
Abstract
There are conflicting reports regarding the relative frequency of benign and malignant epithelial salivary gland tumors in children. There are only a few reports of the cytogenetic abnormalities in the pleomorphic adenomas (PA) that arise in children, and even less information regarding the pleomorphic adenoma gene 1 (PLAG1) and high motility group A2 (HMGA2) histochemical staining in PAs, or their correlation with histologic types (stromal vs epithelial predominance). A retrospective 14 year review of epithelial salivary gland tumors encountered at a children's hospital identified 13 tumors: 12 PAs and 1 acinic cell carcinoma (ACC). No mucoepidermoid carcinomas were identified. Tumors arose in the parotid (7) and other sites (2 submandibular, 4 minor). Ten PAs in our cohort had cytogenetic studies. Four were normal, 5 involved 8q12, and 1 involved 12q13. Immunohistochemistry identified an additional 2 PAs with PLAG1 staining, and 5 additional PAs with HMGA2 staining. One tumor with ins(18;8)(q21.1;q12q22.2) had no PLAG1 staining, but stained with HMGA2. This ins(18;8) may not have involved the PLAG1 gene. There was no demonstrable correlation of 8q12/PLAG1 staining or 12q13/HMGA2 staining with histologic type. Thus we found abnormalities in either 8q12/PLAG1 staining or 12q13/HMGA2 staining in all PAs. The HMGA2 staining in 50% of PAs suggests that it may be more frequently involved in PAs than previously thought based on cytogenetic studies, at least in children.
Keywords
INTRODUCTION
Less than 5% of epithelial salivary glands occur in the 1st 2 decades of life [1–3]. Of these, most occur in the 2nd decade. In children, reports differ regarding the proportion of malignant to benign lesions. Some, including several large studies, report a predominance of benign tumors [2,4–10] approaching the 85%–90% [11] frequency encountered in adults. Others report a predominance of malignant tumors [12–15], and still others report an equal occurrence of malignant and benign tumors [1,3,16–20]. Consistently, the most frequent benign epithelial tumor is the pleomorphic adenoma (PA), and the most common malignant epithelial tumor is the mucoepidermoid carcinoma.
Of the benign tumors, PAs have been well studied in adults. The PA is associated with a translocation involving 8q12 in 25%–39% of the tumors, which is the site of the pleomorphic adenoma gene 1 (PLAG1). Eleven to twenty-three percent of the tumors have sporadic clonal changes, and 8%–13% have rearrangements of 12q13-15, the site of the high-mobility group protein 2A (HMGA2) [21,22]. Correlations of the karyotypic findings with the amount of stroma have been made, with stromal predominance (~80% of tumor mass) reportedly being more frequent in those tumors with normal karyotypes or 12q13 rearrangements and the 8q12 abnormalities associated more frequently with epithelial predominance, although there is considerable overlap [22].
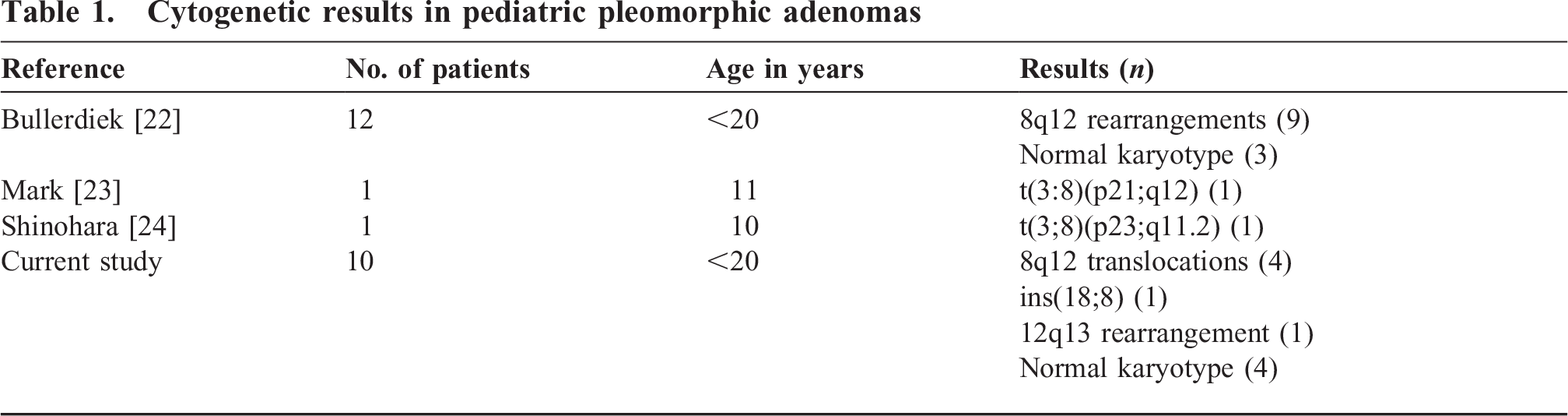
At present, reported data on the spectrum of cytogenetic abnormalities in pediatric PAs are limited (Table 1) [23–25]. There is no systematic evaluation of the correlation of immunohistochemical PLAG1 and HMGA2 staining in PAs with cytogenetic results or with histology in children.
