
Abstract
Smooth muscle tumors of the vulva are rare entities with variable morphologic features and clinical behavior. Our report summarizes the case of a multifocal vulvar smooth muscle tumor of undetermined malignant potential with an unusual intravascular growth pattern and subsequent local recurrence in a 10-year-old girl, the youngest case reported to date, and reviews the specific pathologic findings of that category. Vulvar smooth muscle tumors of undetermined malignant potential represent a diagnostic, prognostic, and therapeutic challenge. The histologic features of this case were predictive of local recurrence, although the significance of the intravascular growth pattern is still uncertain. The relationship of this multifocal, recurrent tumor to the clinical entity, vulvar leiomyomatosis, is unknown at this time.
Keywords
INTRODUCTION
Smooth muscle tumors of the soft tissue represent a unique class of neoplasms that have been divided into 3 general categories based on location: deep seated, superficial (including nipple), and genital (including vulvar) [1]. Each category has separate criteria for malignancy. Soft-tissue smooth muscle tumors of the genitalia are among the rarest.
CASE REPORT
A 10-year-old Hispanic female presented to the emergency department for evaluation of a left vulvar mass and associated discomfort. The mass had 1st been noted 2–3 months prior to presentation. The review of systems was otherwise unremarkable and specifically negative for any trauma, fever, or abnormal bleeding. Menarche began 4–5 months prior to presentation, and her cycles were irregular. Past medical and surgical history was negative. The patient has an older healthy male sibling, and family history was negative for malignancy.
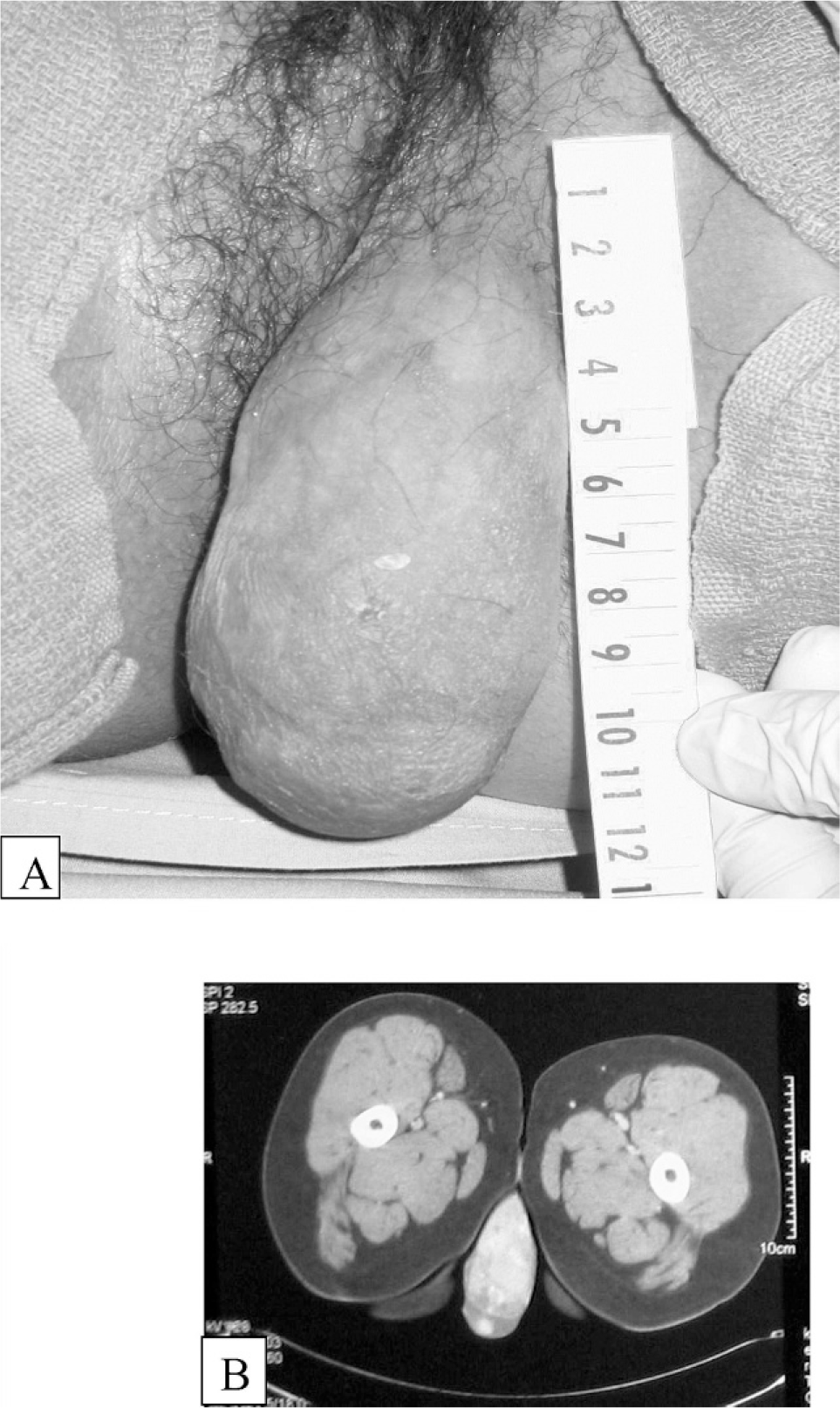
Initial evaluation in the emergency department included physical examination and ultrasonography. The examination revealed a healthy, well-developed female and unremarkable results, with the exception of the gynecologic findings. The gynecologic exam was significant for 2 firm fairly mobile but nonreducible masses of the left labia majora, which were tender on palpation. The masses were approximately 4 cm and 8 cm in greatest dimension, very closely approximated, and located superficial in the labia, just deep to the dermis (Fig. 1A). Prominent vascularity was noted on inspection. The ultrasound confirmed the presence of 2 vulvar masses