
Abstract
Extracorporeal membrane oxygenation (ECMO) is a lifesaving therapy for infants and children with cardiac and respiratory failure. However, thrombosis and hemorrhage are common complications. To determine clinical and laboratory predictors of thrombosis and hemorrhage resulting from ECMO, records and slides were reviewed from 29 consecutive autopsies from 2004 through 2008 of pediatric patients who received ECMO at our institution. Laboratory results, including prothrombin time, activated partial thromboplastin time, platelet count, fibrinogen level, and activated clotting time, were analyzed, as was heparin dosing. Thrombosis and hemorrhage were very common, with 1 or both seen in 86% of patients. Sixty-nine percent had thrombosis, and 52% had hemorrhage after ECMO initiation, including intracranial hemorrhage in 33% of the patients in whom brain examination was permitted. Hemorrhage and thrombosis coexisted in 31% of patients. Thrombosis was significantly more common in patients with congenital cardiac disease. Duration of ECMO therapy, being on ECMO at death, sepsis, and patient age and sex did not predict hemorrhage or thrombosis at autopsy. Laboratory tests were poor predictors of thrombosis and hemorrhage, with no correlation between these complications and prothrombin time, partial thromboplastin time, platelet count, fibrinogen level, activated clotting time, or heparin dose. In conclusion, thrombosis and hemorrhage continue to be frequent complications among patients who die during or after ECMO therapy. Patients with congenital cardiac disease appear especially susceptible to thrombosis on ECMO. Prothrombin time, partial thromboplastin time, platelet count, fibrinogen level, activated clotting time, and heparin dose are poor predictors of thrombosis or hemorrhage for pediatric patients who die after ECMO.
Keywords
INTRODUCTION
Extracorporeal membrane oxygenation (ECMO) is a lifesaving therapy for patients in cardiac or respiratory failure, in which blood is circulated via cannula from a large vein through a membrane oxygenator and is returned to circulation. It is a mainstay of pediatric intensive care and is increasingly used in pediatric cardiopulmonary resuscitation [1].
Despite its clear clinical benefit, however, the ECMO circuit is associated with significant hemostatic derangement, which leads to both hemorrhagic and thrombotic complications. Upon initiation of ECMO, thrombogenic surfaces within the circuit immediately activate the coagulation system, as well as a systemic inflammatory response [2]. Over the next hours and days, ongoing coagulation and fibrinolysis consume clotting factors [3]. Meanwhile, platelets are activated and consumed as a result of surface activation and shear forces within the circuit [3,4]. To counteract the prothrombotic effects of the circuit, patients are routinely anticoagulated with heparin, which may lead to hemorrhagic complications. Additionally, comorbidities, such as organ failure and disseminated intravascular coagulation, may predispose patients to thrombosis or hemorrhage, depending on the clinical circumstances.
Hemorrhage on ECMO is common, occurring in 14%–45% of neonates, infants, and children on ECMO, depending on age and underlying disease [5–8]. Central nervous system (CNS) hemorrhage occurs in 3%–12% of patients, with the greatest risk in neonates [5,7]. Preterm infants have a higher risk still, with 36% of infants less than 35 weeks gestational age experiencing CNS hemorrhage [7]. Similarly, hemorrhage is a common autopsy finding in ECMO patients (Table 1), with reported incidences of CNS hemorrhage ranging from 17% to 52% at autopsy [9–11]. Other severe CNS complications are common during ECMO: brain death occurs in 1%–9.5% of patients, with a risk that increases with age, whereas seizures occur in 5.5%–11% [5,6].
Previous extracorporeal membrane oxygenation autopsy studies
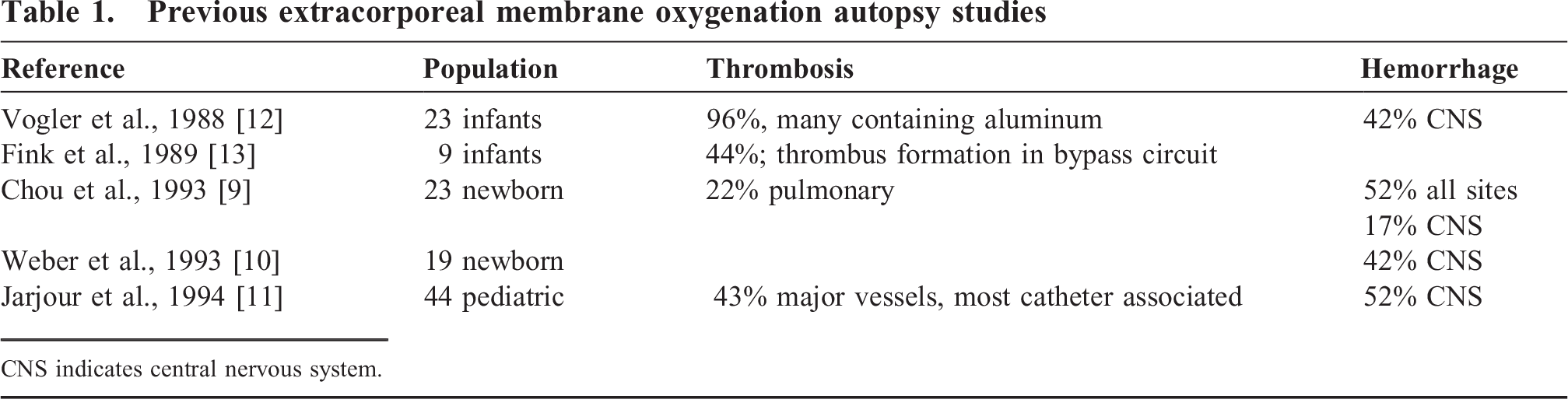
CNS indicates central nervous system.
Information about thrombotic complications of ECMO comes mostly from older autopsy studies (Table 1). Two early studies found frequent thrombosis, often linked to leaching of foreign material from the circuit, or clotting within the circuit [12,13]. More recent autopsy studies report thrombosis in up to 60% of patients [9,11].
The present retrospective autopsy series of pediatric ECMO patients had 2 goals. First, we assessed the current incidence of thrombosis and hemorrhage in pediatric patients who die after ECMO therapy, because the most recent autopsy series of pediatric ECMO patients were published 15 years ago [9–11]. Second, we investigated whether clinical history or laboratory testing can predict development of thrombosis or hemorrhage while on ECMO. We report that the presence of congenital heart disease is a strong predictor of thrombosis in this patient population. In our series, routinely performed laboratory tests of hemostasis and coagulation do not correlate with the presence of thrombosis or hemorrhage at autopsy among patients who die after ECMO therapy.