Cytogenetic results in pediatric pleomorphic adenomas
We review our experience with childhood epithelial salivary gland tumors to identify the spectrum of histologic types in our population, sites of occurrence, outcomes, and spectrum of cytogenetic abnormalities. We utilize immunohistochemical stains against PLAG1 and HMGA2 to assess these stains' correlation with the cytogenetic results and the underlying histology.
MATERIAL AND METHODS
After Institutional Review Board approval, we retrospectively reviewed the pathology records between 1994 and 2008 at a children's hospital to identify all epithelial salivary gland tumors in children less than 19 years of age at 1st diagnosis. Slides of the tumors were reviewed to confirm the diagnosis, confirm the status of the margins, and classify the tumors as predominately epithelial (<50% stroma) or predominately stroma (>50% stroma). Immunoperoxidase stains using antibodies against PLAG1 (Novus Biologicals, Littleton, CO, USA) were performed on all PAs on formalin-fixed, paraffin-embedded tissue. In 7 of the 13 tumors, the entire tumor was fixed in B5. Despite repeated attempts, we could not get the PLAG1 antibody to react in B5-fixed tissue. Positive controls were lipoblastomas and PAs with documented 8q12 translocations. Positive staining was defined as nuclear staining of the myoepithelial cells and of the cells in the mesenchyme. The inner ductular epithelial cells and normal salivary gland do not stain [25]. High-mobility group protein (Biocheck, Foster City, CA, USA) immunoperoxidase stains were performed on all B5- or formalin-fixed, paraffin-embedded tumors. The positive control was a PA with a 12q13 translocation. Nuclear staining of ductular, epithelial, or cells within the mesenchyme was interpreted as positive [26]. Cytogenetic results were also reviewed; all