
Abstract
Lymphadenoma of the salivary gland is a rare benign tumor with only 11 reported cases in the English language literature, most of which have occurred in adults. We report a case of a lymphadenoma occurring in the parotid gland of a 15-year-old girl. The tumor was composed of variably sized cystic cavities within abundant reactive lymphoid tissue. The cystic spaces were filled with eosinophilic secretions with occasional histiocytes. Many of these features were also apparent on cytologic preparations. The cysts were lined by epithelium lacking atypia and showed luminal and abluminal differentiation both by immunohistochemistry and by electron microscopy. Tumor cells were not cycling as determined by MIB1 immunostaining, and the tumor karyotype was normal. This is only the second case to be reported in the pediatric age group. Ultrastructural features and karyotype analysis are reported for the first time. Although this tumor is rarely encountered by pediatric pathologists, awareness of its existence is important to distinguish it from possible malignant mimics, such as lymphoepithelial carcinoma and metastatic mucoepidermoid carcinoma in a lymph node.
INTRODUCTION
Lymphadenoma is a rare salivary gland tumor characterized by epithelial elements intimately associated with a prominent lymphoid component. It is distinct from other salivary gland epithelial neoplasms with a lymphocytic component, such as Warthin tumor (papillary cystadenoma lymphomatosum) and sebaceous lymphadenoma, in that lymphadenoma lacks both oncocytic cells covering papillary formations and sebaceous cells [1,2]. The term was first used in 1994 [3]. To date there are only 11 published cases in the English language literature [3–11], with only a single case occurring in the pediatric age group [9]. We report a second pediatric case of this unusual tumor, occurring in the parotid gland of a 15-year-old girl. This is the first report to detail the electron microscopic and cytogenetic findings of this tumor.
CASE REPORT
A 15-year-old girl presented at the Hospital for Sick Children, Toronto, Ontario, Canada with a 6-month history of a nontender neck mass in the right parotid region. The patient was otherwise well. There was no family history of note. The neck mass was situated in the tail of the right parotid gland and was completely excised with preservation of the facial nerve. A right jugulodigastric lymphadenectomy was also performed. The surgical procedure and the postoperative recovery were routine. There has been no recurrence of disease to date (8 months after surgery).
RESULTS
Macroscopic Features
The tumor was a well-circumscribed, ovoid soft-tissue mass measuring 4.5 × 3.2 × 2.7 cm with a smooth external surface. Cut sections showed a variegated pale tan appearance with small, variably sized cystic foci containing mucoid material (Fig. 1). The mass had a peripheral rim of brown tissue reminiscent of lymph node tissue. The separate lymphadenectomy specimen contained multiple lymph nodes, the largest of which measured 2.3 cm in greatest dimension, and these nodes were not involved by the tumor.

Macroscopic appearance of the tumor showing variably sized cystic spaces containing tenacious mucoid secretions. A brown rim of lymphoid type tissue is present.
Cytologic Features
Smears of the tumor specimen were highly cellular. A dense reactive lymphoid component was present (Fig. 2A) consisting of small reactive lymphocytes, germinal center cells, and plasma cells, features similar to those of benign reactive lymph nodes. The epithelial component consisted of cuboidal to low columnar cells lacking atypia. The epithelial cells had moderate amounts of pale cytoplasm and fairly uniform, round to oval nuclei containing fine chromatin and inconspicuous nucleoli (Fig. 2B). There were no features of oncocytic differentiation. Abundant mucoid material was present, within which were scattered foamy macrophages (Fig. 2C). No hyaline globules were identified.
