
Abstract
Morphologically, the distinction between undifferentiated embryonal sarcoma of the liver (UESL) and biliary tract rhabdomyosarcoma (RMS) can be uncertain because of some shared pathologic similarities. Patients with UESL have been consistently but erroneously enrolled in Children's Oncology Group (COG) treatment protocols because UESL was equated with RMS, despite the differing primary treatment modalities of these entities. Review of COG pathology files yielded 20 cases of UESL that were compared to 25 cases of biliary tract RMS. Clinicopathologic features including immunohistochemical staining were examined. In the UESL cases, the male:female ratio was 1:1 and the median age was 10.5 years. Histologically, hyaline globules and diffuse anaplasia were consistently present. The cases of RMS had a male:female ratio of 1.8:1 with a median age of 3.4 years and routinely lacked diffuse anaplasia and hyaline globules. Polyclonal desmin and muscle-specific actin were variably immunoreactive in UESL and RMS; however, myogenin and myogenic regulatory protein D1 (MyoD1) were uniformly negative in UESL and routinely positive in the majority of biliary tract RMS. Myogenin, in particular, was highly significant (P = 0.0003) in distinguishing RMS from UESL. With a median follow-up of 8 months, 11 of 18 patients with UESL were still alive. The estimated 5-year survival for biliary tract RMS was 66%. Establishing the correct diagnosis of these distinct clinical and pathologic entities is important, as surgery alone may be curative in UESL, whereas initial chemotherapy is often recommended for the treatment of biliary tract RMS.
INTRODUCTION
Undifferentiated embryonal sarcoma of the liver (UESL) was first recognized as a distinct clinical and pathologic entity in 1978 [1]. It is the third most frequent primary hepatic malignancy of childhood after hepatoblastoma and hepatocellular carcinoma, comprising 2% to 15% of malignant liver tumors diagnosed in the pediatric population [2–5]. Despite some consensus that UESL is not a rhabdomyosarcoma (RMS) [6], the tumor's histogenetic origin remains uncertain. Early descriptions of this tumor as an intrahepatic neoplasm [7] labeled it as a rhabdomyoblastic mixed tumor possibly related to embryonal rhabdomyosarcoma of the extrahepatic bile ducts; cross striations were even reported to be present, though difficult to find [8]. Both UESL and RMS can contain a cambium tumor cell layer with associated bile duct epithelia. A shared myogenic phenotype of UESL and RMS has even been suggested at the ultrastructural and immunohistochemical level [3,9–11], with evidence of both actin and desmin immunopositivity [11]. Comprehensive studies of UESL, including assessment of expression of myogenic intranuclear transcription factors, such as myogenic regulatory protein D1 (MyoD1), are lacking [11]. These shared phenotypic features with RMS have led institutional pathologists to expect enrollment of such patients on COG treatment protocols for RMS.
The reported 2-year disease-free survival of all of the reported pediatric cases of UESL has improved only slightly—from 17% to 27%—with chemotherapy [12]. Because the prognosis of UESL is felt to be poor and chemotherapy may not affect the outcome, curative therapy requires complete surgical resection; this means that accurate differential diagnosis is essential. With the advent of immunostains for myogenic intranuclear transcription factors (MyoD1, myogenin) as the established markers [13] for diagnosis of RMS, we sought to more clearly define the clinicopathologic features that distinguish UESL from RMS; our own pilot studies [14] of an extensive panel of antibodies in a smaller number (6) of local UESL cases [14] revealed a uniform absence of myogenin staining. Distinction of UESL from RMS is critical, as treatment of RMS may require frontline chemotherapy [15,16].
MATERIALS AND METHODS
We retrospectively reviewed the files of the Children's Oncology Group (COG) Pathology Center at Children's Hospital of Columbus, Ohio, and retrieved the records of 20 consecutive cases of UESL from 1973 through 2004. Materials from the 20 cases of UESL were compared to 25 cases of biliary tract RMS previously studied in the Intergroup Rhabdomyosarcoma Study (IRS) I to IV clinical trials over a similar time span [16]. Over the slightly more than 3 decades of the study, UESL patients were increasingly referred for enrollment into RMS protocols, with 1 referral seen between 1973 and 1982, 7 referrals between 1983 and 1992, and 12 referrals between 1993 and 2004. No biliary tract RMSs were misdiagnosed as UESLs during this time period. Clinical data and outcomes of all cases were analyzed. Final pathology reports and glass slides stained with hematoxylin and eosin, along with various special stains (periodic acid–Schiff [PAS] with diastase and reticulin) and immunohistochemical stains (muscle-specific actin [MSA], polyclonal desmin, vimentin, and myoglobin), were examined. We also performed additional immunostains using an avidin-biotin peroxidase technique [14] with primary rabbit polyclonal (MSA and desmin) or murine monoclonal (myogenin and MyoD1) (Dako Corp, Carpinteria, CA, USA) anti-human sera on available paraffin blocks or unstained slides (14 UESL, 13 RMS) with antigen retrieval technique and automated immunostaining (Dako). Immunostaining results were analyzed statistically using the chi-square test with continuity correction (for small case numbers), with significance determined at the P < 0.05 level.