closely approximated, characterized as complex and heterogeneous in appearance with extensive vascularity. The uterus and adnexa were normal. A computed tomographic scan of the pelvis was obtained to rule out communication with the abdominal cavity and to evaluate for associated adenopathy. The labial mass was seen on computed tomographic scan and was again noted to be quite vascular (Fig. 1B). Importantly, the computed tomographic scan confirmed normal pelvic anatomy, normal bowel, and no adenopathy.
Excision was recommended for definitive diagnosis and alleviation of discomfort. An incision over the medial aspect of the left labia was made, the most prominent vessels were ligated, and then sharp dissection of each mass was performed. The masses were relatively superficial with some extension into the soft tissue but were not adherent to any underlying structures. Two discrete masses with smooth capsules, extensive vascularity, and mixed solid and cystic consistency were removed intact and without complications. The patient tolerated the procedure well.
The patient underwent serial examinations every 4–6 months for surveillance and was without evidence of disease until approximately 26 months after the initial excision, when she was noted to have 2 small firm areas on the left labia again just deep to the dermis. These areas were nontender and mobile, and each measured approximately 0.5 cm in greatest dimension. A repeat excision with pathologic examination was performed. Postoperatively, a computed tomographic scan of the pelvis was performed to rule out adenopathy or local spread of disease, and this revealed normal anatomy, with the exception of the areas of the recent resection consistent with postoperative healing.
The patient continued to be in otherwise good health and was followed with serial exams. There were no changes in her family or medical history during this surveillance period. Three and a half years after the original diagnosis, she was again noted to have several small nodular areas of the left vulva. These lesions were again resected in the same manner as the previous lesions. There were multiple small lesions noted in the superficial aspect of the labia just deep to the dermis without adherence to underlying structures. They were again rounded, firm, and mobile on exam and on palpation during the procedure. The lesions ranged in size from a few millimeters to several centimeters.