METHODS
This study was conducted with the approval of the Seattle Children's Hospital institutional review board. All patients at Seattle Children's Hospital who were on ECMO prior to death and underwent autopsy between January 2004 and December 2008 were identified by review of autopsy records and included in the study. For each patient, data were gathered from the electronic and paper chart, the autopsy report, and selected autopsy slides. Clinical information included patient age, sex, diagnosis, surgical history, duration of ECMO therapy, time from cessation of ECMO to death, and clinical or radiologic evidence of hemorrhage or thrombosis prior to death. Laboratory and pharmacologic data for the final 24 hours of ECMO therapy were collected, including prothrombin time (PT), activated partial thromboplastin time (PTT), platelet count, fibrinogen, activated clotting time (ACT), and heparin dose. Activated clotting time was measured using the Hemochron Response HR 5540 (ITC Medical, Edison, NJ, USA), a point of care instrument. During ECMO therapy, the ACT is recorded on an hourly basis and the heparin infusion rate is adjusted accordingly. Quality assurance, instrument training, maintenance, and oversight were provided by the Department of Laboratories at Seattle Children's Hospital, and the tests were performed by the ECMO nurses. Other laboratory tests were performed in the central laboratory at Seattle Children's Hospital. Prothrombin time, PTT, and fibrinogen levels were measured using a STA Compact (Diagnostica Stago, Asnieres-sur-Seine, France). Platelet counts were performed on a Sysmex XE-2100 (Sysmex America, Mundelein, IL, USA). Autopsy data included the presence and location of macroscopic hemorrhage and microscopic and macroscopic thrombi.
Statistical analysis was performed using Microsoft Excel (Redmond, WA, USA) and the Analyse-It software package (Leeds, United Kingdom).
RESULTS
From 2004 to 2008, 158 patients received ECMO therapy at our institution. Autopsies were performed on 29 patients who died during or after ECMO. Table 2 lists the indications for ECMO in this population, surgical history, and circumstances of death. The study population included 18 female patients and 11 males. Most were young infants, with a median age of 2 months (Fig. 1A). Duration of ECMO therapy was variable (Fig. 1B), but in many cases, the ECMO course was prolonged. Although indications for ECMO varied, 20 of the 29 patients in this series had congenital cardiac disease, with single ventricle physiology (10 patients) and ventricular septal defect (5 patients) being the most common diagnoses in this subset. Other indications for ECMO included acquired cardiac disease and congenital and acquired pulmonary diseases. Most patients had undergone surgery, including median sternotomy for all 20 congenital heart disease patients, thoracotomy in 3 additional patients for lung biopsy or congenital diaphragmatic hernia repair, and abdominal surgery in 2 patients. Eleven patients were septic at the time of death (defined as a positive blood culture within 24 hours of death). The majority of patients (21 of 29) died while on ECMO or immediately after its withdrawal; the remaining 8 patients survived for 3 to 120 days after ECMO therapy.
Study population and autopsy findings
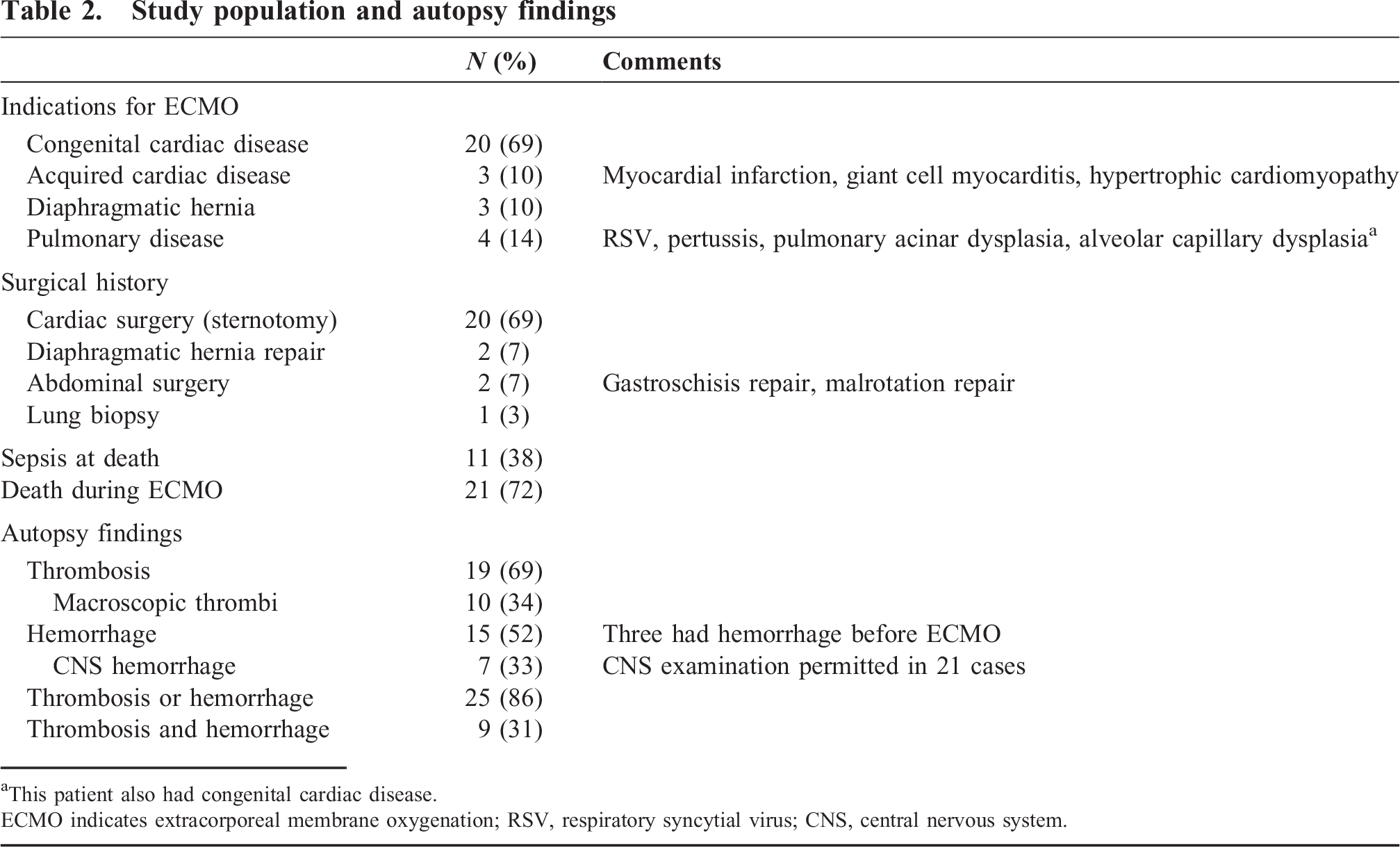
This patient also had congenital cardiac disease.