RESULTS
Clinical Features
The ages of the 20 children diagnosed with UESL ranged from birth to 18 years (median 10.5 years). The cases were evenly divided by gender (male: female ratio of 1:1). These patients tended to present with increased abdominal girth and associated pain. Serum alpha-fetoprotein (AFP) and human chorionic gonadotropin (hCG) levels were unknown in many of the cases, but the levels reported in the literature are rarely increased [3]; both AFP and hCG were normal when measured in 2 of our cases. Thirteen of the tumors were confined to the right lobe of the liver. Of the remaining 7 cases, 2 had tumor extending from the right lobe into the left lobe, 2 had tumor involving the right hepatic lobe and transverse colon, 1 had tumor involving only the left hepatic lobe, and 2 had widely metastatic disease outside the liver at presentation.
The 25 cases of RMS of the biliary tract occurred in children 0.4 to 9.6 years old (mean, 3.4 years). The male-to-female ratio was 1.8:1. The tumors were most commonly found in the hilum of the liver, and the children usually presented with jaundice, with or without an abdominal mass or pain [16].
The treatments administered and outcomes of the entire cohort of 43 patients (2 UESL patients were lost to follow-up) are shown in Table 1. Eight of the 20 cases of UESL (40%) were originally diagnosed as RMS. All cases of RMS were correctly identified by the referring pathologist. Eleven of the 18 patients with UESL were alive at last contact, but follow-up was short (median follow-up, 8 months; range, 2.0 weeks to 6 years, 10 months). Follow-up on patients who are deceased was also short, with death occurring near the time of diagnosis (3 cases) or within the following year (4 cases at 1.5, 2, 5, or 11 months of follow-up). Patients with biliary tract RMS had an estimated 5-year survival rate of 66% (median follow-up, 2.3 years; range, 9 days to 7.6 years).
Treatment and survival of undifferentiated embryonal sarcoma of the liver (UESL) compared to biliary tract rhabdomyosarcoma (RMS)
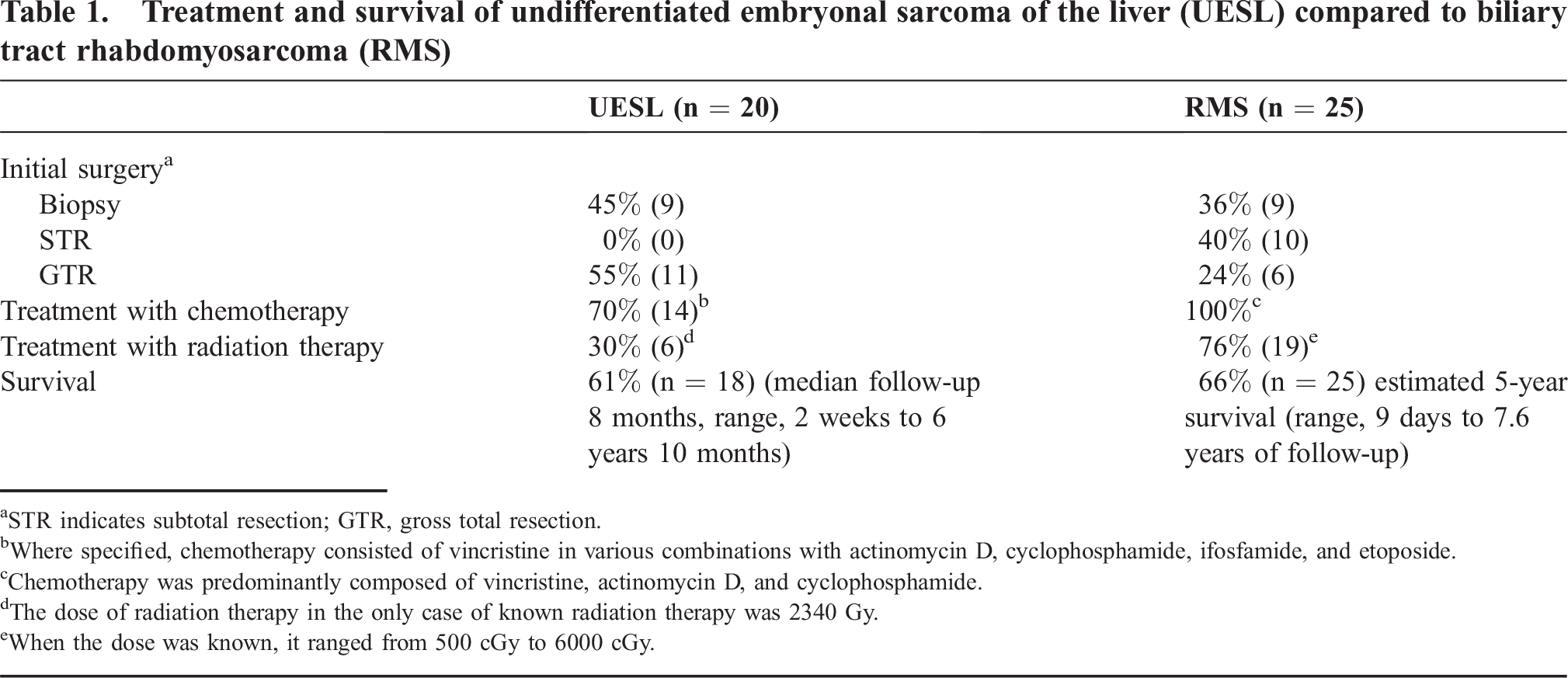
STR indicates subtotal resection; GTR, gross total resection.