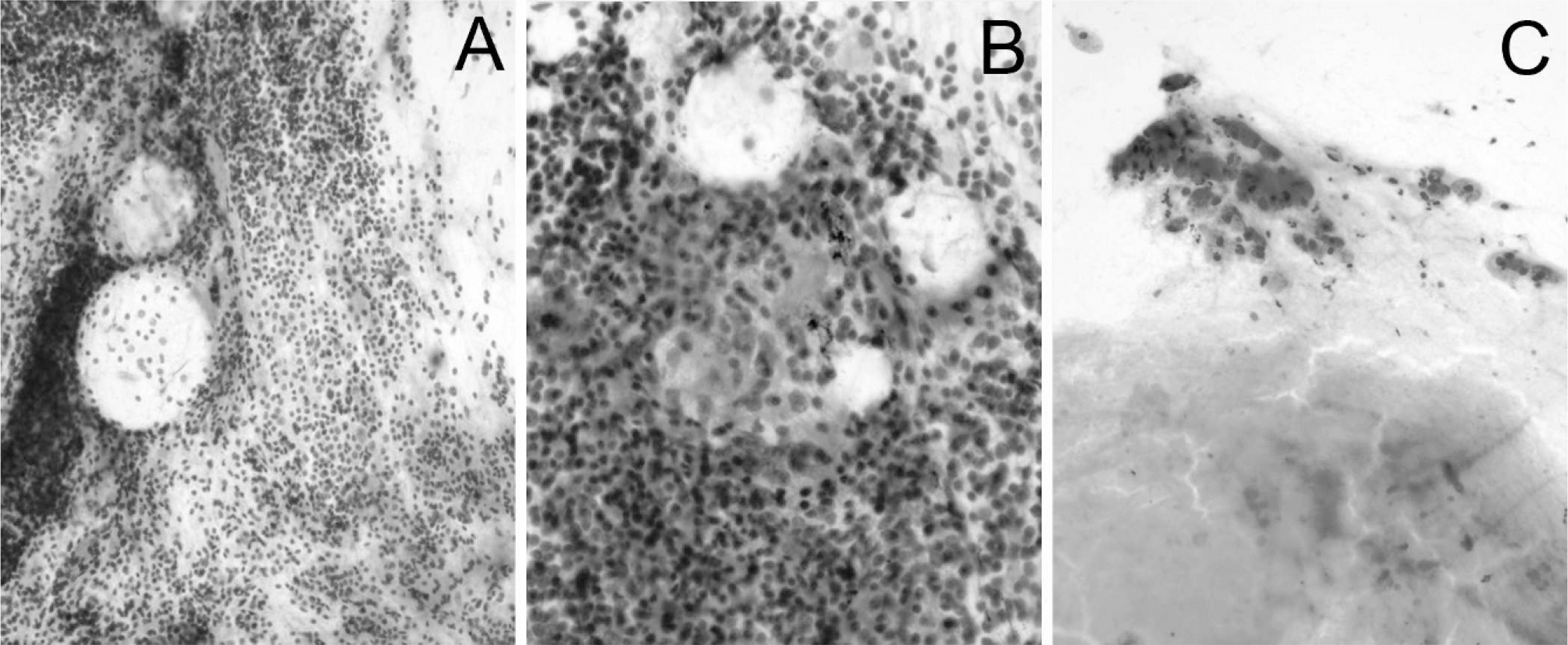
Cytologic features of the tumor include (
Histologic Features
A small amount of normal-appearing salivary gland tissue was present at one edge and separated from the tumor by a fibrous capsule. The tumor was composed of variably sized cystic cavities within abundant reactive lymphoid tissue with secondary follicle formation (Fig. 3A). The cystic spaces were filled with eosinophilic secretions with occasional histiocytes and cholesterol clefts (Fig. 3B). Secretions were also mucicarmine positive, alcian blue positive and periodic-acid Schiff positive diastase resistant (results not shown). The cysts were lined by epithelium, which varied from multilayered and cuboidal (Fig. 3B) to attenuated and flat (Fig. 3C). There were focal areas showing a more cellular haphazard proliferation of epithelial cells with formation of complex microcystic lumina containing similar secretions (Fig. 3D). The cells had a more squamoid appearance but were not mitotically active and showed minimal cytologic atypia. There were no identifiable features of stromal invasion in the tumor.