ECMO indicates extracorporeal membrane oxygenation; RSV, respiratory syncytial virus; CNS, central nervous system.
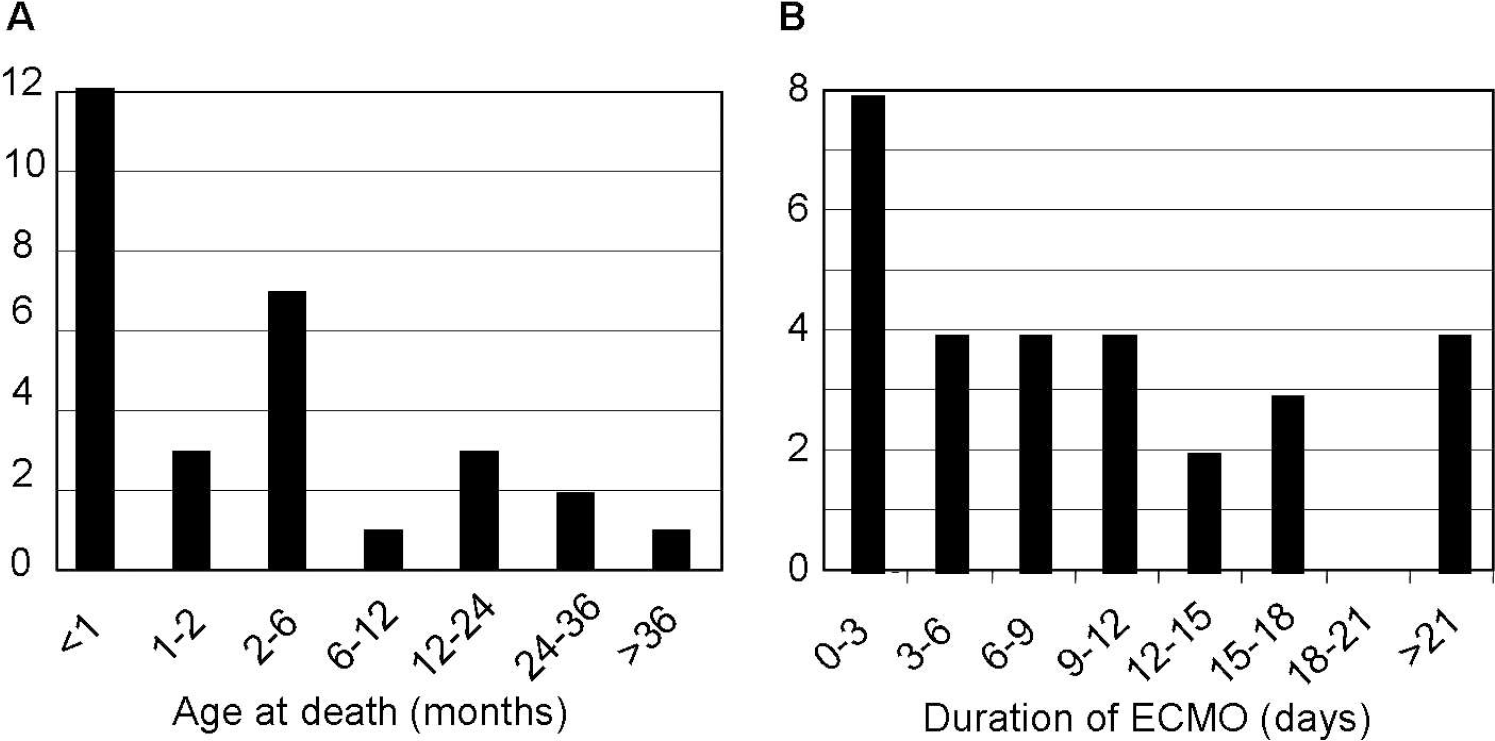
Study population characteristics, including age at death
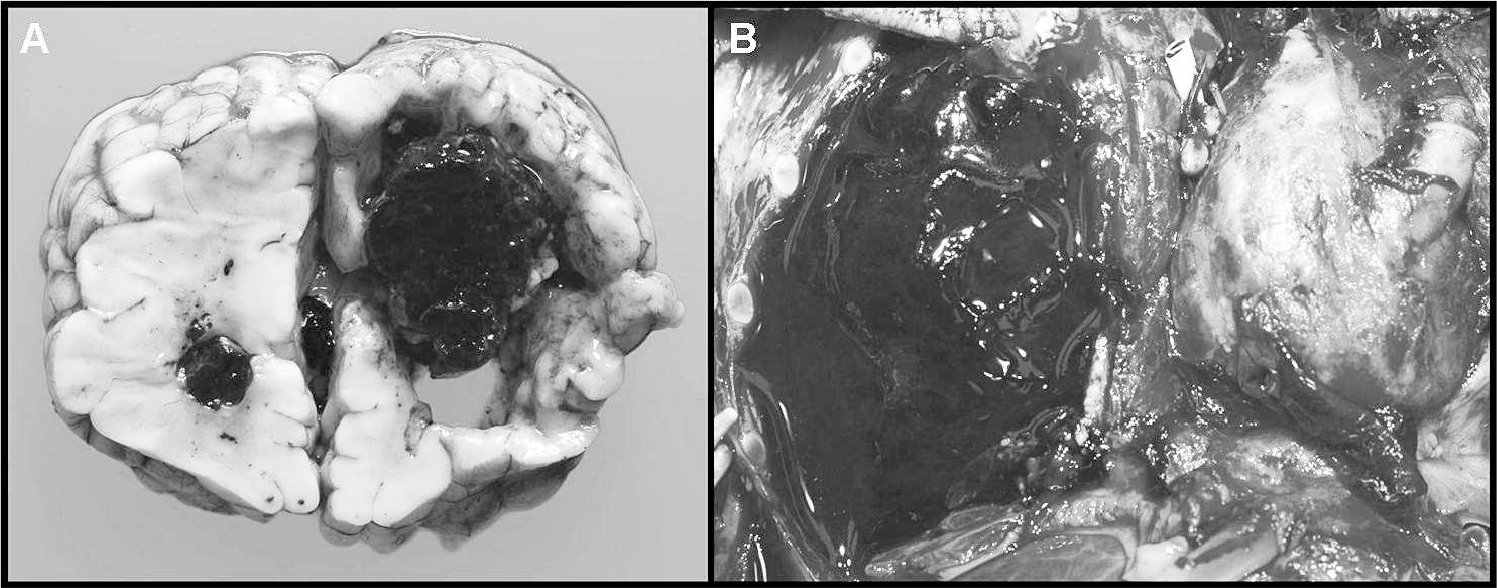
Thrombosis and hemorrhage were common findings at autopsy (Table 2). Overall, 25 of 29 patients (86%) had thrombosis or hemorrhage at autopsy, and 9 patients (31%) had both thrombosis and hemorrhage. Macroscopic (grossly identifiable) thrombi were seen in 10 patients; the most common sites were the pulmonary arteries (4 patients) and the superior vena cava (3 patients) (Fig. 2). Arterial thrombi were also seen in renal and coronary arteries and in a Sano shunt. Venous thrombi were seen in the inferior vena cava, innominate vein, iliac veins, and transverse dural sinus; in a single case, it was associated with a central venous catheter. Microscopic thrombi were present in an additional 9 patients, and 4 patients had both microscopic and macroscopic thrombi. Pulmonary microthrombi were present in all but 1 of these cases, and renal microthrombi were identified in 5 (Fig. 3). Other less common sites of microthrombi included the brain, spleen, pancreas, liver, heart, and adrenal glands.
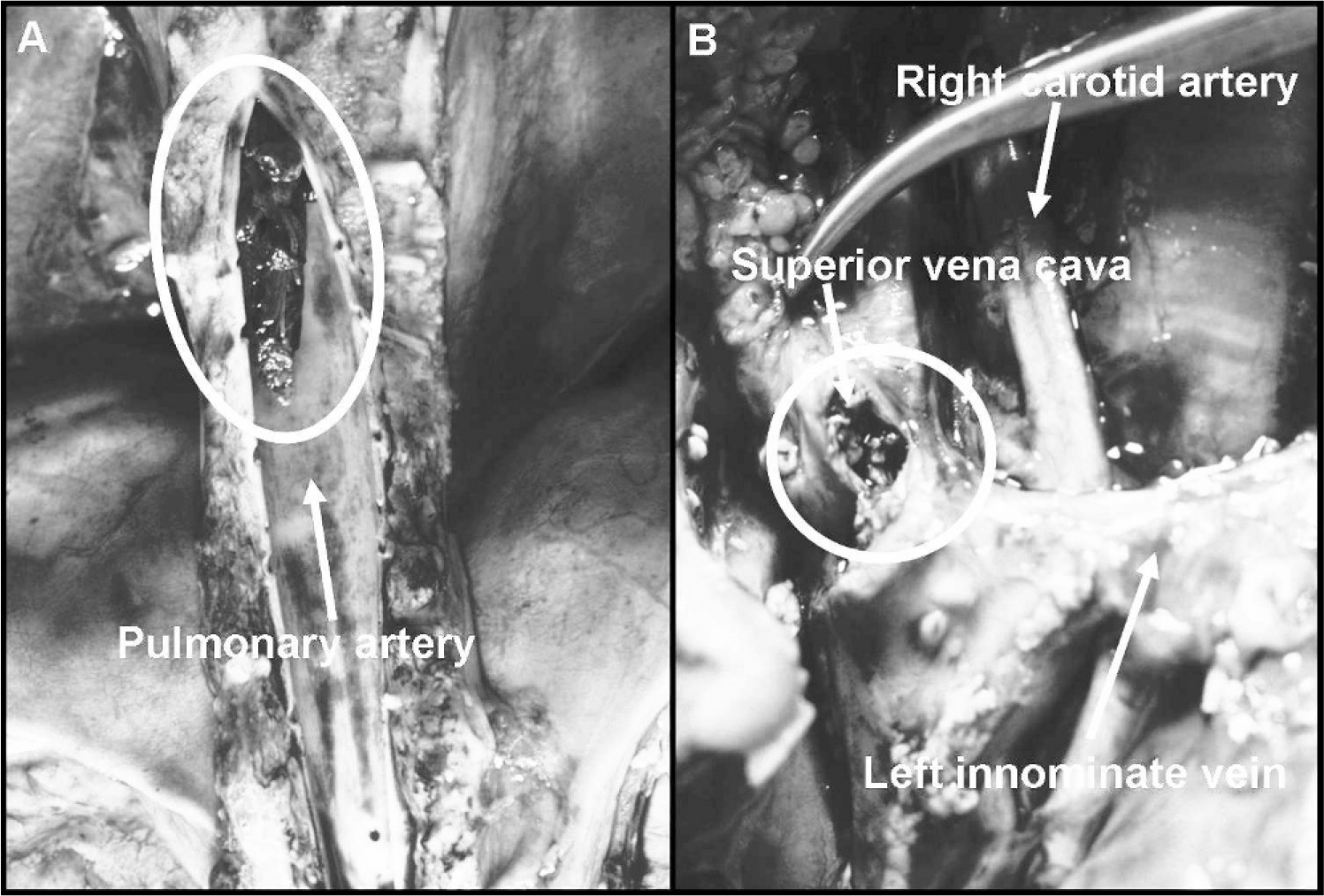
Representative images of macroscopic thrombi identified at autopsy in the pulmonary artery
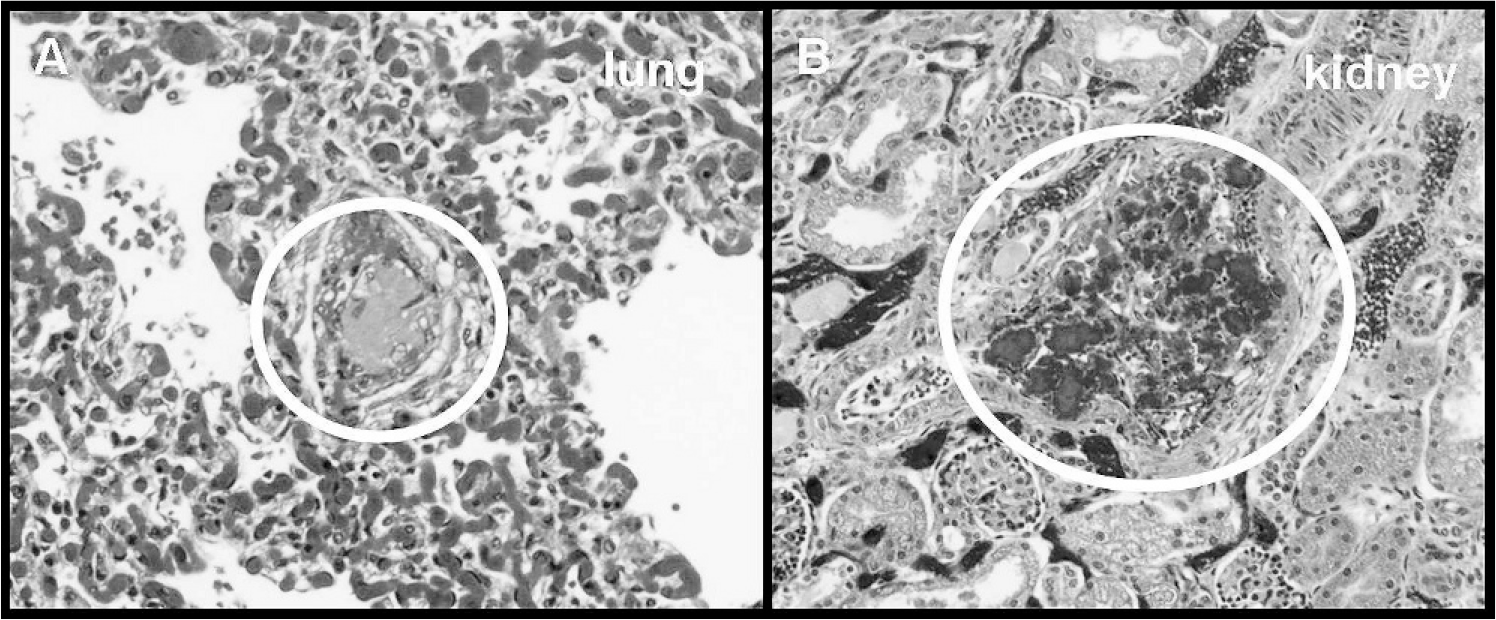
Representative images of microscopic thrombi identified at autopsy in the lung