Where specified, chemotherapy consisted of vincristine in various combinations with actinomycin D, cyclophosphamide, ifosfamide, and etoposide.
Chemotherapy was predominantly composed of vincristine, actinomycin D, and cyclophosphamide.
The dose of radiation therapy in the only case of known radiation therapy was 2340 Gy.
When the dose was known, it ranged from 500 cGy to 6000 cGy.
Gross and Histopathologic Features
The UESLs ranged from 3 × 5 × 6 cm to 10 × 23 × 35 cm and were typically located in the right lobe of the liver. They were white-tan and bosselated (Fig. 1); upon sectioning, there was hemorrhage and necrosis, and a pseudocapsule was present. It is important to note that because UESLs can involve or extend into the left hepatic lobe (3 cases in our studies), they can overlap in geographic area with intrahepatic RMS involving smaller bile ducts.
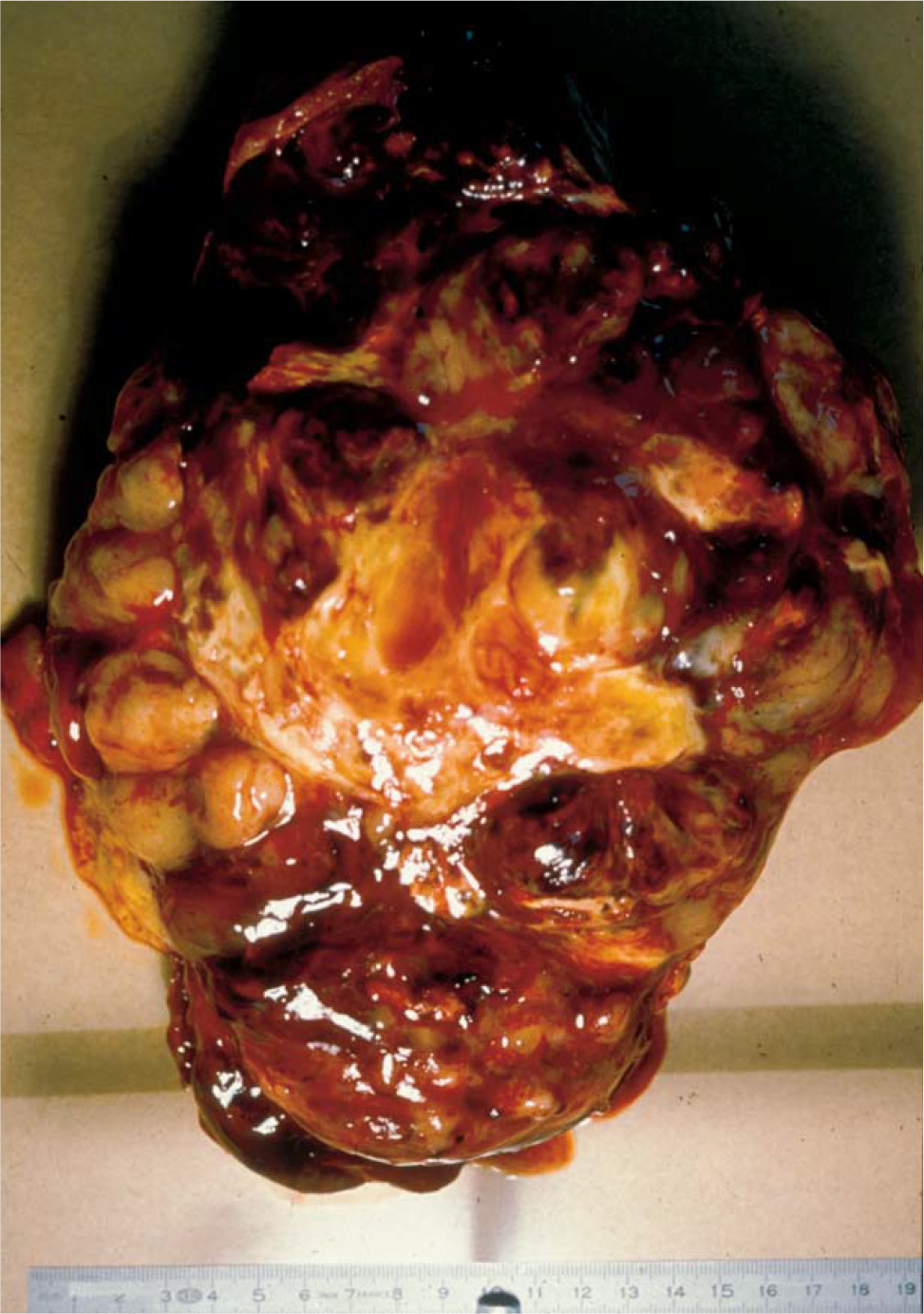