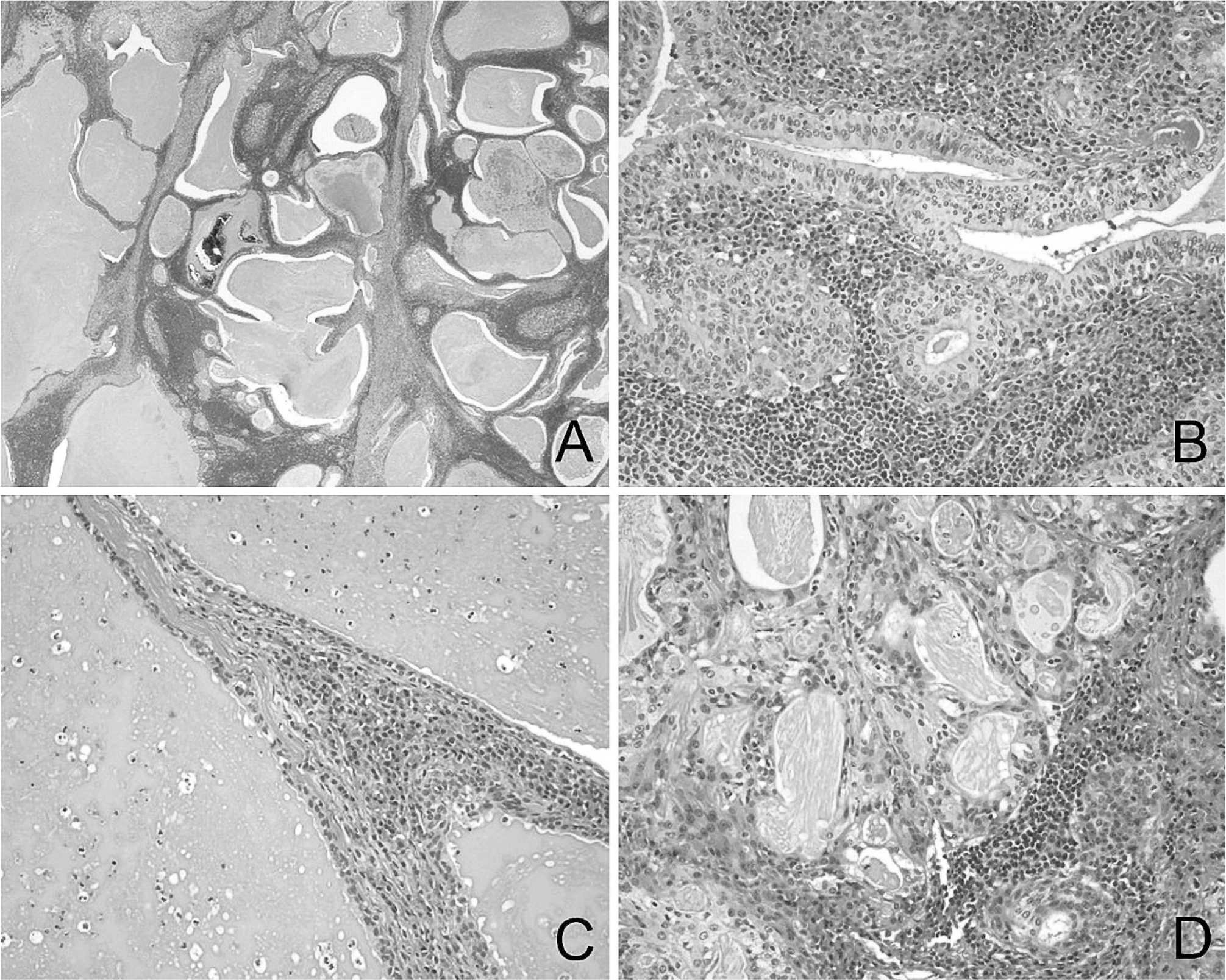
Histologic features of the tumor include (
Immunohistochemistry
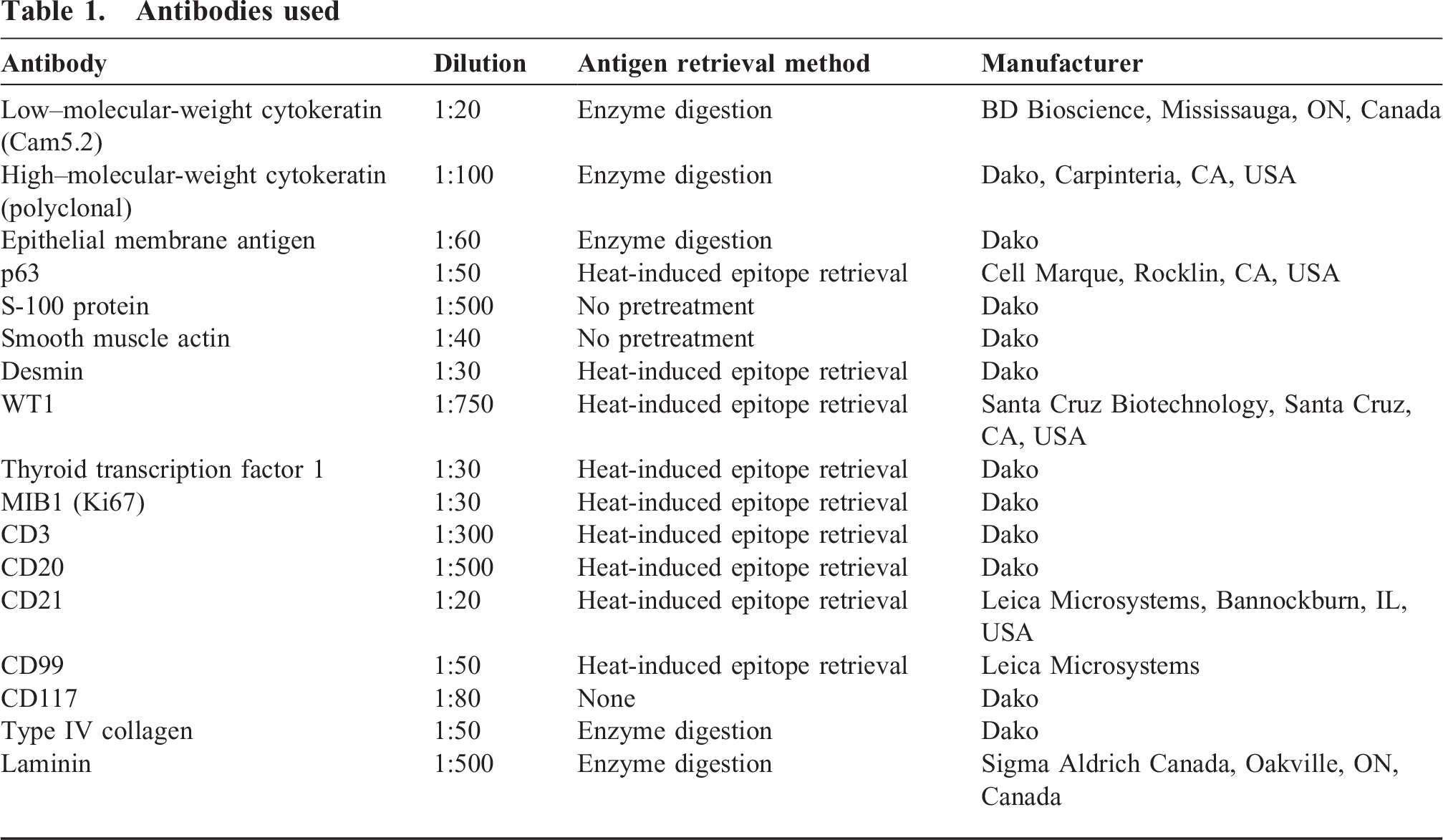
The following antibodies were used: low- and high-molecular-weight cytokeratins, epithelial membrane antigen, p63, S-100 protein, smooth muscle actin, desmin, WT1 and thyroid transcription factor 1, MIB1, CD3, CD20, CD21, CD99, CD 117, type IV collagen, and laminin. Antibody dilutions, antigen retrieval methods, and antibody manufacturers are listed in Table 1. The epithelial component showed diffuse positivity for high- and low-molecular-weight cytokeratins. Epithelial membrane antigen was positive in a patchy distribution along the luminal aspects of the epithelial cells. P63 was positive in the abluminal layer of epithelial cells and negative in the luminal layer (Fig. 4A). S-100 protein, smooth muscle actin, thyroid transcription factor, desmin, and CD99 were all negative. CD117 showed patchy positivity in luminal epithelial cells but with a staining intensity less than that of scattered mast cells in the stroma (Fig. 4B). Type IV collagen and laminin were negative, indicating absence of a basement membrane around the epithelial nests. The lymphoid component consisted of populations of B- and T-lymphocytes in their appropriate cellular compartments as identified by immunostaining for CD3 and CD20. A follicular dendritic cell meshwork was highlighted by CD21 staining and was present in lymphoid stroma between cysts and glands deep within the substance of the tumor. MIB1 showed a proliferative index of virtually 0%, even in the more complex microcystic areas, although lymphocytes were focally positive, particularly in germinal centers. In situ hybridization for Epstein-Barr virus-encoded RNA was negative.