Hemorrhage was also a frequent complication, with macroscopically identified hemorrhages in 15 patients. Three of these had known hemorrhage prior to the initiation of ECMO and were therefore excluded from further analysis. Central nervous system hemorrhage was present in 7 of the 21 patients in whom examination of the CNS was permitted (Fig. 4A), making it the most common site of hemorrhage. Pulmonary hemorrhage was identified in 6 patients, hemothorax in 2 (Fig. 4B), and intra-abdominal hemorrhage in 2. Surgical site hemorrhages and microscopic hemorrhages were not included in this analysis.
Representative images of hemorrhage identified at autopsy, including right intraventricular hemorrhage
Underlying disease was a strong predictor of thrombosis at autopsy. Thrombosis was observed in 17 of 20 patients with congenital cardiac disease (85%) but in only 3 of 9 patients with other diagnoses (33%), a significant difference (P = 0.005, chi-square test). No association was found between underlying disease and the presence of hemorrhage at autopsy. Other clinical factors, including patient age, sex, sepsis at the time of death, duration of ECMO therapy, and remoteness of ECMO therapy, did not predict thrombosis or hemorrhage.
We collected and analyzed laboratory measures of coagulation, including PT, PTT, platelet count, fibrinogen, and ACT, from the final 24 hours of ECMO. Most patients were coagulopathic on ECMO: many had elevated PT and PTT (with elevated PTT being more common); nearly all were thrombocytopenic; and fibrinogen levels varied substantially between patients but were generally low (Fig. 5). However, none of these laboratory tests correlated with the presence of either thrombosis or hemorrhage at autopsy.
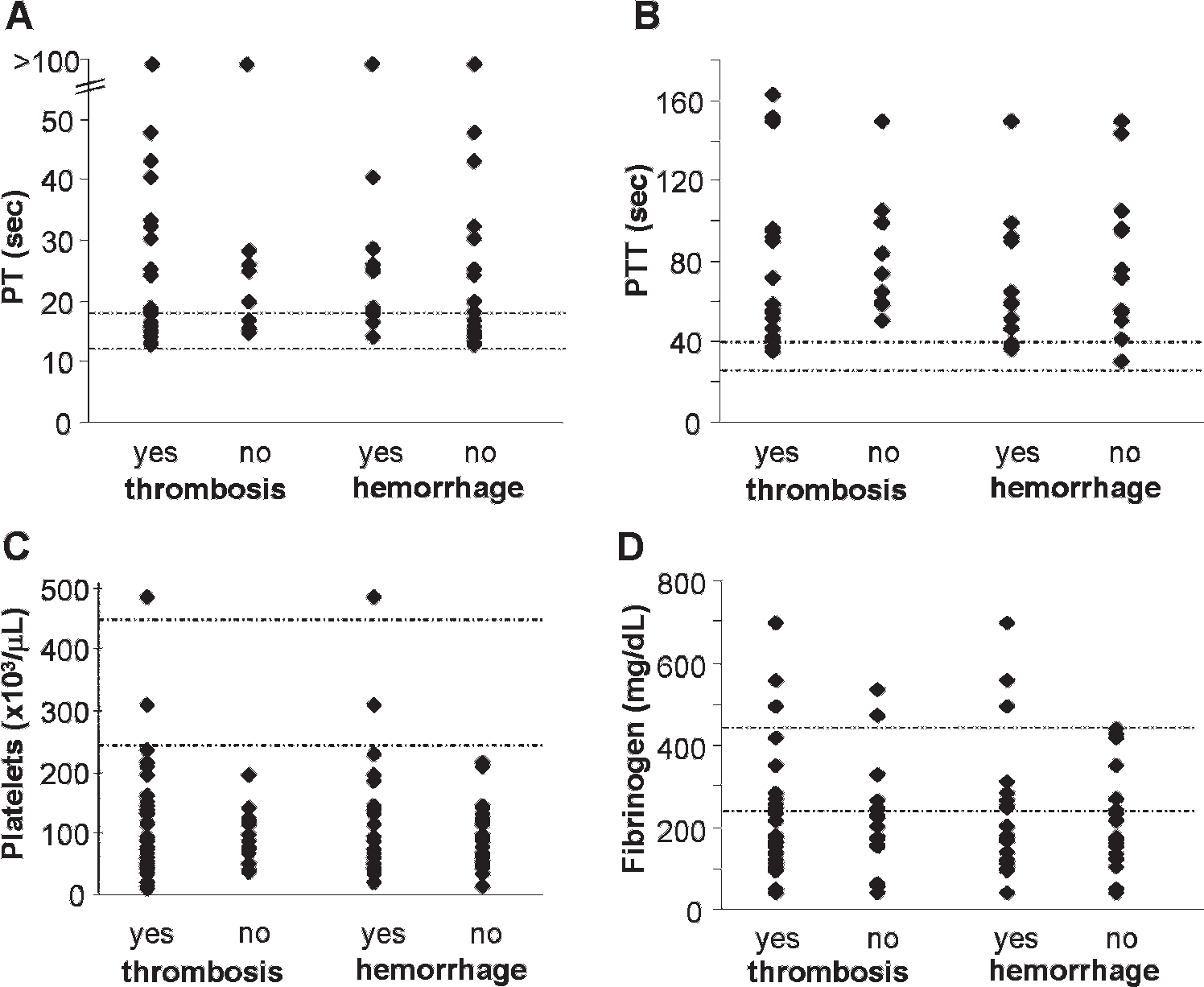