Gross specimen of a liver resection that is involved by an undifferentiated embryonal sarcoma (UESL). These tumors typically involve the right lobe of liver.
Undifferentiated embryonal sarcoma of the liver and biliary tract RMS are both malignant mesenchymal neoplasms that share some histologic features. Abundant spindle and polygonal cells can be found in a myxoid or mucinous stroma, and a cambium layer has been described as well (Figs. 2 and 3). All cases of UESL also demonstrated hyaline globules (Fig. 2C), both within the tumor cells and extracellularly, that were PAS positive and diastase resistant. These are typically not seen in RMS, but they are not pathognomonic of UESL. Anaplastic, multinucleated giant cells with prominent atypical mitoses were common in UESL (Fig. 2B) and absent in the RMS cases. Despite spindling, cross striations were not seen in the UESL cases.
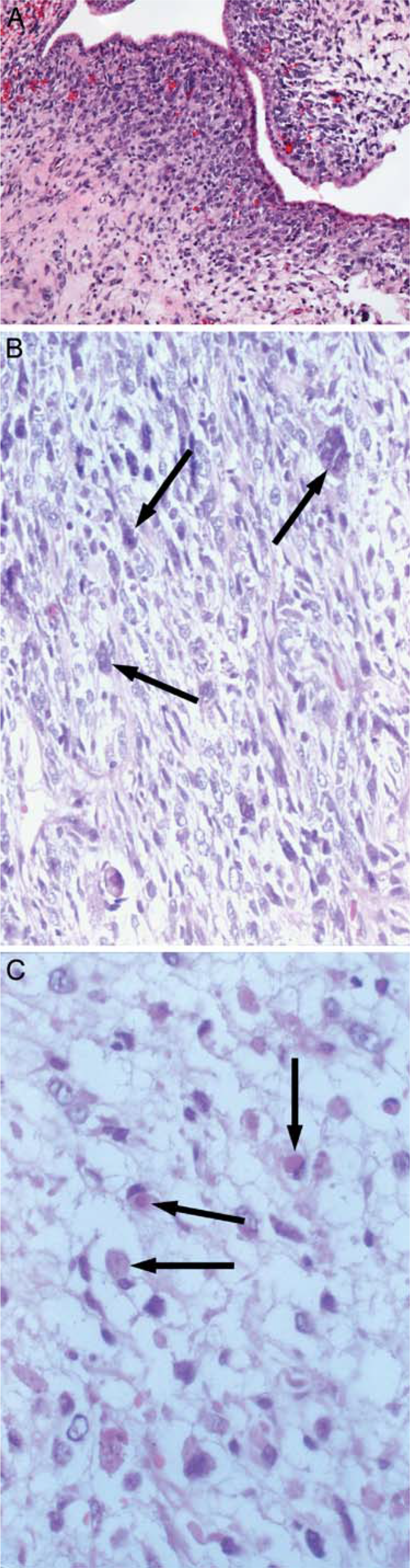
UESL demonstrating (
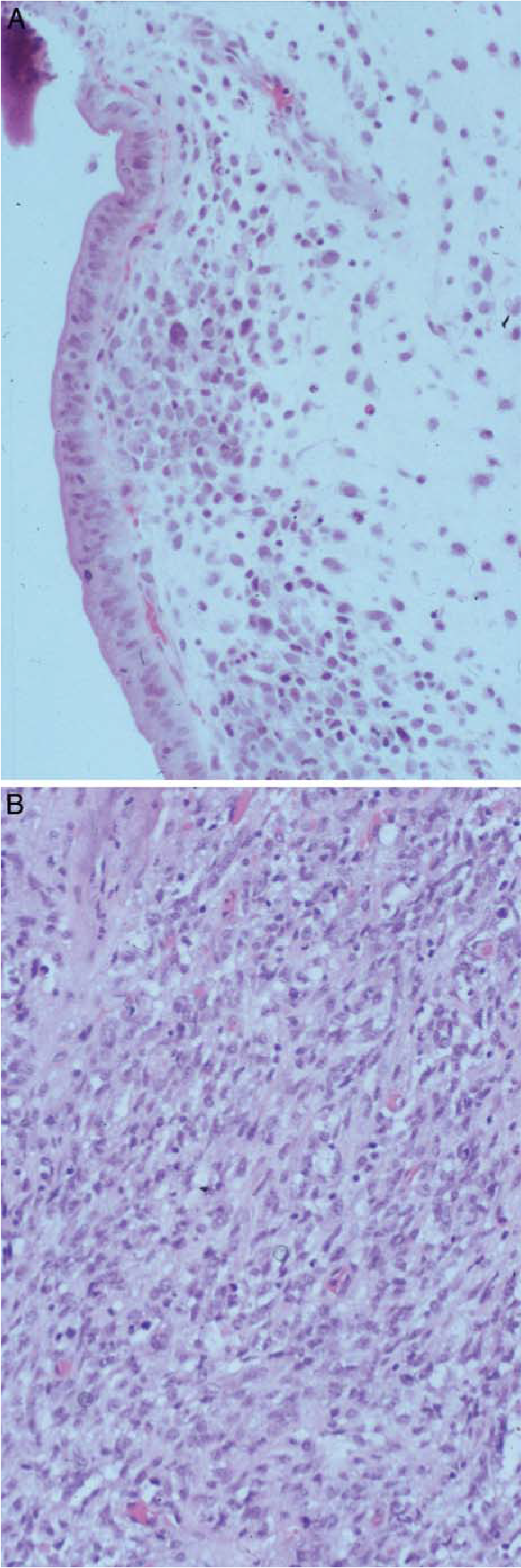