cytogenetic results were initiated at the original time of surgery. Clinical records were reviewed for demographics, recurrence, and associated abnormalities. The Louisiana Tumor Registry was accessed to supplement the clinical records to determine if any child had a previous diagnosis of malignancy, if any malignancy subsequently developed in these individuals, or if any malignancy recurred.
RESULTS
Tumors from 13 children were identified (Table 2). Age at diagnosis ranged from 10 to 17 years. There was 1 acinic cell carcinoma and 12 PAs (Fig. 1).
Epithelial salivary gland tumor characteristics in 13 children
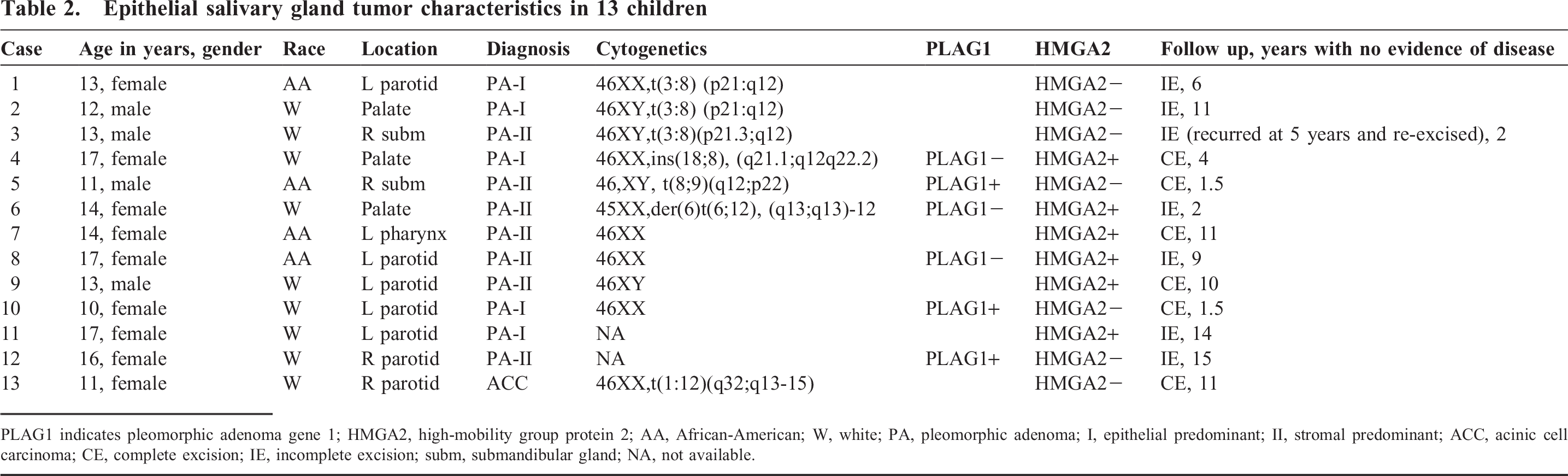
PLAGI indicates pleomorphic adenoma gene 1; hmga2, high-mobility group protein 2; AA, African-American; W, white; PA, pleomorphic adenoma; I, epithelial predominant; II, stromal predominant; ACC, acinic cell carcinoma; CE, complete excision; IE, incomplete excision; subm, submandibular gland; NA, not available.
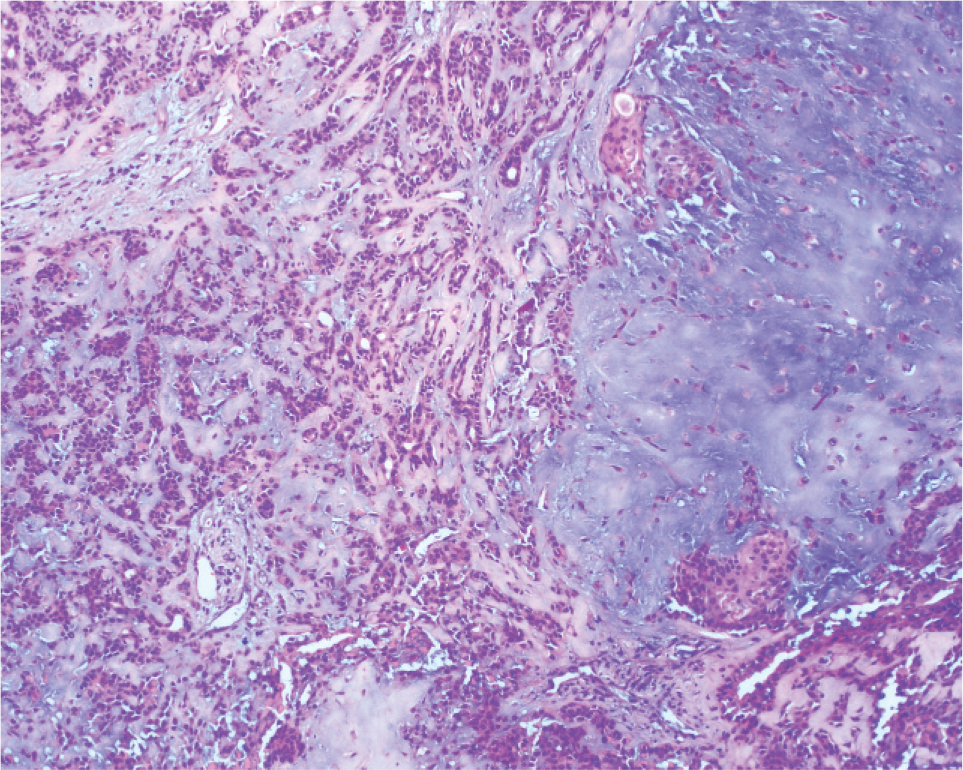
Pleomorphic adenoma (hematoxylin and eosin, ×100). A color version of this figure is available online.
Of the 12 PAs, the average age was 13.9 years (range 10-17 years). Eight were female, and 4 were male. Eight were white, and 4 were African-American. Six were from the parotid gland, 2 were from the submandibular gland, and 4 were from minor salivary glands (3 palate, 1 pharynx [parapharyngeal]). Five were completely excised, and 7 had at least microscopic residual disease in the surgical margin. Average follow up was 7.7 years and ranged from 18 months to 15 years. There was 1 local recurrence at 5 years (submandibular gland), which was re-excised, and no subsequent tumor had recurred after 2 years of follow up. None degenerated into a malignancy. None of these children had received previous radiation treatment.