PATHOLOGY
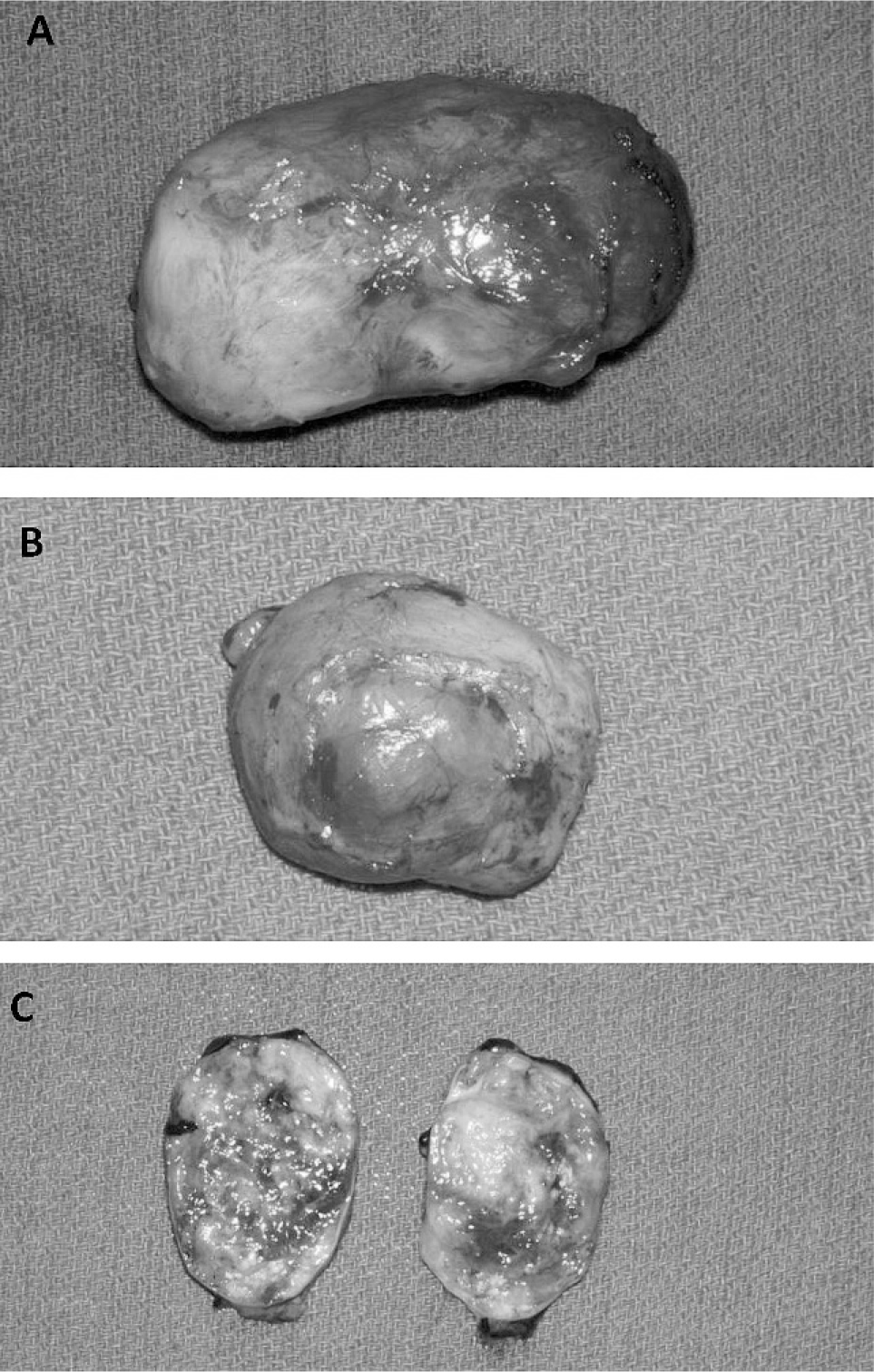
Gross examination of the diagnostic resection specimen revealed 2 distinct masses. The larger mass was 81.8 g, 8.6 ×4.8 ×3.3 cm, ovoid, and covered with an intact thin, translucent fibrous capsule (Fig. 2A). Upon sectioning, the mass had a heterogeneous maroon to tan-white, solid, and focally gritty cut surface. The smaller mass was 12.2 g, 3.9 ×3.3 ×3.2 cm, roughly ovoid, variably solid, and fluctuant and also covered with an intact thin, translucent fibrous capsule (Fig. 2B). Sectioning of this mass revealed a thin-walled, fluid-filled cystic structure containing a 3.0 ×1.8 ×1.2 cm portion of pink-tan solid tissue.