Dot plots of laboratory coagulation test results in the final 24 hours of extracorporeal membrane oxygenation. The results are grouped according to whether the patient had thrombosis, hemorrhage, or both at autopsy. Dotted lines indicate the reference range.
Most ACT values collected in the final 24 hours of ECMO were within our usual goal range of 180-220 seconds, although supratherapeutic ACTs were common, regardless of whether thrombosis or hemorrhage were identified at autopsy (Fig. 6A). Although ACTs were significantly higher among patients with hemorrhage compared with patients with no hemorrhage, the difference was too small to be clinically meaningful: the median ACT for the hemorrhage group was 214 seconds versus 209 seconds for the no-hemorrhage group (P = 0.005, 2-tailed Mann-Whitney U-test). Activated clotting times over the final 24 hours were not significantly different among patients with and without thrombosis. Similarly, heparin dosing over the final 24 hours of ECMO, when normalized for patient weight, was not predictive of thrombosis or hemorrhage at autopsy (Fig. 6B). Measures of hemostatic instability, including the amount of time a patient spent at a supratherapeutic ACT, the number of heparin dose adjustments in a 24-hour period, and the variability of ACTs (as expressed by standard deviation), also failed to predict thrombosis or hemorrhage (data not shown). Activated clotting times were generally similar regardless of the heparin dose, although some very high ACTs were recorded in patients who were receiving very little or no heparin (Fig. 7), probably reflecting coagulopathy due to other causes, such as disseminated intravascular coagulation.
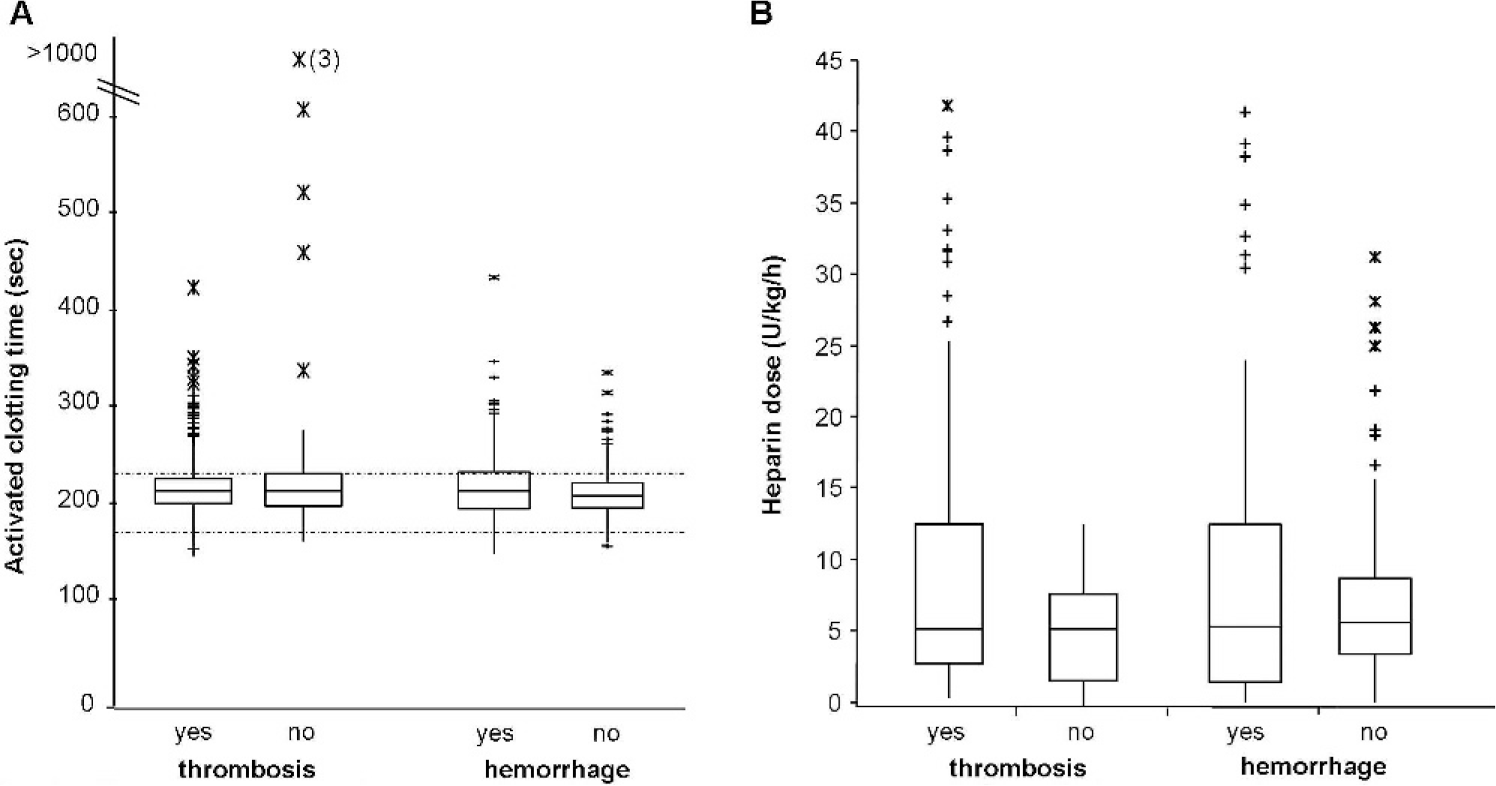
Box plots illustrating activated clotting times
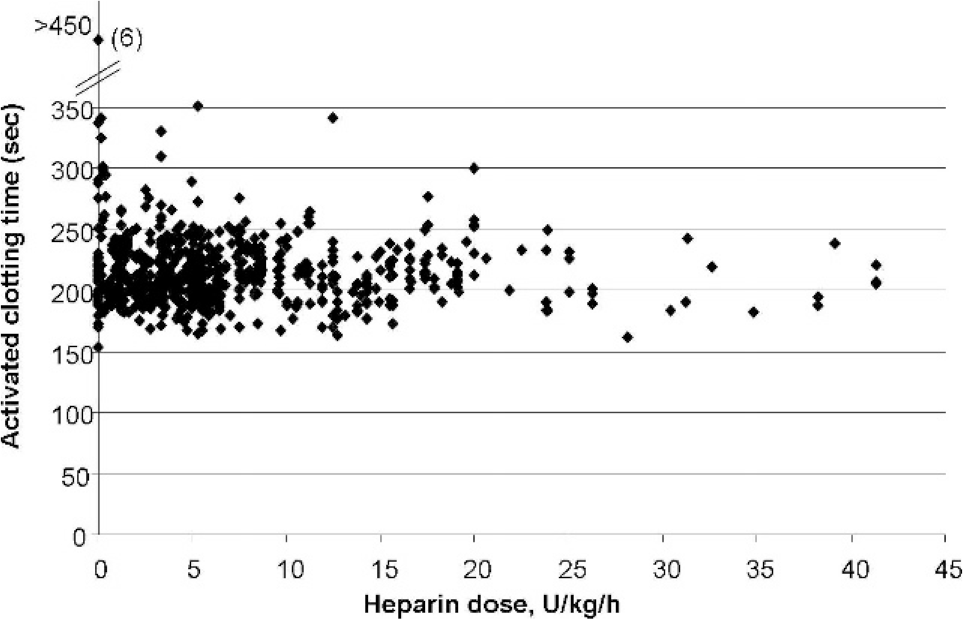