Antibodies used
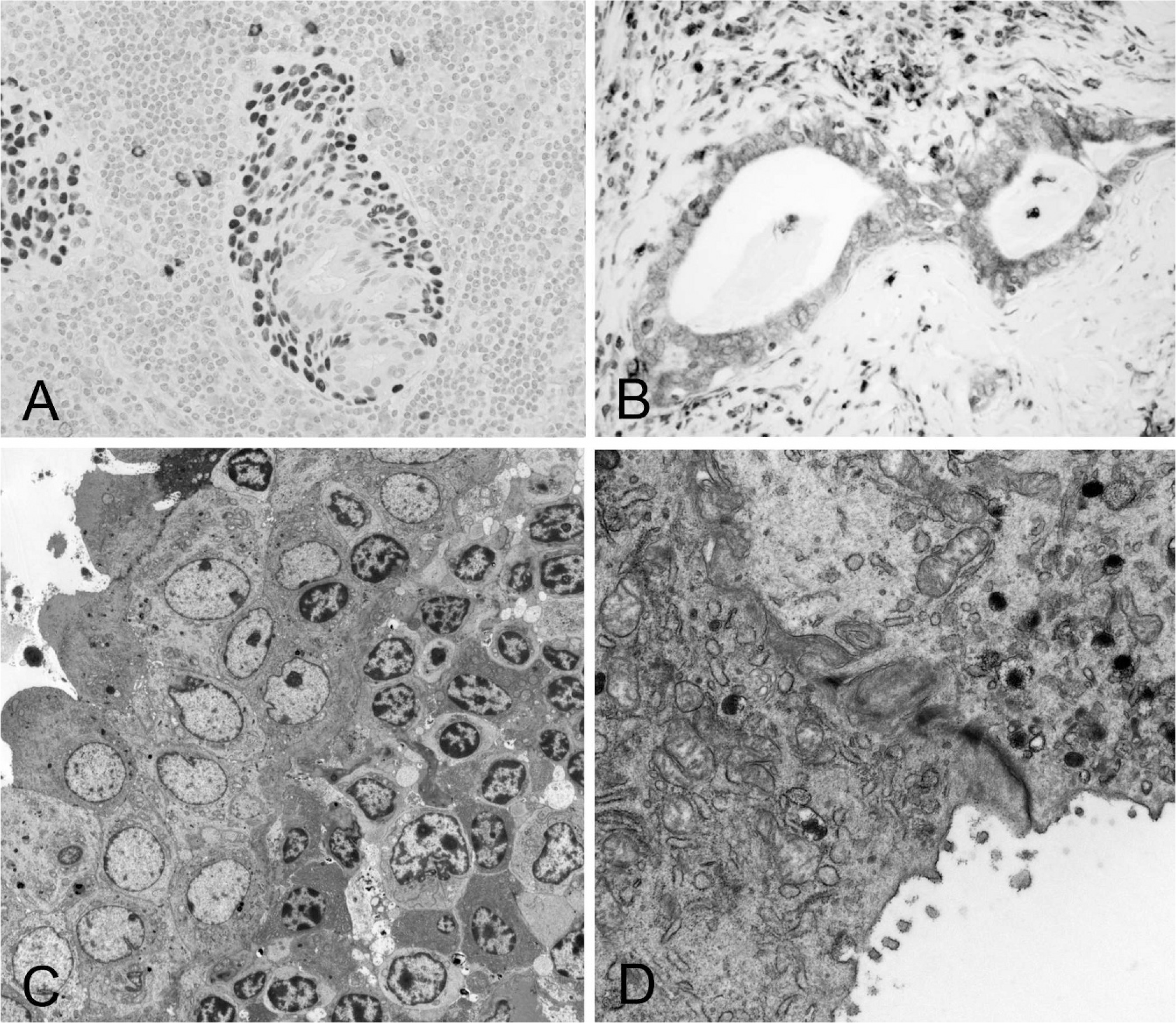
Immunohistochemical staining for p63 is positive in the basal layer of the epithelial cells (
Ultrastructural Features
Electron microscopy confirmed the large numbers of lymphocytes and plasma cells adjacent to epithelial cells (Fig. 4C). The epithelial cells had complex infoldings of the intercellular membranes characteristic of glandular type cells. Only small numbers of mitochondria were present. Luminal and basal epithelial cells could be distinguished on the basis of the former showing microvilli present on luminal surfaces and cytoplasm containing numerous secretory vesicles and lysosomes with formation of Golgi complexes (Fig. 4D). Basal cells were comparatively featureless. Myoepithelial differentiation was not apparent, and basement membrane material was not identified.
Cytogenetics
G-band analysis at 350-band resolution showed a normal female karyotype 46XX.