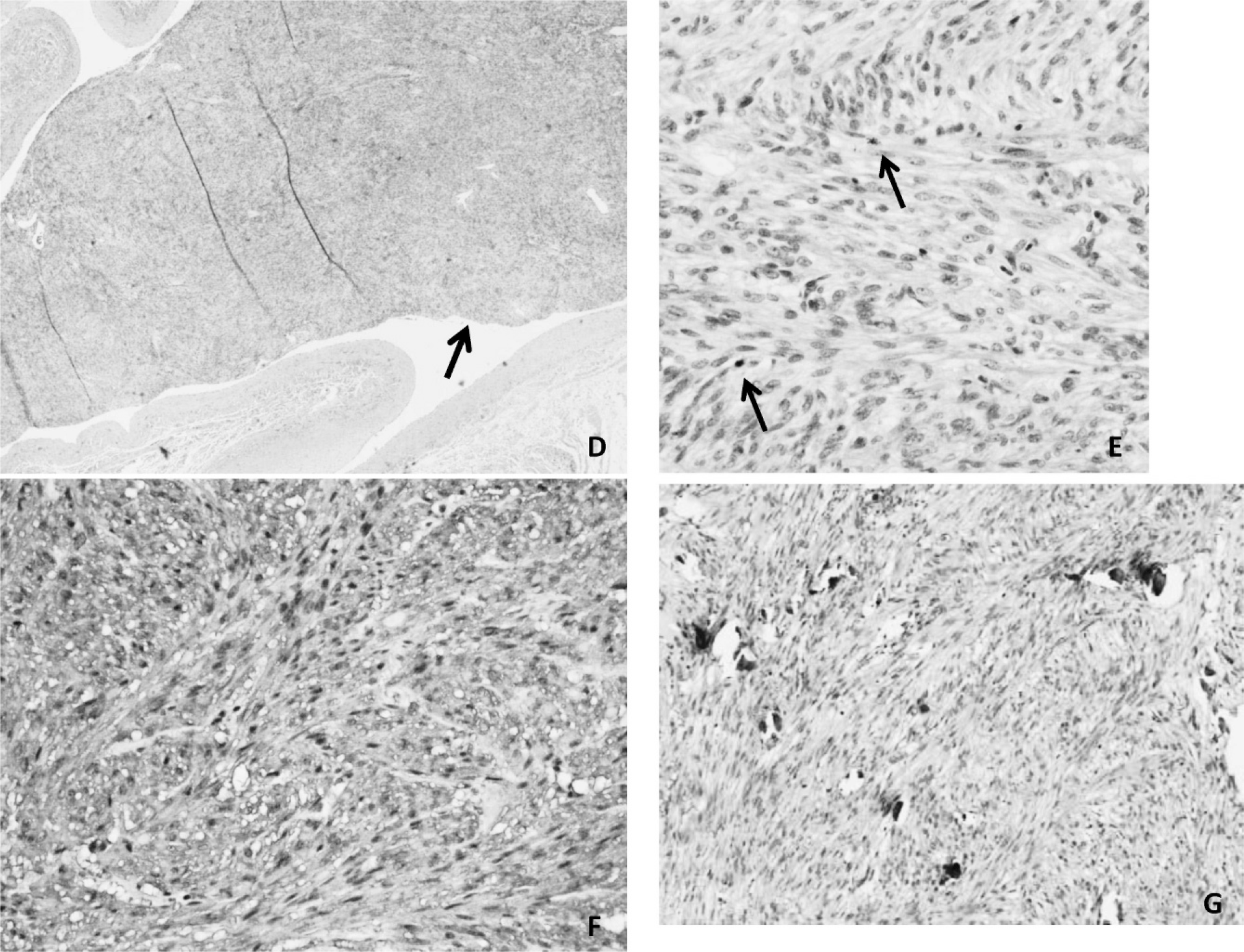
Microscopic examination of both masses revealed largely encapsulated, densely cellular and vascular, spindle-cell tumors with focal areas of edema and hyalinization. Tumor cells were arranged in randomly orientated fascicles, having nuclei ranging from oval to elongated and spindled, with stippled chromatin, variably prominent central nucleoli, and abundant lightly eosinophilic cytoplasm. The tumor cells showed minimal atypia and focal epitheliod change. Abundant calcifications were present. Prominent intravascular tumor growth was identified in the smaller mass. The tumor cells were diffusely positive for smooth muscle actin, muscle-specific actin, and desmin; focally positive for progesterone receptor (<10% showed nuclear staining); and negative for epithelial membrane antigen, S-100, CD10, CD34, inhibin, estrogen receptor, and CD117. The larger mass had <1 mitotic figure per 10 high-power fields (HPFs), and the smaller mass had 2–3 mitotic figures/10 HPFs on average, but at least 2 HPFs with 9 and 17 mitotic figures. MIB-1 stains performed on sections from both masses showed a proliferation index of approximately 3–9% in the larger mass and 7–12% in the smaller mass. The largest mass was interpreted as a cellular leiomyoma, and the smaller mass was interpreted as a smooth muscle tumor of uncertain malignant potential.
Cytogenetic analysis performed on both masses revealed normal female karyotypes. Fluorescent in situ hybridization analysis for the t(X;18) was negative.
Approximately 26 months later, several resected, skin-covered fragments of tissue, excised to a depth of 0.8 cm, were received. The tumor cells were arranged in nodules and identical histologically to the original diagnostic specimen. Tumor was again noted within a vessel. One histologic section revealed up to 9 mitotic figures/HPF within the tumor nodules. MIB-1 stains demonstrated a proliferation index of 3–5%, with 1 nodule showing a 10% proliferation index. The diagnosis of recurrent smooth muscle tumor was rendered.