Scatter plot illustrating relationship of activated clotting time to heparin dose.
DISCUSSION
This retrospective autopsy series of 29 recent pediatric ECMO patients demonstrates that thrombosis and hemorrhage remain remarkably common complications in pediatric patients who do not survive after ECMO, despite advances in surgical and medical management of infants and children with cardiac or respiratory failure. Hemostatic complications were nearly ubiquitous in our patient series, with thrombosis or hemorrhage identified in all but 14% of patients at the time of autopsy. Hemorrhage occurred in 52% of patients, including CNS hemorrhage in 33%, frequencies similar to those reported in previous autopsy series (Table 1). Thrombosis was more frequent in our study than in historical series, occurring in 69% of patients, but it is unclear whether previous studies included microscopic thrombi in their numbers. Macroscopic thrombi were seen in 34% of our patients, slightly less frequently than thrombi in previous autopsy series (Table 1). Interestingly, thrombosis and hemorrhage coexisted in 31% of our patients, suggesting that these patients may have experienced both hypo- and hyperco-agulable states, either sequentially or concurrently.
We investigated clinical predictors of thrombosis and hemorrhage among ECMO patients, finding that patients with congenital cardiac disease are significantly more likely to have thrombosis at autopsy than those with normal cardiac anatomy. This has not been previously described, although increased incidence of thrombosis and thromboembolism has been reported among children with single-ventricle physiology after Fontan palliation [14]. In contrast to this population, the patients in our series were generally younger, and only 1 had undergone Fontan palliation. However, abnormalities of the coagulation system are common in children with single-ventricle and 2-ventricle congenital cardiac disease, even in the 1st few days of life. Relative to normal, age-matched children, these patients demonstrate decreased levels of numerous pro- and anticoagulation factors, including factors II, V, VII, VIII, IX, and X, protein C, protein S, fibrinogen, and antithrombin, and achieve adult levels of these factors at a later age compared with controls [15,16]. It is possible that delayed or uneven maturation of the coagulation system in children with congenital cardiac disease results in an imbalance of procoagulant and anticoagulant factors, leading to an increased propensity for thrombosis. Increased levels of factor VIII, an acute phase reactant, may account for some of the relative thrombophilia seen among post-Fontan patients [17]. Perhaps factor VIII levels are similarly elevated among cardiac patients on ECMO, even before Fontan palliation. Another possible explanation for the increased incidence of thrombosis among cardiac patients is that cardiac surgery might contribute to thrombophilia. Cardiopulmonary bypass, circulatory arrest, or release of tissue factor as a result of median sternotomy or prolonged surgery, for example, might lead to an increased incidence of systemic thrombosis. Alternatively, many of these patients receive artificial or tissue allograft material as part of their corrective surgery; perhaps reaction of the coagulation system to these materials leads to increased incidence of thrombosis.