DISCUSSION
Lymphadenoma is a rare salivary gland tumor, with only 11 published cases [3–11]. This tumor is even more uncommon in the pediatric age group, with only a single reported case [9] to which we now add a second. The clinical features of the previously reported cases of lymphadenoma are summarized in Table 2. The age of presentation ranges from 13 to 80 years (mean 49 years). More cases have been reported in males (7 cases) than in females (5 cases, including the present case), and the majority of cases (8 cases, including the present case) have involved the parotid gland. Clinical follow-up data are scarce, and the longest reported period of follow up is 4 years [9]. Thus far, this type of tumor has demonstrated a benign course, and complete surgical excision appears curative [1,12].
Published cases of lymphadenoma
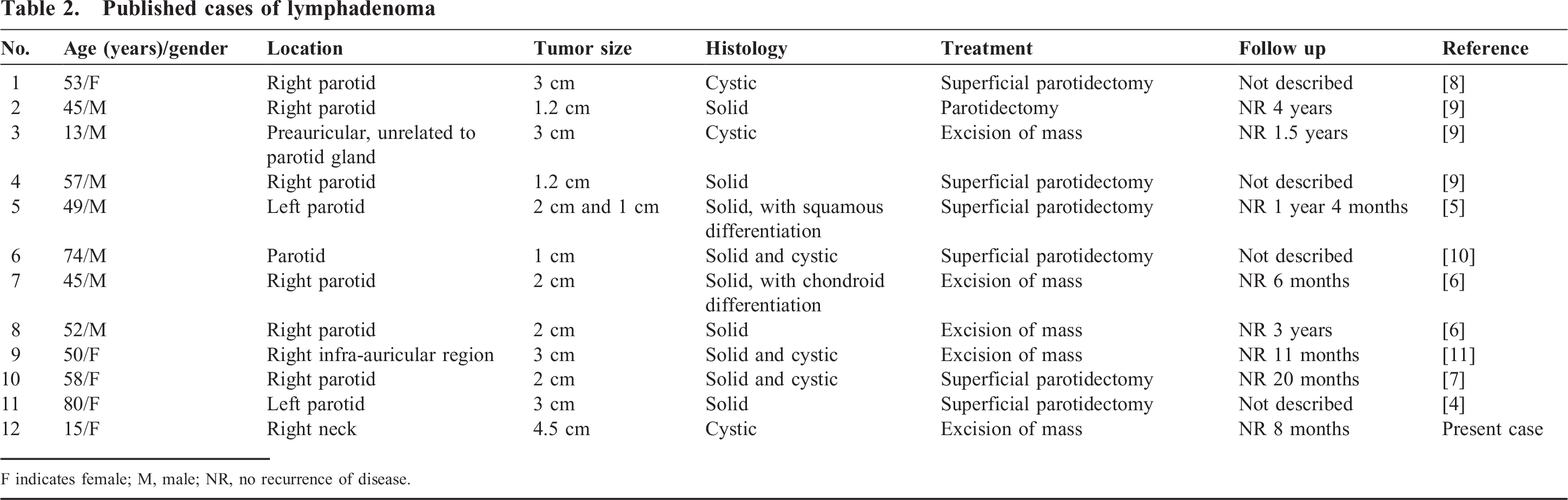
F indicates female; M, male; NR, no recurrence of disease.
