
Abstract
The vermiform appendix may react as part of a generalized viral infection, but histological documentation of appendiceal viral infection is rare. Adenovirus has been described in association with mesenteric adenitis and ileocecal intussusception, but to our knowledge there are no well-documented cases of adenoviral appendiceal infection presenting clinically as acute appendicitis without intussusception. We reviewed the pathology records of all appendectomies performed at our institution from 2001 through 2005. All incidental appendectomies and appendices with acute appendicitis or other pathological findings were excluded. We selected all negative appendices with lymphoid hyperplasia and reviewed hematoxylin and eosin–stained slides. Representative sections of each of these cases were immunostained with adenovirus antibody. Eight hundred seventy-seven appendectomies were performed during the study period. Of these, there were 94 cases that had a clinical diagnosis of acute appendicitis and that were pathologically negative. Sixty-three of the 94 cases had lymphoid hyperplasia and were stained for adenovirus. We identified 2 positive cases, which also showed epithelial proliferation and viral inclusions. One involved a 6-year-old male and the other involved a 5-year-old female, without intussusception. Adenovirus can infect the appendix and clinically mimic acute appendicitis without intussusception. We recommend that all negative appendices be evaluated for lymphoid hyperplasia and epithelial viral changes and possibly be stained with immunoperoxidase staining if indicated. We speculate that adenovirus may play a role in the pathogenesis of acute appendicitis.
INTRODUCTION
There are few reports indicating that the appendix can be involved in several generalized viral illnesses such as adenovirus, cytomegalovirus, Epstein-Barr virus, and measles [1–4]; however, morphological documentation of these infections is rare. Adenovirus has been demonstrated in cases of mesenteric adenitis and ileocecal intussusception by several methods, including classic morphologic changes, electron microscopy, DNA in situ hybridization, and immunoperoxidase staining [5–7], but to our knowledge adenoviral appendicitis without intussusception has not been reported.
To investigate whether adenovirus infection of the appendix can occur without intussusception, we retrospectively reviewed all appendices removed at our institution within a 4-year period.
METHODS
Internal review board approval was obtained for this study. Pathology records of all appendectomies performed at our institution from 2001 through 2005, inclusive, were reviewed. We identified cases with a clinical preoperative diagnosis of acute appendicitis that were pathologically negative for significant mucosal ulceration and transmural acute inflammation. In our department, grossly inflamed and incidental appendices are routinely sampled for microscopic examination, with representative sections including a longitudinal section of the tip and several cross sections from the mid and distal portion. All other appendices that are removed for clinical suspicion of acute appendicitis with no recognizable pathology on gross inspection or following microscopic evaluation are submitted entirely for histologic examination. All hematoxylin and eosin–stained sections in these cases were reviewed, and we selected those that showed lymphoid hyperplasia, which has been described as suggestive of viral infection [6]. Lymphoid hyperplasia was defined as crowded more-than-average-size follicles, with prominent reactive germinal centers associated with flattening of overlying epithelium, increased number of intraepithelial lymphocytes, and narrowing of the appendiceal lumen. Sections were stained with adenovirus antibody. Immunohistochemical studies were performed on 4- to 6-μm sections cut from formalin-fixed, paraffin-embedded blocks after antigen retrieval by incubation with trypsin for 10 minutes at 37 °C. The primary antibody used was anti-adenovirus (clone 10/11, catalog number MAB 8052, Chemicon, Temecula, CA, USA; dilution 1:50). According to the manufacturer, this antibody is specific for all 41 species of adenovirus. The avidin-biotin-complex method was used, and the chromogen was diaminobenzidine. Sections were counterstained with hematoxylin. Lung tissue with adenoviral pneumonia was used as a positive control. Strong nuclear staining with or without cytoplasmic staining was required for a positive result.
RESULTS
Eight hundred seventy-seven appendectomies were performed during the study period. Of these, there were 94 cases that involved a clinical preoperative diagnosis of acute appendicitis and that were pathologically negative for mucosal ulceration and acute inflammation. Lymphoid hyperplasia was noted in 63 of the 94 cases, and these were stained for adenovirus. Two out of 63 appendices showed positive staining.
Case 1
The first patient was a 6-year-old male who presented with abdominal pain, fever, and vomiting for 1 day. He had no diarrhea, constipation, urinary complaints, or any other upper respiratory tract symptoms. His temperature was 38.3 °C and his abdominal exam revealed tenderness in the right lower quadrant. Laboratory workup showed elevated white blood cell count 16.3 (normal: 4.1 to 11.3 K/CUMM), with increased neutrophils 11.9 (normal: 1.58 to 7.13 K/ CUMM). His pain worsened and the patient underwent laparoscopic evaluation approximately 72 hours after presentation. No intussusception was identified during surgery.