Previous attempts to identify laboratory predictors of hemostatic complications on ECMO have focused on CNS hemorrhage as an outcome, yielding occasionally conflicting data. Several studies suggest that platelet levels are important in predicting CNS hemorrhage, reporting an increased risk of hemorrhage when the platelet count is less than 100 000/μL for more than 16 hours [18], when platelet counts are difficult to maintain [8], or with increased platelet transfusion requirements [19]. The ACT, a point of care test widely used to monitor heparin therapy on cardiopulmonary bypass and ECMO [20], has been studied as a predictor of hemorrhage, with mixed results. Although CNS hemorrhage is reported to correlate with the amount of time the ACT exceeds the goal range [19] and with difficulty maintaining a consistent ACT [8], another small series found no correlation between hemorrhage and ACT [18], and a recent large study concluded that the ACT did not predict mortality on ECMO [21]. The predictive value of heparin dosage is similarly uncertain. Although no correlation between heparin dosage and CNS hemorrhage was seen in an earlier study [18], Baird and colleagues [21] report that increased heparin administration correlated with increased survival on ECMO.
In this series, we found no association between thrombosis or hemorrhage at autopsy and any of the laboratory parameters of coagulation we examined, including PT, PTT, platelet count, fibrinogen, ACT, and heparin dose. Secondary measures of hemostatic instability, including the amount of time a patient spent at a supratherapeutic ACT, the number of heparin dose adjustments in a 24-hour period, and the variability of ACTs (as expressed by standard deviation), also failed to predict thrombosis or hemorrhage.
The strength of this study is the unmatched level of sensitivity to thrombosis and hemorrhage that autopsy provides, thereby establishing a gold standard for detecting disordered hemostasis after ECMO. However, because this is an autopsy series, the study is necessarily limited to pediatric patients who did not survive after receiving ECMO therapy. Extracorporeal membrane oxygenation nonsurvivors may differ from ECMO patients who survive to discharge in several respects, including clinical indications for ECMO, laboratory findings, and incidence of complications during and after ECMO. In particular, it is likely that pediatric ECMO survivors have a lower frequency of major thrombotic and hemorrhagic events than those who die after receiving ECMO. The question of how these findings apply to the general pediatric ECMO population is an important one, and it should be addressed in future investigations. However, this study does not attempt to compare the cohort of ECMO nonsurvivors to survivors of ECMO, for methodologic and logistical reasons.
The methodologic difficulties of comparing autopsy findings with findings in living patients are considerable. It is difficult to compare the different methods used to detect thrombosis and hemorrhage in these patients, because autopsy provides more detailed information about thrombosis and hemorrhage than clinical and radiologic studies in living patients. Although computed tomography, ultrasonography, and other modalities can identify large thrombotic and hemorrhagic events in vivo, they are generally used only when there is clinical suspicion of an event (with the exception of routine cranial ultrasounds in neonates on ECMO). However, thrombosis and hemorrhage may be clinically inapparent and can therefore go undetected in survivors. For instance, in several autopsies, we discovered large organized thrombi that were not clinically suspected. Similarly, small CNS hemorrhages can go undetected, especially in patients who are sedated, as is typical on ECMO. Furthermore, imaging is not sensitive to small or microscopic thrombi, which were very common in our series. Discovering these thrombi in living patients would require an invasive procedure, such as a tissue biopsy. The difference in sensitivities between autopsy and imaging complicates a comparison between the 2 populations.
From a logistical standpoint, comparing clinical data, laboratory values, and incidence of thrombosis and hemorrhage between ECMO survivors and nonsurvivors is beyond the scope of this study. The best way to make this comparison would be to prospectively study patients receiving ECMO, gathering laboratory coagulation data and clinical and radiologic findings, and in the event of death, link these data to autopsy findings. A slightly more expedient method would be to analyze data retrospectively from an age-matched set of ECMO survivors, essentially repeating the entire current study with a 2nd set of patients. However, such investigations, although worthwhile, are far beyond the scope of the current study, which is essentially a clinicopathologic and laboratory investigation, not a clinical study. Moreover, studies with a similar design and goal have been performed by others [8,17,18,21,22].
It may be that the population of patients who die after ECMO is different enough from ECMO survivors that laboratory findings are more reliable in the latter group than in the patients we examined. It is also possible our sample size of 29 patients lacked sufficient statistical power to detect a correlation between one or more laboratory measures and disordered hemostasis. However, a worrisome alternative conclusion is that none of the laboratory values routinely measured in patients on ECMO are reliable predictors of thrombosis or hemorrhage, despite the frequent occurrence of one (or both) of these complications, at least among nonsurvivors. The failure of the ACT to predict thrombosis or hemorrhage was particularly surprising, because this test is used to monitor and dose heparin anticoagulation while receiving ECMO. Activated clotting time is a point of care test and as such is susceptible to greater variability than many laboratory-based tests of coagulation. However, to reduce this variability, our Department of Laboratories provides quality assurance, maintenance, training, and oversight of the instruments. Frequent, repeated testing with the same instrument (ACTs are commonly measured every hour while the patient undergoes ECMO) demonstrates that within-patient, within-instrument variability is fairly low. Furthermore, the great majority of ACTs in our study were in the goal range, indicating that most patients were usually maintained at the desired level of heparin anticoagulation, as measured by the ACT. Although it is possible that thrombosis or hemorrhage might have been even more frequent if ACTs were outside of the goal range, maintaining an optimal ACT was not sufficient to prevent thrombosis or hemorrhage in this patient series.
This study suggests that the current routine laboratory tests used for clinical decision making are not sufficient to predict or prevent thrombotic and hemorrhagic complications in pediatric ECMO nonsurvivors. This raises questions of what testing should guide clinicians in the management of anticoagulation on ECMO and of how hemostasis should be assessed in patients receiving ECMO. Several alternatives to the ACT have been suggested to monitor and manage anticoagulation, including thrombin generation, anti-factor Xa activity, heparin levels [21], and thromboelastography [22,23]. However, these tests have not been validated in ECMO patients, and none have been assessed for their value in predicting thrombosis or hemorrhage on ECMO. Additionally, use of these tests to guide bedside management of anticoagulation poses logistical difficulties, including relatively long turnaround times compared with ACT and, in the case of thromboelastography, significant interpatient variation and complexities of interpretation. If these or other tests could be validated as possessing predictive value for clinical decision making, this might provide the impetus for developing a rapid, (ideally) point-of-care assay with improved value in managing anticoagulation and preventing hemostatic complications for pediatric patients receiving ECMO.
Footnotes
ACKNOWLEDGMENTS
The authors would like to thank Drs Joseph Siebert, Kathleen Patterson, Laura Finn, and Raj Kapur, who performed many of these autopsies. In particular, thanks goes to Dr Siebert, who took the gross photographs.