A 3rd resection specimen, 3.5 years after the original diagnostic procedure, consisted of 2 ovoid, well-circumscribed masses, 2.4 and 3.2 cm in greatest dimension. Histologically, the tumor cells again were similar to the diagnostic specimen. Mitotic figures numbered 2/40 HPFs. MIB-1 stains demonstrated similar proliferation indices to the previously resected specimens. Tumor was again noted in the vascular spaces. Similarly, the diagnosis was recurrent smooth muscle tumor.
DISCUSSION
Smooth muscle tumors of the distal genital tract represent a rare and diverse group of tumors whose clinical behavior and pathologic characteristics have yet to be fully understood. The characteristics of size, circumscription, and specific mitotic counts have been utilized to delineate benign vulvar smooth muscle tumors from those with greater recurrent potential [2–5]. Recommended criteria for malignancy, proposed by Tavassoli and Norris [2] in their 1979 study of 32 vulvar smooth muscle tumors, includes 3 features: size ≥5 cm, infiltrative margins, and ≥5 mitoses/10 HPFs. Additionally the authors noted that those tumors that lacked infiltrative margins but exhibited ≥5 mitotic figures/10 HPFs and were ≥5 cm in size were likely to recur. No relationship between cellular atypia and tumor recurrence rate was established. In contrast, Nielsen and colleagues [3] in their cohort of 25 vulvar smooth muscle tumors identified significant atypia as a common finding in those tumors that recurred or metastasized. Thus, their group proposed a 4th additional criteria for malignancy, moderate to severe cytologic atypia, with the diagnosis of sarcoma being advised in cases that fulfilled 3 of the 4 criteria. Finally, in a review article, Nucci and Fletcher [1] reported the presence of any mitotic activity, nuclear pleomorphism, and infiltrative margins as features favoring local recurrence. These authors also suggest that tumor necrosis favors a diagnosis of leiomyosarcoma, when seen in association with any of the 4 accepted criteria. When a tumor only partially fulfills the criteria for malignancy, the use of a borderline or smooth muscle tumor of undetermined malignant potential (STUMP) category has been advocated by Tavassoli [2], an atypical leiomyoma category by Nielsen and colleagues [3], and an atypical smooth muscle tumor category by Nucci and Fletcher [1].