Case 2
This case involved a 5-year-old female who presented with complaints of abdominal pain, nausea, vomiting, decrease in activity and appetite, and fever. She had no cough, nasal congestion, or rash. Her temperature was 38.6 °C and her abdominal exam showed diffuse tenderness and some guarding. Her laboratory workup revealed a white blood cell count of 11.4 (normal: 4.1 to 11.3 K/CUMM). This patient underwent exploratory laparoscopy on the day of presentation. There was some intra-abdominal fluid and mild enlargement of mesenteric lymph nodes noted, but no intussusception was identified.
Pathologic examination
Both appendices showed significant lymphoid hyperplasia, but no mucosal ulceration or transmural acute inflammation was noted (Fig. 1). The mucosa revealed focal tufting and piling up of epithelial cells, with nuclear crowding and loss of cellular orientation (Fig. 2). The nuclei were enlarged and exhibited 2 types of intranuclear changes including eosinophilic nuclear inclusion bodies and “smudge cells” with homogeneous basophilic nuclei, as previously described by Yunis and colleagues [5]. There were shed epithelial cells in the appendiceal lumina, some of which showed the same inclusions. Case 1 showed focal neutrophilic infiltration of the surface epithelium without mucosal ulceration. Case 2 showed only a single focus of neutrophils infiltrating a reactive germinal center just under the surface epithelium. Neither case showed extension of acute inflammation into the muscularis propria. Immunoperoxidase stain for adenovirus showed scattered surface epithelial cells with strong nuclear positivity and focal cytoplasmic positivity (Fig. 3). None of the deeper glands, lymphoid cells, or histiocytes showed any positivity. Intranuclear inclusions were not seen in any of the immunoperoxidase-negative cases. No obvious inclusions were noted in the appendices lacking lymphoid hyperplasia or in the acute appendicitis cases.
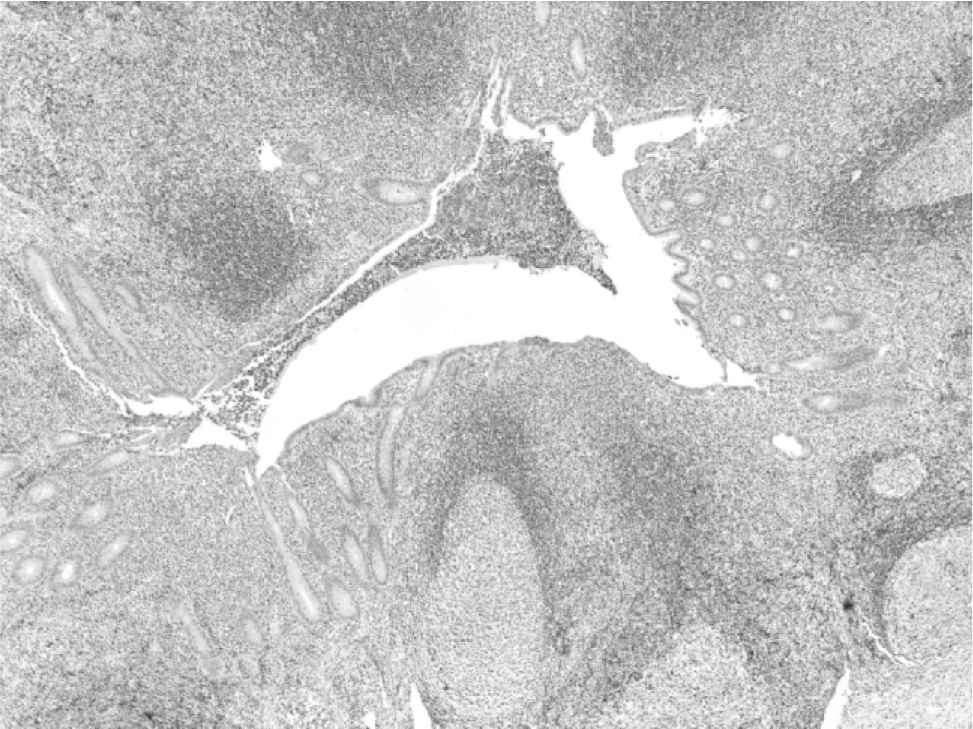
The appendiceal surface epithelium is stretched over hypertrophic lymphoid follicles, causing luminal narrowing.