Biliary tract rhabdomyosarcoma (RMS) with (
In cases for which unstained slides or blocks were available (14 UESL, 12 biliary tract RMS), immunohistochemistry was performed as part of the COG review. Immunopositivity for both UESL and RMS has been variably reported using polyclonal desmin and MSA [3]. Fifty percent of the biliary tract RMS cases (n = 12) stained with either desmin or MSA (Table 2). Thirty-six percent of the UESL cases (n = 5) were desmin positive (Fig. 4A), but no UESL cases stained for MSA. Immunostains for myogenin (Fig. 4B) or MyoD1 were uniformly negative in all studied UESL cases; 75% of all studied RMS were positive for at least 1 of these intranuclear transcription factors (myogenin) (Table 2) (Fig. 4C), and 50% of RMS were positive for both (myogenin and MyoD1) (Table 2).
Immunohistochemical staining in RMS versus UESL
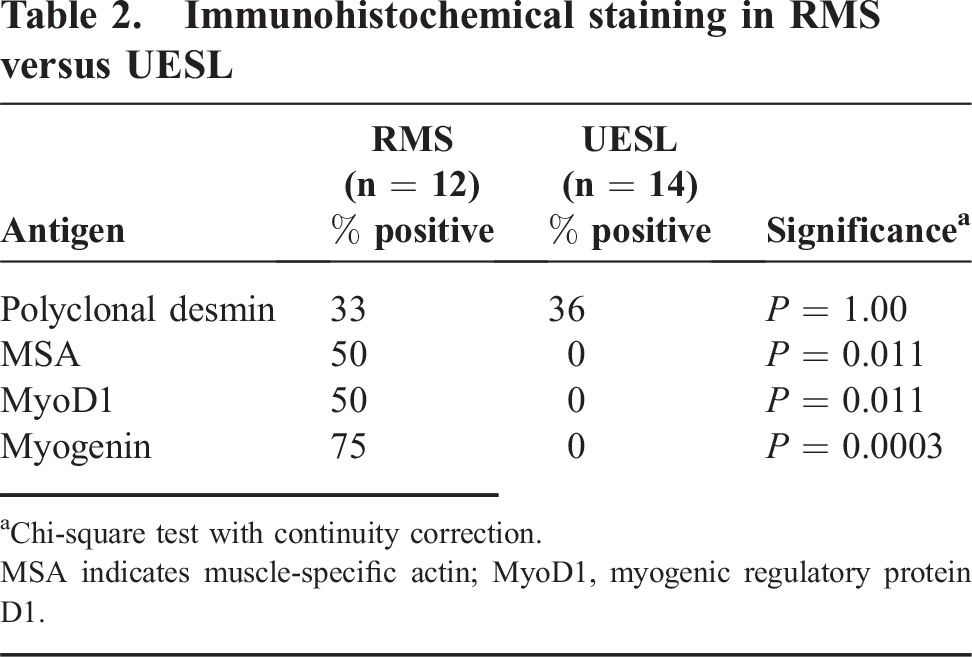
Chi-square test with continuity correction.