One 13-year-old African-American girl had Klippel-Trenaunay-Weber syndrome with left hemifacial hypertrophy (tumor involved left parotid, case 1). She had the common t(3:8) abnormality. All of the remaining children were normal. Cytogenetic studies were available in 10 children with PAs, all obtained from the primary surgical material. Four were normal. Five involved 8q12,− 4 translocations (3 involving t[3;8], another involving t[8;9]) and 1 insertion. The 6th abnormal cytogenetic study involved translocation of 12q13-15. No other clonal abnormalities were identified.
All PAs had tissue preserved in B5, only 6 PAs had formalin-fixed tissue for evaluation. In the 6 PAs with formalin-fixed tissue, 3 stained positively for PLAG1. In the positive cases, the nuclei of the myoepithelial cells, clusters of epithelial cells, and cells embedded within the stroma, often individual, stained. The well-differentiated ductular epithelial cells present in the tumor did not show nuclear staining. The cytoplasm did not stain (Fig. 2). The cells in the surrounding normal salivary gland did not stain with PLAG1. This conforms to the pattern previously described [25]. The tumors staining positive for PLAG1 included 1 with a translocation involving 8q12 (case 5), 1 with normal cytogenetics (case 10), and 1 without cytogenetic studies (case 12). The PLAG1 stain was negative in 3, 1 with normal cytogenetics (case 8), 1 with ins(18;8) (case 4), and 1 with t(6;12) (case 6). All 3 of these negative PLAG1 tumors stained with anti-HMGA2 (vida infra). In summary, the PLAG1 stain disclosed 2 tumors with PLAG1 abnormalities (cases 10 and 12) that lacked cytogenetic abnormalities in the region of the PLAG1 gene. One of 2 PLAG1-positive tumors with cytogenetics studies had a documented translocation involving 8q. The lack of PLAGI staining brought into question the relationship of the ins(18;8) to PLAGI activation.