The histologic features of this lesion have been well described in previous reports, and criteria for diagnosis include (1) well-defined tumor mass with a lack of nodal capsule or subcapsular sinusoids; (2) predominant lymphocytic component with or without germinal centers; (3) solid, glandular, or cystic epithelial nests; (4) no sebaceous differentiation; and (5) no oncocytic epithelium. By these criteria, there is a spectrum of appearances for the epithelial component, with some tumors composed of epithelial nests, islands, or trabeculae not associated with gland or cyst formation and others showing prominent glandular or cystic structures that vary in size and contain proteinaceous eosinophilic secretions within which foamy macrophages can be present. The cysts are lined by variably attenuated epithelium, lacking atypia and displaying dual luminal and abluminal differentiation. Some authors consider lymphadenoma to correspond to a form of basal cell adenoma when solid and a form of cystadenoma when cystic, both accompanied by a heavy lymphoid infiltrate [1,12]. Viewed from this perspective, lymphadenoma would be not a specific tumor type; rather, it would be considered a variant of other adenomatous epithelial tumors but with a prominent lymphoid component. The general consensus from the published cases, however, is that lymphadenoma represents a distinct entity with a spectrum of histology.
Additional histologic features of lymphadenoma have been described, mainly in the more solid variants. Squamous differentiation has been noted with keratin pearl formation [5]. This is a not unexpected feature, given that salivary basal cell adenomas may display focal squamous metaplasia. More unusual is the presence of chondroid differentiation described in one case [6]. Chondromyxoid stroma is a typical constituent of pleomorphic adenoma rather than basal cell adenoma, and its presence in a case of lymphadenoma suggests that the morphologic spectrum may extend to cases showing some features of pleomorphic adenoma combined with a prominent lymphoid component. Periodic-acid Schiff-positive and diastase-resistant basement membrane-like material has also been described to surround epithelial islands in cases of noncystic lymphadenoma, akin to that seen in basal cell adenoma.
Our case demonstrated a immunohistochemical profile similar to that previously reported for this tumor [7,9,11]. The epithelial cells displayed luminal and abluminal differentiation. Luminal differentiation has been demonstrated by positive staining for epithelial membrane antigen and low-molecular-weight cytokeratins and abluminal differentiation by high-molecular-weight cytokeratins and p63 [12]. Myoepithelial differentiation as detected by S-100 protein and/or smooth muscle actin is often negative in lymphadenoma [6,9,11], as with the present case, implying that the myoepithelial cell does not participate to any significant degree in lymphadenoma, in contrast to some other salivary gland tumors. CD117 is positive in luminal (glandular) cells of various types of salivary gland tumors, as in our tumor, and is no longer considered specific for adenoid cystic carcinoma [12]. Immunohistochemical staining for basement membrane components type IV collagen and laminin was negative in the present case, implying that this tumor differs from the typical basal cell adenoma that characteristically has basement membrane formation [6]. This case is the first to be studied by electron microscopy, and the findings correlate with the light and immunohistochemical results. Epithelial cells showed luminal and basal differentiation and did not display oncocytic features. Myoepithelial differentiation and basement membrane formation were not seen. Overall, the diagnosis of nonsebaceous lymphadenoma can generally be made by routine light microscopy with awareness of this entity. Immunohistochemical stains may be helpful in confirming the light microscopic impression, using a low-molecular-weight cytokeratin for highlighting luminal epithelial cells and p63 for basal cells.