Further classification within the category of smooth muscle tumors was difficult in our case. Both original tumors failed to meet all the criteria for malignancy established by Tavassoli and Norris. Although the larger mass was >5 cm (8.6 cm), it was well circumscribed, without necrosis or significant atypia, and had a low mitotic rate, thus only meeting 1 criterion for malignancy. Due principally to the increased mitotic rate focally of the smaller tumor, a diagnosis of STUMP was rendered in our patient. The mitotic rate on at least 1 of the recurrent specimens (up to 9 mitotic figures/HPF) did support classification as a vulvar STUMP as well.
The prominent intravascular growth seen in the smaller mass of the initial diagnostic specimen and the subsequent recurrences are interesting findings. This feature, while being well described in the uterine corpus, has not been described in the literature with respect to vulvar smooth muscle tumors. Uterine leiomyomatosis is characterized as a clinically benign entity, composed of nodules of bland smooth muscle cells located within venous spaces [6]. To the best of our knowledge, such an intravascular growth pattern has not been described in smooth muscle tumors of the vulva that do not meet strict criteria for malignancy, as in our case. Interestingly, on multiple occasions, computed tomographic scans of the pelvis in our patient did not reveal uterine abnormalities, and therefore the likelihood of these vulvar smooth muscle tumors with notable intravascular growth patterns representing involvement by uterine leiomyomatosis is very unlikely.
A condition known as vulvar leiomyomatosis exists, in which patients present with multiple mucosal-based smooth muscle tumors in the vulva. Cases are usually seen in association with Alport's syndrome but have been described without this entity [7]. These patients may develop leiomyomas of the esophagus most commonly, as well as of the uterus and tracheobronchial tree. Computed tomographic scans in our patient did not reveal any evidence of nodular lesions elsewhere; notably, however, the patient has not had a scan of the chest to evaluate for esophageal lesions. Additionally, the patient does not have a significant family history or abnormal kidney function to suggest Alport's syndrome, although this clinical entity may not manifest until later in adulthood. Metachronous occurrence of esophageal leiomyomas [1,7] is well described in the reports of vulvar leimyomatosis, so the absence of other lesions at this time in our patient does not exclude the potential for such manifestations in the future. Although the reports of vulvar leiomyomatosis do describe multifocality of lesions, as seen in our case, interestingly, they do not describe intravascular growth patterns or concerning histologic features, such as atypia and increased mitotic figures.
In our case, we illustrate a vulvar smooth muscle tumor that has an unusual intravascular growth pattern and was difficult to initially classify, as well as local recurrence of this tumor, in the youngest patient reported to date. Its original histologic features have, according to the literature, been accurately predictive of local recurrence. In addition to the already proposed criteria for predicting local recurrence, it is easy to hypothesize that intravascular tumor growth may also be indicative of a higher risk of local recurrence. The relationship of this multifocal, recurrent tumor to the entity vulvar leiomyomatosis is uncertain at this point, because the patient does not display any other clinical manifestations associated with that entity. Therapy remains a dilemma at this time, because it is likely that surveillance and repeat resections will be required in the future. It is conceivable that antihormone therapy may be used in the future, but in a patient this age, the option to utilize such medications is limited because of her need to continue normal development. Although currently the patient is without disease, she will remain under surveillance and close follow up.
Footnotes
ACKNOWLEDGMENT
We thank Dr F.A. Tavassoli for her expertise and assistance with this case.