Pleomorphic adenoma gene 1 (PLAGI) stained the nuclei in the myoepithelial cells and the individual cells within the stroma. Note the lack of nuclear staining in the ductular cells (anti-plag1, ×400). A color version of this figure is available online.
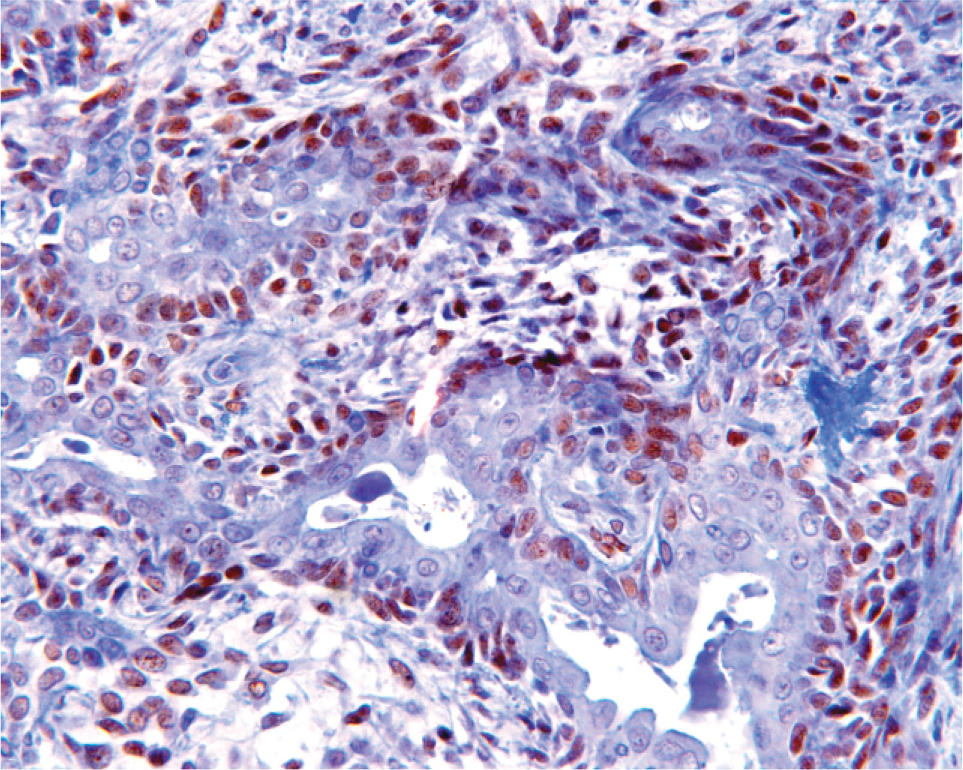
Staining with antibodies against HMGA2 was positive in 6 tumors (Fig. 3). In the positive tumors, the nuclei of the ducts, epithelial islands, and cells within the stroma stained positive. Often, the cytoplasm also stained, but in general it was less intense than the nuclear staining. In the surrounding normal salivary gland, the duct cytoplasm stained positive, and the acini oftentimes had a faint blush, but these cells lacked nuclear staining. Of these 6 positive tumors, 1 had the t(6;12) (case 6), 3 had normal karyotypes (cases 7–9), 1 had no cytogenetic studies performed (case 11), and the karyotype in 1 (case 4) showed an in(8;18) and no PLAGI staining. Three of 5 HMGA2-positive tumors had normal chromosomes, 1 of 5 had a demonstrable t(12q13), and 1 was associated with a PLAG1-negative ins(18;8).
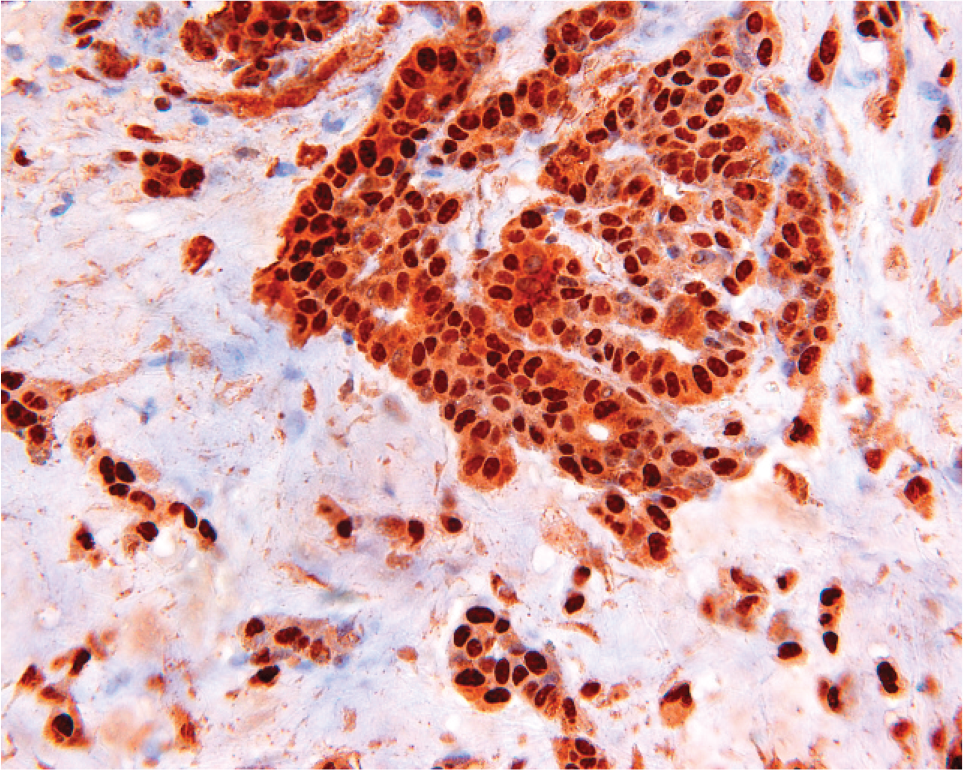
High-mobility group protein 2A (HMGA2) stained the nuclei of the ductular cells, myoepithelial cells, islands of epithelial cells, and cells within the stroma. Some cytoplasmic staining is also present (anti-HMGA2, ×400). A color version of this figure is available online.
There was no correlation between cytogenetics/ immunohistochemical phenotype and histologic type of PA. There were 5 epithelial predominant tumors (3 associated with the 8q12/PLAG1-positive group of tumors, 2 with the 12q13/HMGA2-positive tumors). The 7 stromal-predominant tumors included 3 8q12/PLAG1-positive and 4 12q13/HMGA2-positive tumors.