Staining for the proliferation marker MIB1 (Ki67) has only been reported once [7], showing “occasional” positivity, whereas in the present case, there was no staining of tumor cells, although lymphoid cells were occasionally positive. This other report also assessed cell kinetics by flow cytometry, and the tumor was diploid, with ~4% in the G2M phase [7]. However, the technique used would also include the reactive lymphoid tissue; hence, it is difficult to know whether the tumor cells were actually cycling at this level. The present case is the first to undergo karyotypic analysis, showing a normal karyotype as might be predicted for a benign tumor. This result corresponds to the diploid DNA content documented in the above reported case by flow cytometry.
The differential diagnosis has been previously detailed by others [6,9] and principally includes nonneoplastic conditions, such as lymphoepithelial sialadenitis, chronic sialadenitis, and lymphoepithelial cysts related to acquired immune deficiency syndrome, as well as other salivary gland tumors with a prominent lymphoid component (eg, Warthin tumor, sebaceous lymphadenoma, lymphoepithelial carcinoma, lymph nodes containing metastatic carcinoma, in particular mucoepidermoid carcinoma). Lymphoepithelial sialadenitis is commonly but not exclusively seen in Sjögren syndrome and is characterized by lymphocytic infiltration of the salivary gland with parenchymal atrophy and formation of lymphoepithelial islands (hyperplastic ductal cells infiltrated by lymphocytes) that are not a feature of lymphadenoma. Chronic sialadenitis features periductal lymphoplasmacytic infiltrates and progressive periductal fibrosis but preservation of the normal architecture, distinguishing it from lymphadenoma. Lymphoepithelial cysts may occur in children but are most common in the adult population. They resemble branchial cleft cysts histologically; are unilocular; and are lined by squamous, cuboidal, or columnar epithelial cells with dense lymphoid tissue in the cyst wall [13].
Warthin tumor can resemble lymphadenoma in having cystic spaces lined by bilayered epithelium and a background of dense lymphoid tissue but can be distinguished from the latter by the formation of papillae and the oncocytic phenotype of luminal epithelial cells. Although Warthin tumor is the second most common benign parotid salivary gland tumor in the general population, its occurrence in the pediatric population is exceedingly rare, with no cases documented in the computerized archives (dating back 20+ years) of the Hospital for Sick Children. Lymphadenoma is distinguished from sebaceous lymphadenoma by the absence of any sebaceous differentiation [9].
Of far greater clinical importance is the need to distinguish lymphadenoma from malignant mimics. The presence of epithelial elements rules out a diagnosis of lymphoma together with the reactive appearance of the lymphoid infiltrate. Lymphoepithelial carcinoma is rarely cystic and consists of islands of malignant undifferentiated epithelial cells dispersed within a rich lymphoid stroma. Lack of mitotic activity, lack of invasion, and presence of ductal differentiation is supportive of a diagnosis of lymphadenoma. Moreover, Epstein-Barr virus infection of the malignant epithelial cells can generally be demonstrated in patients of Asian origin in contrast to lymphadenoma [14]. Mucoepidermoid carcinoma is the most common malignant salivary gland neoplasm in childhood [15] but generally lacks a lymphoid component, unless the tumor has metastasized to a node that is biopsied. Higher-grade tumors would not usually be confused with lymphadenoma. Low-grade mucoepidermoid carcinoma can be distinguished from lymphadenoma by greater variation in size and shape of the cysts, ducts, and epithelial islands and the presence of clear and intermediate cells [16]. Generally speaking, the lack of cytologic atypia and lack of mitotic activity should allow lymphadenoma to be distinguished from malignancies. The cytologic features of this tumor that are helpful clues to the diagnosis include a prominent lymphocyte population, epithelial cells lacking atypia, and mucoid secretions associated with macrophages. The presence of the latter 2 features on a fine-needle aspiration would help distinguish this tumor from a reactive lymph node or malignant lymphoma.
In summary, we document the second case of lymphadenoma of the salivary gland to be reported in the pediatric age group. The ultrastructural findings and karotype of this tumor are presented for the first time. This is a rare benign tumor and one with which pediatric pathologists would have little familiarity. The main clinical importance is to distinguish this tumor from other malignant tumors that can resemble it.