
Abstract

To the Editor,
A 6-day-old female infant was born weighing 3.3 kg at 35 and 5/7 weeks by elective cesarean for breech presentation to a 24-year-old gravida 1, para 1 mother with a history of gestational diabetes. A 31-week ultrasonogram revealed enlarged cystic kidneys in the fetus and oligohydramnios. It was presumed that the fetus would develop severe pulmonary hypoplasia; her parents decided to continue the pregnancy but requested that comfort measures only be provided at birth. However, the neonate demonstrated spontaneous respiratory effort at birth, with APGAR scores of 8 and 9 at 1 and 5 minutes, respectively. There was some increased work of breathing, and the patient required oxygen through a nasal cannula. Mild hyponatremia (sodium 134 mMol/L) and hypertension were documented. The patient was anuric, with blood urea nitrogen of 20 mg/dL and creatinine of 1.7 mg/dL. There is no family history of renal disease, and both parents underwent renal ultrasonograms, with no evidence of polycystic kidney disease. With a presumptive diagnosis of bilateral polycystic kidney disease, the infant underwent bilateral nephrectomy and was placed on hemodialysis, awaiting renal transplantation.
We received both kidneys, with a weight of 214 g (left) and 217 g (right), for an expected weight of 14 g each. The kidneys measured 10.5 × 6.5 × 5.5 cm (left), and 10.0 × 6.0 × 5.5 cm (right). Both kidneys featured a reniform shape with fetal lobations and a smooth translucent capsule. Small, subcapsular cysts were appreciated. The cut sections revealed tan, polycystic, striated renal parenchyma. The corticomedullary demarcation was completely obliterated and replaced by uniform, thin, linear, and radially oriented cystic structures. There were no grossly identified masses (Fig. 1A).
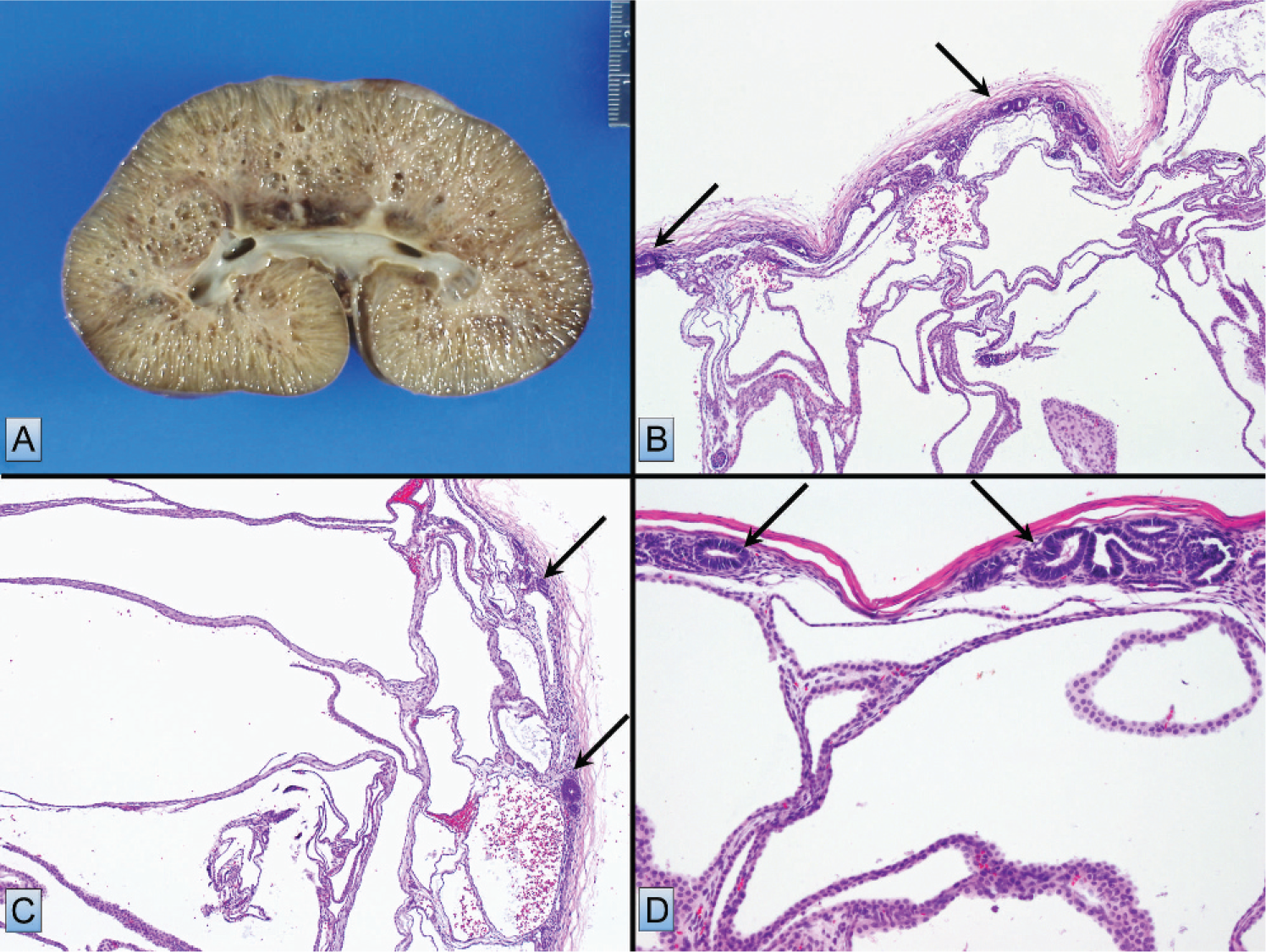
The histologic sections of both kidneys confirmed the numerous radially arranged cystic spaces lined by uniform cuboidal epithelium. There were occasional nephron units with normal-appearing glomeruli and tubules trapped between the cysts. Of note, both kidneys exhibited multifocal, small, immature nephrogenic elements (nephrogenic rests), located peripherally in a perilobar, subcapsular distribution (Fig. 1B,C,D).
These findings are characteristic of autosomal recessive polycystic kidney disease, grossly and histologically [1–6]. However, we are puzzled by the small, multifocal nephrogenic rests present. We wonder whether these could be explained by a discontinuous nephrogenic zone, but also note that the gestational age of our patient was nearly term and that mature renal cortex was identified elsewhere in the specimen. We hypothesize that the underlying autosomal recessive polycystic kidney disease may have arrested growth and development of the nephrogenic system and that we are seeing the result of delayed nephrogenesis. In this case, both kidneys have been removed, so there is no concern for potential risk of developing malignancy in the future. To the best of our knowledge, this finding has not been remarked upon in the literature, and we are most interested in knowing whether others have also come across this observation.