There was no difference in the distribution of tumors between African-American and white children, with respect to site, karyotypic results, PLAG1, or HMGA2 staining.
The only malignancy identified was an acinic cell carcinoma of the parotid. It was completely excised, and there has been no recurrence after 11 years of follow up. The karyotype demonstrated 46XX,t(1:12)(q32;q15). This acinic cell carcinoma did not show staining with HMGA2.
DISCUSSION
Our experience encountering 12 benign and 1 malignant epithelial salivary gland tumor agrees with those who encounter a predominance of benign lesions [2,4–10]. That there is such a wide variation in the reports of the frequency of benign vs malignant tumors in the literature suggests this may reflect differing referral patterns of the host institutions or genuine regional differences in tumor biology.
Most (80%–90%) [9,20] salivary gland tumors in childhood occur in the parotid, with 11% and 1% occurring in the submandibular and minor salivary glands, respectively [20]. Our distribution of tumors differs in several ways from that reported in the literature. Our parotid tumors account for only 7 of 13 (54%) epithelial salivary gland tumors, with minor salivary gland tumors composing 4 of the 13 (31%) sites. Another difference is a lack of mucoepidermoid carcinomas in this study. We also did not identify any in our hospital tumor registry (established 1986). The small number of patients in our study limits definitive statements regarding this distribution.
In mixed studies of adults and children, the male:female ratio is 1:2 [11]. This ratio was preserved in our study population.
To date, PAs have not been associated with any specific genetic syndromes. Klippel-Trenaunay-Weber syndrome (case 1) is a triad of varicose veins, cutaneous capillary malformation, and hypertrophy of bone and soft tissue. There is 1 report of a translocation involving 8q22.3 in this syndrome [27]. Because this location is some distance from the translocation involving 8q12, this is probably a coexistent condition rather than etiologically related. Other studies have implicated molecular abnormalities of vasculogenesis as the basis of Klippel-Trenaunay-Weber syndrome [28]. Because the PLAG1 gene activates insulin-like growth factor 2 [29] and our case (case 1) had a t(3;8), a relationship between PLAG1 and Klippel-Trenaunay-Weber syndrome is not readily evident.
In adult or mixed adult/children studies, it is reported that approximately 50%–70% of PAs will demonstrate karyotypic abnormalities [21,22]. The most common (25%–40%) involves the region of the PLAG1 gene at the 8q12 locus. Abnormalities of 8q12 reportedly tend to occur in slightly younger patients (average age 39 years) than in patients with 12q13-15 or normal tumor karyotypes [22]. In our study, 50% of the tumors with cytogenetic data involved the 8q12 region, although the tumor with the ins(18;8) may not have involved PLAG1. This is in keeping with the reported younger averaged aged patients with karyotypic 8q12 abnormalities.
In those 30%–50% of PAs with normal tumor cytogenetic studies, 60% may demonstrate cryptic translocations leading to PLAG1 upregulation [30]. In our small study, only 1 of 4 with a normal karyotype had demonstrable PLAG1 staining by immunohistochemical detection, whereas the remaining 3 of 4 PAs with normal karyotyes demonstrated HMGA2 staining.
The 60% prevalence of identifiable karyotypic abnormalities in our childhood PAs conforms to what has been described in adult or mixed adult/children studies. Based on the cytogenetic findings alone, we did not encounter sporadic clonal abnormalities. Perhaps these sporadic abnormalities take many years longer to evolve into tumors than the 8q12 and 12q13-15 abnormalities, which may have a selective growth advantage. Alternatively, the sporadic abnormalities may be coincidental, not necessarily playing a role in tumor genesis, but arising in the tumors as a result of increased age.
With the use of immunohistochemistry, we were able to demonstrate PLAG1 staining in an additional 2 PAs without 8q12 karyotypic abnormalities in our cohort, 1 with a normal karyotype and 1 in which no cytogenetic studies were performed. The lack of PLAG1 staining in case 4, with the ins(18;8), suggests that the PLAG1 gene was not upregulated in this tumor. In another study, PLAG1 expression by northern blot was found in 13 of 17 PAs with normal karyotypes, higher than our 1 in 4 [31]. In that study, 5 of 10 tumors with the 12q13 abnormality also demonstrated increased PLAG1 expression. In our 1 case with the 12q13 abnormality, the PLAG1 was negative, and in no other HMGA2-expressing tumor was there also PLAG1 staining demonstrated.
