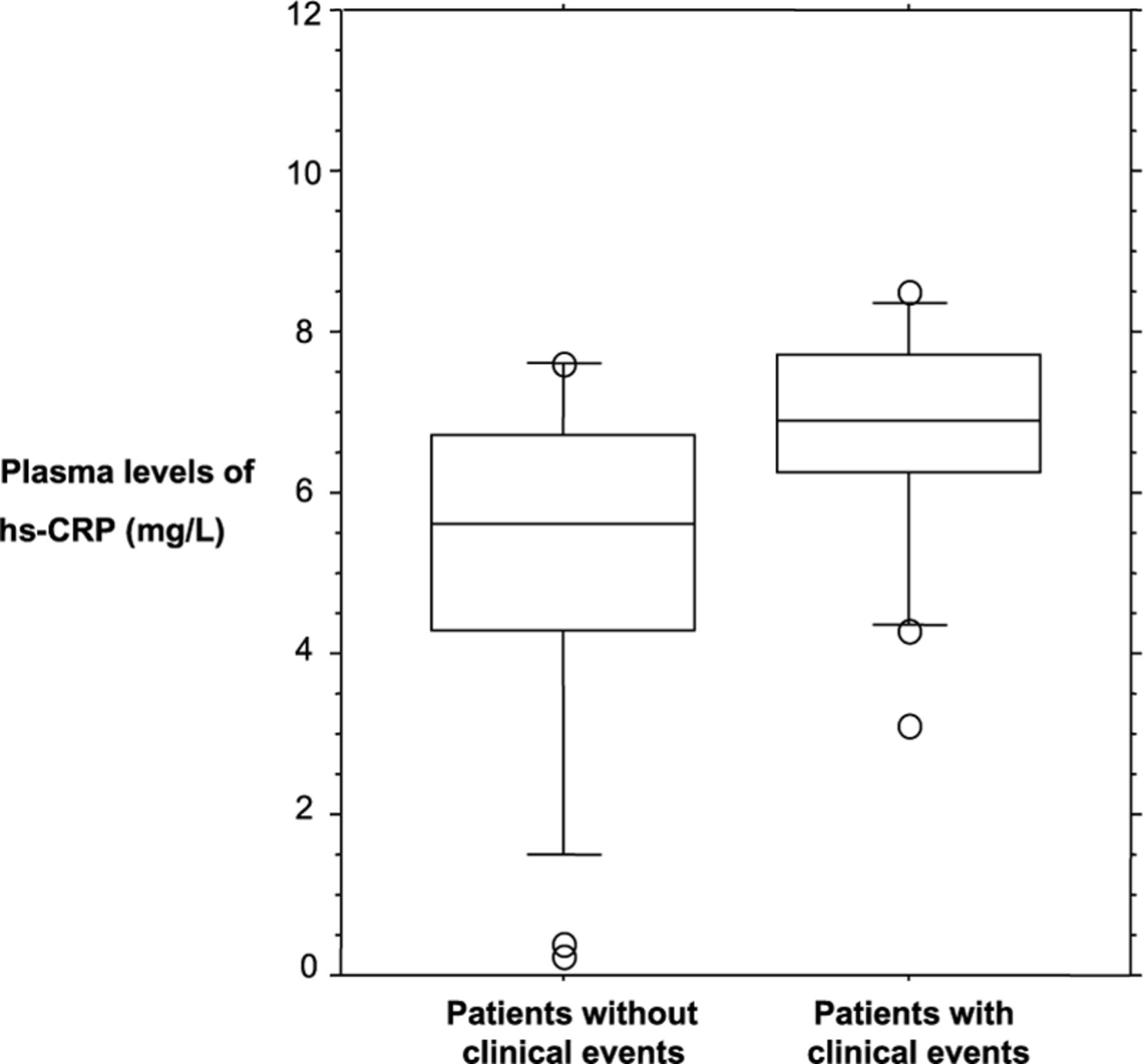
Box plots (median, 10%, 25%, 75%, 90%, and single values) of plasma high-sensitivity C-reactive protein (hs-CRP) levels in patients with (n = 122) and without (n = 28) clinical events, as registered in the 5-year follow-up.
Discussion
The pathophysiological role of markers of inflammation and infection in atherogenesis has been extensively studied, and inflammation has been particularly shown to be crucial throughout the time course of atherosclerosis from endothelial dysfunction to plaque rupture and thrombosis. 8
Regarding CRP, this protein has been found to activate in vitro a number of processes involved in inflammatory reactions, whereas in humans, endothelial cells induce expression of the adhesion molecules vascular cell adhesion molecule-1, intercellular adhesion molecule-1, and E-selectin and of monocytes chemoattractant protein-1; in human monocytes, CRP seems to stimulate production of tissue factor, an activator of the extrinsic pathway of the coagulation system. 31 Large population-based studies have suggested a relation between CAD and CRP levels, and its predictive role has been examined through stratifications or multivariable statistical adjustments: CRP has been independently associatedwith the incidence of coronary events after adjusting for the traditional cardiovascular risk factors.8,10,12 In addition, recent studies have demonstrated the ability of elevated CRP to predict coronary events in women after adjusting for risk factors used in the Framingham risk score and in the elderly with extensive adjustment for cardiovascular disease risk factors. 32
Several prospective studies have demonstrated the association between IMT and the occurrence of cardiovascular and cerebrovascular events.4,6 The measurement of carotid intima-media thickness improves cardiovascular risk assessment in patients with intermediate Framingham scores, 33 and recent studies suggest that patients with abnormal IMT should be treated more aggressively than those with normal IMT. 34 In addition, it has been suggested that measurement of carotid artery IMT may represent a more powerful predictor of cardiovascular events than traditional risk factors. 4 However, even if the role of markers of inflammation and infection in CAD development and progression has been extensively studied, very few studies addressed their role in early stages of atherosclerosis,7,18–20,35 such as in subjects with subclinical carotid atherosclerosis.