MSA indicates muscle-specific actin; MyoD1, myogenic regulatory protein D1.
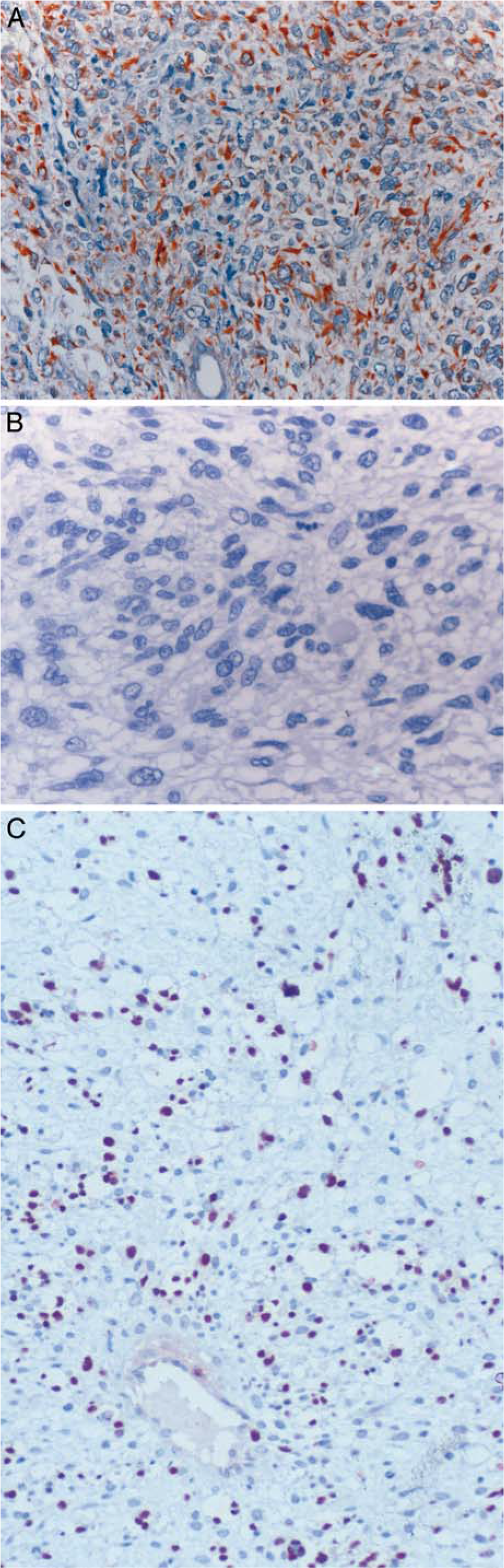
Immunohistochemical staining of UESL and RMS. (
Immunostaining results for polyclonal desmin, MSA, MyoD1, and myogenin in the selected RMS and UESL cases (Table 2) were analyzed statistically using the chi-square test with continuity correction (for small case numbers). All immunostains were scored as either positive or negative in each case. Polyclonal desmin did not distinguish UESL from RMS (P = 1.00). MyoD1 and MSA showed some statistical significance (P = 0.011) in distinguishing RMS (positive in 50% of cases) from UESL (negative); however, MSA was clearly found in UESL from other case series [11]. Neither MyoD1 nor myogenin has been reported as positive in UESL, and myogenin was highly significant (P = 0.0003) in distinguishing RMS (positive in 75% of cases) from UESL (all negative).
Electron micrographs of UESL (n = 3) available for review in our cases revealed that the eosinophilic globules were composed of lysosomes with various ingested materials. No cross striations (actin-myosin Z-band complexes) were identified.
DISCUSSION
The distinction between UESL and RMS of the biliary tract has been less clear in the literature of the last 10 to 15 years, as some authors have suggested a shared myogenic phenotype for the 2 malignancies on ultrastructural or immunohistochemical grounds [3,11]. In addition, the International Classification of Rhabdomyosarcoma describes an undifferentiated sarcoma [17] akin to alveolar RMS in behavior [18] and describes an “embryonal sarcoma” that is possibly related to embryonal RMS [17]. This confusion of terms and phenotypes has lead to an increasing enrollment of UESL cases into COG/IRS protocols over the last 3 decades (1 case between 1978 and 1982, 7 cases between 1993 and 1992, and 12 cases between 1993 and 2004). With this study, we hope to clarify the morphologic and phenotypic distinctions of RMS and UESL, which may have important initial treatment implications.