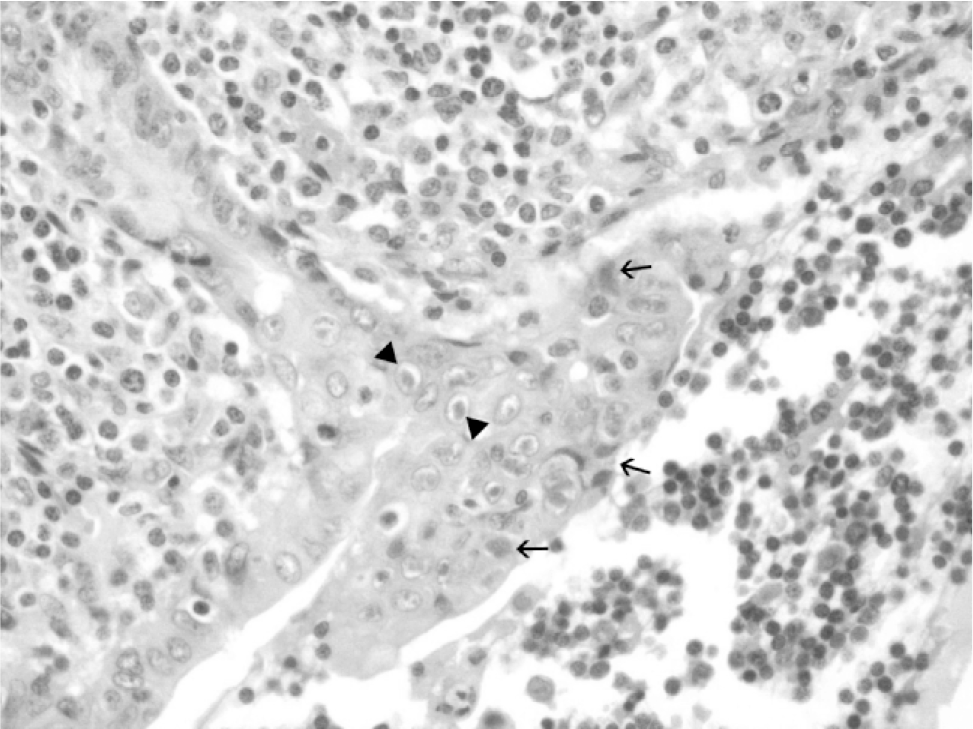
Tufting and piling up of epithelial cells with nuclear crowding and loss of cellular orientation. Two types of nuclear changes are seen, including eosinophilic intranuclear inclusions (between arrowheads) and “smudge cells” (arrows).
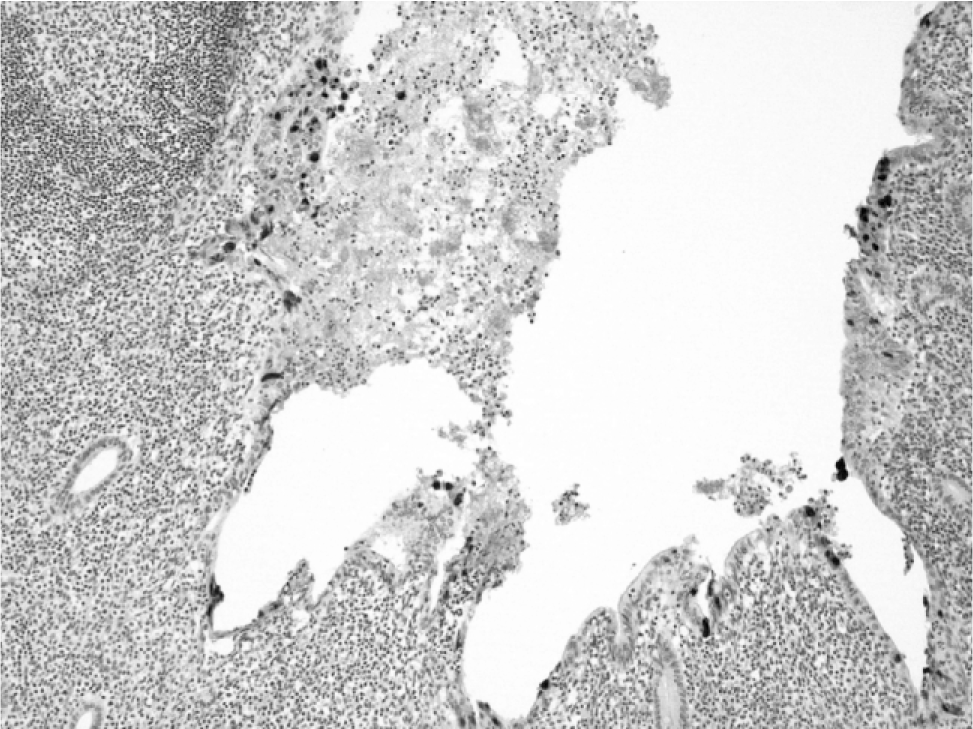
Immunoperoxidase stain for adenovirus shows scattered surface epithelial cells with strong nuclear and associated cytoplasmic positivity.