We had 6 tumors with abnormal nuclear staining with HMGA2. One was associated with an abnormal t(12q13-15) and another 3 with normal cytogenetics. There was 1 in which no cytogenetic studies were performed, and 1 had an abnormal ins(18;8) karyotype. The lack of demonstrable PLAG1 staining with HMGA2 in case 4 with the ins(18;8)(q21.1;q12q22.2) suggests that even though the insertion is near the PLAG1 gene, it may not involve the gene. Instead, the HMGA2 gene was expressed. There is a precedent for this, because another study had an ins(8;12)(q12-13;q14q15) with no increased expression of PLAG1 by northern blot [32]. Thus, the ins(18;8) may represent a sporadic clonal event.
In 6 tumors, there was formalin-fixed tissue available to perform both PLAG1 and HMGA2 immunohistochemistry. These tumor were positive for PLAG1 (3 tumors) or HMGA2 (3 tumors), but none were positive for both. Although we cannot confirm that PLAG1 stained in 3 of our t(3;8) tumors, these were all negative for HMGA2. Caution still needs to be taken in that there are instances in which the breakpoint is near the 8q12 in PAs, but PLAG1 staining is negative [32–34].
The oncogene PLAG1 is a transcription factor normally expressed only in fetal tissues [29]. Upregulation by promoter swapping results in stimulation of insulin-like growth factor 2, which in turn is involved in many different tumors. One of the more common translocation partners is 3p21, where the gene cadherin-associated CTNNB1 is located. This gene, which encodes beta catenin, is ubiquitously expressed, so the translocation allows the active promoter portion of CTNNB1 to drive PLAG1 expression. Another common translocation, not seen in our cohort, involves the leukemia inhibitory factor receptor, associated with the t(5;8)(p13;q12) [35]. Our translocation involving 9p22 also seems to be a recurring translocation, because it has previously been reported in at least 2 PAs [23]. It may involve an as yet unidentified promoter. The insertion involving 18q may be novel and may not affect the PLAG1 expression.
In tumors with normal karyotypes, cryptic translocations involving the region of PLAG1 have been found. These have involved the SII/TCEA1 gene (centromerically located on 8) [31] and CHCHD4 (telomerically located) [36]. The cryptic rearrangement of CHCHD4 has been described also in novel translocations (t[6;8], t[8;15]) [23,36].
From the literature, identified recurrent translocated genetic partners for HMGA2 include 3p14, the site of the FHIT (fragile histidine triad) gene, and 9p23, the site of NFIB (nuclear protein involved in transcriptional regulation). Fusion leads to deregulation of HMGA2 expression [21]. An abnormality involving 6q12 has previously been described as in our study [23]. This may be a recurring abnormality involving another as of yet undescribed promoter gene.
With the addition of immunohistochemical studies, we were able to identify abnormalities in all of our 12 pediatric PAs. These included an abnormal 8q12 or abnormal positive staining with PLAG1 (7 tumors, including case 4) and abnormal 12q13 or abnormal positive staining with HMGA2 (6 tumors). The abnormal staining demonstrated by immunohistochemistry with normal cytogenetics may represent either normal stromal overgrowth in the fibroblast cultures or cryptic translocations. The more frequent finding of abnormal staining with HMGA2 with normal chromosomes suggests that HMGA2 may be more frequently involved in PAs than was previously thought, at least in children. One source may be cryptic translocations that involve the HMGA2 locus.
The significance of the t(1;12) in our acinic cell carcinoma is presently unknown, because no consistent karyotypic abnormality has been described. This translocation does not appear to involve HMGA2, because our HMGA2 stain was negative.
In conclusion, most (12 of 13) of our tumors were benign PAs, with only 1 malignant tumor, the acinic cell carcinoma. Mucoepidermoid carcinomas were absent from our series. Only 1 recurred, although 7 of 13 were incompletely excised. Tumors were near evenly split between the parotid (7) and other sites (6), unlike other series in children, in which 90% arose in the parotid. Most (12 of 13) children had no underlying abnormality. Karyotypic abnormalities or abnormal staining with PLAG1 or HMGA2 were present in all of our PAs, with only 1 overlap involving an ins(18:8). Abnormalities of 12q13 and/or staining with HMGA2 were demonstrated in 50% of the PAs, suggesting that HMGA2, at least in children, is more frequently involved than previously recognized.