Rhabdomyosarcoma is a common sarcoma in children that arises from primitive mesenchyme and has been recognized as a clinical and pathologic entity for much longer than UESL [19]. Rhabdomyosarcoma often produces biliary tract obstruction with a hilar mass, and patients present with obstructive jaundice and abdominal pain [19,20]. Undifferentiated embryonal sarcoma of the liver, an uncommon malignancy, is found more frequently as a large mass in the right lobe of the liver, although it may also involve the left lobe. It is also occasionally mistaken for RMS histologically; however, many reports including ultrastructural and immunohistochemical studies have failed to definitively identify a specific histogenesis, only verifying its mesenchymal origin and various differentiated components [2,9,21–24]. Parham et al [11] and Aoyama et al [3], however, suggest that, at least on an ultrastructural and immunohistochemical level (with filamentous inclusions), RMS and UESL share a partial myogenic phenotype. In our study, 5 cases of UESL (36%) were immunopositive for polyclonal desmin, but all cases were negative for MSA, myogenin, and MyoD1.
Our study showed no ultrastructural evidence of a myogenic phenotype (actin-myosin Z-band complexes) in a limited number of UESL cases. These findings are similar to those previously reported [3,9,24], with the exception of Aoyama et al [3]; however, they did not stain their cases with MyoD1 or myogenin immunostains to confirm an RMS diagnosis. Forty percent of our UESL cases were originally diagnosed as RMS, while none of the biliary tract RMS cases were identified as UESL. Whereas both RMS and UESL are usually seen in children younger than 20 years [1], the majority of our UESL cases presented at an older age than did the RMS cases (median ages of 10.5 years versus 3.4 years, respectively).
Stocker and Ishak reported the largest series of UESL cases when they classified the neoplasm in 1978 [1]. The cases we reviewed demonstrated features described in the literature, including a proliferation of spindled cells with polygonal or round cells in a myxoid background. Foci of storiform cellular arrangement, occasional atypical mitoses, and anaplastic multinucleated giant cells are commonly present in UESL. Anaplasia, as defined elsewhere for RMS [14], is identical in UESL and includes cells with lobulated hyperchromic nuclei at least 3 times larger than those of the neighboring cells, with or without large atypical mitoses. Although anaplasia may be seen in embryonal RMS [25], it was not identified in our biliary tract RMS cases. All of our cases of UESL demonstrated PAS-positive, diastase-resistant, eosinophilic globules of variable size within the tumor cell cytoplasm and extracellular matrix. These globules were absent in the biliary tract RMS cases that we studied; however, they can be seen in a number of high-grade tumors, such as choroid plexus carcinoma, yolk sac and embryonal carcinomas, and rhabdoid tumors [26], and we have identified them in RMSs at other sites. At the edge of UESL, occasionally within the pseudocapsule, cystic structures (distended bile ducts) can be identified. Obvious rhabdomyoblasts and cross striations were absent from the UESL cases; however, a few cases demonstrated areas of spindle cell aggregation under this biliary epithelium (cambium layer) (Fig. 2A).
The cases of biliary tract RMS were of the botryoid variety, thus exhibiting scattered rhabdomyoblasts, virtually no giant cells, and a characteristic cambium layer under the biliary tract epithelium (Fig. 3). Features of alveolar RMS were not present in the biliary tract RMS cases.
Several reports have detailed the staining patterns of UESL with various special stains and immunohistochemical techniques [14]. Of note, tumor cells stain positive for cytokeratin, vimentin, S100, and occasionally desmin and actin [2,3,22,23]. Many of the markers, including the keratin as well as the desmin and actin, are reported as variably positive in both UESL [14,23] and RMS [27]. The eosinophilic globules of UESL have been shown to stain for alpha-1-antitrypsin as well [21].