DISCUSSION
Existing research on viral involvement of the appendix can be broadly divided into 3 categories: (1) investigation of a viral role in the etiology of acute appendicitis, (2) demonstration of appendiceal involvement in specific viral infections, and (3) demonstration of a viral role in intussusception and mesenteric adenitis. At present there is very little morphological evidence of viral appendicitis presenting clinically as acute appendicitis without either systemic viral disease or intussusception.
The etiology of acute appendicitis remains enigmatic despite its frequency [8,9]. Suggestion of a viral role in acute appendicitis comes from epidemiologic as well as serologic and immunofluorescence studies. Barker [10] analyzed time trends in mortality rates for appendicitis in England and Wales and observed that appendicitis became frequent coincident with diminished childhood infections secondary to improved living conditions and sanitation. He hypothesized that the decreased incidence of childhood infections may have changed the populations' patterns of immunity and response to enteric pathogens later in life, allowing viral infection to incite acute appendicitis. Other research has shown clustering and outbreaks among appendicitis cases, supporting an infectious etiology [11]. Tobe [12] found raised antibody titers against Coxsackie virus before appendectomy with reduced titer values in paired sera checked 3 or 12 weeks after appendectomy, compared to results from a control group of patients. In addition, Tobe showed more immunofluorescence positivity for Coxsackie B virus and adenovirus in the cytoplasm of epithelial histiocytes and intranodal reticulum cells in patients with abnormal appendices ranging from lymphoid hyperplasia to gangrenous appendicitis than was found in a control group. For those authors who suggest a viral role in acute appendicitis, the proposed mechanisms of viral damage include ischemic luminal obstruction secondary to florid reactive lymphoid hyperplasia, as suggested by Bohrod in 1946 [13], and direct damage of the surface epithelium secondary to infection [14].
There are several reports documenting appendiceal involvement in systemic viral infection. Lopez-Navidad and colleagues [3] described a 17-year-old immunocompetent patient with a perforated appendix and periappendiceal abscess 3 weeks following a documented episode of infectious mononucleosis. Lin and colleagues [1] and, more recently, Neumayer and colleagues [2] reported cases of cytomegalovirus-associated appendicitis in patients with acquired immunodeficiency syndrome. Paik and colleagues [4] described 2 cases of appendicitis in patients with measles, 1 occurring during the prodromal phase and 1 occurring during the full-blown stage, and in both of these cases classic Warthin-Finkeldey-type giant cells were identified.
Adenovirus has been linked to mesenteric adenitis as well as to ileocecal intussusception [5,6,15–17]. Bell and Steyn [15] were able to culture adenovirus from 10 out of 17 patients with intussusception and from 10 out of 31 cases with mesenteric adenitis compared to only 5 out of 50 control cases, including 38 confirmed histologically with acute appendicitis. Yunis and colleagues [5] performed a histological and ultrastructural study on 682 appendices, of which 30 were from patients with ileocecal intussusception. They found that 11 of these 30 cases contained viral inclusions by light microscopy as well as viral particles on electron microscopy, consistent with adenovirus. They described 2 types of intranuclear changes on light microscopy, similar to our 2 cases. Porter and colleagues [6] found viral inclusions as described above in 19 of 39 appendices removed at the time of surgical reduction of intussusception and in 0 of 15 incidental appendectomies using in situ hybridization. Twelve out of 15 inclusion-positive cases that were available for staining were confirmed to be positive for adenovirus, while none of the inclusion-negative intussusception cases or controls was positive.
To our knowledge this is the 1st report of adenoviral infection of the appendix presenting clinically as acute appendicitis without intussusception. The histological findings in our cases were similar to those described in intussusception. We speculate that there is a spectrum of effects of adenoviral infection on the appendix that could lead to variable clinical presentations, including enteritis, intussusception, viral appendicitis, as demonstrated in our study, and possibly full-blown acute appendicitis. The presentation likely depends on various host and pathogen factors and would be a fruitful area of further research.
Our study confirms that adenovirus can infect the appendix and present with signs and symptoms of acute appendicitis without intussusception. We hypothesize that adenovirus may play a pathogenetic role in some cases of acute appendicitis; however, future studies to evaluate the role of viral infection in histologically confirmed acute appendicitis are needed to answer that question.
We recommend that all negative appendices be evaluated carefully for lymphoid hyperplasia and epithelial viral changes and possibly be stained with immunoperoxidase staining, if indicated.