Therefore, we reasoned to include in a prospective 5-year follow-up study 150 patients with subclinical carotid atherosclerosis, evaluating at baseline all the established traditional cardiovascular risk factors (eg, older age, male sex, obesity, hypertension, diabetes, smoking, family history of CAD, and dyslipidemia), as well as levels of fibrinogen and the seropositivity to H. pylori, C. pneumoniae, and cytomegalovirus in relation to quintiles of CRP. Although many authors used tertiles of CRP, others used quartiles or quintiles,36,37 and we reasoned in the present study to use quintiles of CRP to show more clearly the potential associations between baseline clinical and laboratory variables and the increment in CRP levels. We found that the increment in CRP concentrations was significantly associated with smoking, dyslipidemia, and plasma fibrinogen concentrations; yet, we did not find any association with obesity, whereas other studies have reported obesity to be one of the main determinants of CRP levels. 36
Notably, the median of CRP concentrations in the present study (6 mg/L) is much higher than what already reported in other studies performed on US populations.36–39 This should be partially explained by the fact that Mediterranean diet seems to have no effect on such markers of inflammation, 40 and elevated CRP levels have been commonly found in healthy Mediterranean subjects. 41 Because the population included in the present study should be a less healthy cohort, given the increased IMT, the relative higher CRP levels should not be surprising. In other studies performed on European subjects with asymptomatic or symptomatic carotid lesions, CRP concentrations were somewhat similar to what was found in our population.42,43 Yet, this point has to be considered when comparing our results with those obtained in other cohorts.
At the end of the follow-up, cardiovascular and cerebrovascular events were registered in the 19% of patients, and we found that the increment in quintiles of CRP concentrations was significantly associated with ischemic stroke, AMI, and cardiovascular or cerebrovascular death and with the presence of any event When we made a comparison between the 2 groups of patients with or without the events, among all evaluated baseline variables, only the elevated CRP levels showed a predictive role at both univariate (P = 0.0016) and multivariate analysis (OR, 7.0; 95% CI, 2.2-18.4; P = 0.0247). Most traditional cardiovascular risk factors (eg, older age, hypertension, diabetes, and dyslipidemia) were significantly associated with the events registered in the follow-up but only in the unadjusted analysis; interestingly, the statistical significance was lost when adjusted in the multiple regression model. These findings highlight the role of CRP in this category of patients with subclinical carotid atherosclerosis beyond traditional established cardiovascular risk factors, markers of infection and fibrinogen plasma concentrations.
Our findings are somewhat consistent with what was very recently reported by Cao et al. 39 These authors studied the relationship between carotid atherosclerosis, CRP, and cardiovascular risk in approximately 5000 subjects, and they found that elevated CRP levels were associated with increased risk only in those with carotid atherosclerosis. Because the study by Cao et al 39 involved participants older than 65 years (with an average age of 73 years), it seems interesting that we confirmed their findings in a somewhat younger European cohort. Beyond the study of Cao et al, 39 we also evaluated the potential role of 4 different markers of infection on the cardiovascular outcome in our cohort of subjects. Notably, null findings were obtained by viral and bacteria titers, suggesting a greater role of inflammation (and not of infection) in the progression of atherosclerosis in our cohort of patients with subclinical carotid alterations.
Because it is known that cardiovascular medications may influence event risk, we also performed univariate and multivariate analyses (data not shown) for each individual group of treatment (included as nominal values) to assess any influence on the clinical events. Surprisingly, we did not find any significant result at both univariate and multivariate analyses; probably, this may be explained by the fact that no significant differences were found in all traditional cardiovascular risk factors, including hypertension, diabetes, and dyslipidemia (at both univariate and multivariate analyses) in patients with or without the clinical events, and therefore, it is likely that such treatments were well balanced between the 2 groups.
Recent studies have addressed the importance of therapeutical modulation of CRP levels in high-risk patients for the prevention of vascular events,44–47 and it cannot be excluded that an effective primary prevention on the categories of patients included in our study may take into account the reduction of the concentrations of this marker of inflammation. The strong relationship that we found between CRP and IMT in our cohort of subjects may potentially account for a complex role of CRP and IMT in the pathogenesis of cardiovascular events. However, beyond the potential use of CRP plasma level measurement for the assessment of patients with subclinical carotid atherosclerosis at higher risk of vascular events, further studies are needed to evaluate the therapeutic implications in this category of patients.