We examined polyclonal desmin and MSA, in addition to myogenin and MyoD1, to distinguish UESL from RMS. Myogenin and MyoD1, intranuclear transcription factors expressed during myogenesis, are now the established immunohistochemical markers to confirm a diagnosis of RMS [13,14]. Myogenin was routinely detected by immunohistochemistry in the majority of biliary tract RMS (75%), and staining was uniformly absent in the UESL cases (P = 0.0003). MyoD1 is also a highly sensitive and specific marker for RMS, but it is highly prone to antigen decay [28]. Desmin is less specific [28] and variably positive in both UESL and biliary tract RMS cases. MSA has a very low level of sensitivity in RMS [28] and has been eliminated from our series of diagnostic markers; it is also reported as variably positive in UESL [11]. With the use of the antigen retrieval technique and timely immunostaining of tumor sections (within 1 week of cutting the paraffin blocks to avoid antigen decay) [28], we have demonstrated prospectively that MyoD1 and myogenin immunostains can exceed an immunopositivity of 97% for RMS, regardless of site [28], whereas UESLs remain consistently immunonegative for both these markers [14] when studied prospectively.
Additional studies of UESL include flow cytometry and cytogenetics. Leuschner et al [29] described the findings of a limited number of cases in which DNA flow cytometry was performed. Eighty percent of their UESL cases were diploid, while 20% were aneuploid. It was postulated that the diploid cases had a better prognosis with a longer survival time; however, Chou et al [30] described 2 cases of aneuploid UESL in which the children were alive at 1 year following diagnosis. Cytogenetic studies have found 3 cases with 19q13 abnormalities [6,31]. Iliszko et al [32] featured a case with complex chromosomal rearrangements that also included 19q13 involvement, suggesting that this locus may play a role in the pathogenesis and diagnosis of UESL, and linked it to mesenchymal hamartoma of the liver [31].
Historically, the prognosis of UESL is poor, perhaps because of the advanced stage of disease at the time of initial presentation [1,3]. Reports with larger case numbers describe a mortality rate of 81% to 86% and a median survival of <12 months [1,2]. Historically, adjuvant chemotherapy has had variable efficacy, and surgery is the mainstay of treatment; tumor resection appears to be necessary for cure [4,33–35]. Neoadjuvant chemotherapy may improve the chances of a gross total resection in some cases [5,36–39]. The literature on adjuvant chemotherapy is limited by the small numbers of patients treated, although responses have been documented following regimens that included cisplatin and doxorubicin [34,37,40,41]. Eleven of the 18 patients with UESL studied here were known to be alive at last contact (61%), but follow-up of the cohort was short (median follow-up of 8 months) (Table 1).
The estimated 5-year survival of biliary tract RMS is 66% [16] (Table 1), and survival is nearly universal for patients with nonmetastatic tumors. Treatment of these patients consists of surgery (usually biopsy only or subtotal resection) followed by chemotherapy and radiotherapy for most patients. With the relative success of this approach, it is suggested that patients with biliary tract RMS do not require aggressive approaches to achieve gross total tumor resection. Initial surgery may be limited to biopsy for diagnosis and staging, followed by multiagent chemotherapy and external beam radiotherapy [16].
UESL differs from biliary tract RMS, both clinically and pathologically. UESL tends to occur in older children, generally arises in the right lobe of the liver, and usually lacks the biliary obstruction seen with RMS. In addition to variable histopathologic differences between UESL and RMS, the consistent absence of myogenin or MyoD1 staining in UESL supports its distinction from RMS. These staining characteristics are extremely important when the sample size is limited, as in needle biopsy (either core biopsy or needle aspiration biopsy) [5,24]. In these cases the definitive diagnosis can be difficult, especially if sampling fails to demonstrate hyaline globules or anaplasia (both of which suggest the diagnosis of UESL). Cytogenetic analysis searching for complex chromosomal rearrangements of t(19q)(13.4) associated with UESL and mesenchymal hamartomas may also be a useful diagnostic adjunct in the future. These findings are not described in RMS [42], where loss of heterozygosity on chromosome 11p is the most consistent finding in the face of absence of consistent structural chromosomal abnormalities.
Historically, patients with UESL have been entered erroneously into COG protocols for RMS. The diagnostic distinction between UESL and biliary tract RMS is important clinically, as cure of UESL may require aggressive surgery (including liver transplantation), whereas aggressive surgery is unnecessary for cure of localized biliary tract RMS. Whereas adjuvant therapies may improve survival in UESL, the data in this paper (Table 1) are too limited to draw such conclusions. Enrollment in clinical trials that include systemic chemotherapy for all patients, such as the COG RMS studies, is appropriate for patients with biliary tract RMS. However, patients with UESL are better suited for clinical trials for non-RMS soft tissue sarcomas that include both surgery-only and surgery/chemotherapy treatment arms. Patients with UESL are eligible for a COG non-RMS soft tissue sarcoma clinical trial, scheduled to begin in early 2006. Further study will be needed to understand the underlying pathogenesis of these tumors and to clarify the role of adjuvant and neoadjuvant chemotherapy in UESL.
Footnotes
ACKNOWLEDGMENT
The assistance of James Anderson, PhD, in statistical analysis is greatly appreciated.