
Abstract
Although twin pregnancies complicated by a coexisting complete hydatidiform mole are uncommon, those with partial hydatidiform mole (PHM) are exceedingly rare; there are only several well-documented cases diagnosed antenatally. Here we present the first case of a twin placenta containing a nodular embryo associated with PHM diagnosed on routine placental examination. This dizygotic twin pregnancy featured viable embryos at 8 weeks' gestation, death of 1 embryo at 12 weeks, and delivery of a healthy infant by caesarean section at 28 weeks because of worsening maternal reflux nephropathy. Macroscopic and microscopic placental examination and fluorescence in situ hybridization showed one part of the placenta to be diploid and the other to contain a vanishing triploid embryo and a PHM, which had eluded antenatal ultrasound diagnosis. Careful pathologic examination of vanishing twins and their placentas may disclose an unexpected PHM, which can be associated, albeit infrequently, with persistent gestational trophoblastic disease or a trophoblastic tumor.
INTRODUCTION
Complete hydatidiform mole (CHM) is the result of a diploid androgenic conceptus, which demonstrates avascular villi with central cisterns in the chorionic villi and atypical trophoblastic hyperplasia, while diandric triploid conception features the partial hydatidiform mole (PHM) with avascular hydatid villi with trophoblastic hyperplasia without atypia, intermixed with normal villi. Digynic triploid placentas do not demonstrate these features [1,2]. Other diseases with double-male imprinting such as Beckwith-Wiedemann syndrome may feature placental mesenchymal dysplasia, sharing some features of the molar placenta [2]. The CHM, and to a lesser extent the PHM, can be associated with persistent trophoblastic disease with persistently elevated β-human chorionic gonadotropin (β-hCG), the latter used for follow-up. Choriocarcinoma may occur with metastasis, but is highly curable if diagnosed and treated [3].
The rates of multiple conceptions vary significantly but they may constitute more than 12% of natural conceptions (70% of them dizygotic), with only 2% of them surviving to term [4]. As 1% to 3% of all conceptions are triploid [5]—85% of them diandric [1]—this would yield the theoretical incidence of PHM of roughly 7 in 1000 to 2 in 100 dizygotic pregnancies, provided that diandric triploidies indeed produce PHM, which is not always the case [6]. These expected frequencies of PHM in twin pregnancies seem to be much more than diagnosed in practice [7,8], particularly antenatally [9,10]. However, the true rate of PHM in twin pregnancy is unknown, and there is even more uncertainty how to manage such patients [11].
“Vanishing twin” is the loss in a later ultrasound of a usually dichorionic twin seen by ultrasound in the first trimester [1,4]. The frequency of the phenomenon can be predicted from the high frequency of early pregnancy loss due to chromosomal abnormalities and the high incidence of dizygotic twinning as many vanishing twins are not clinically discovered.
We report a unique case of a vanishing twin and a PHM associated with a normal dizygotic twin diagnosed on placental examination at the turn of 2nd and 3rd trimester of pregnancy.
CASE REPORT
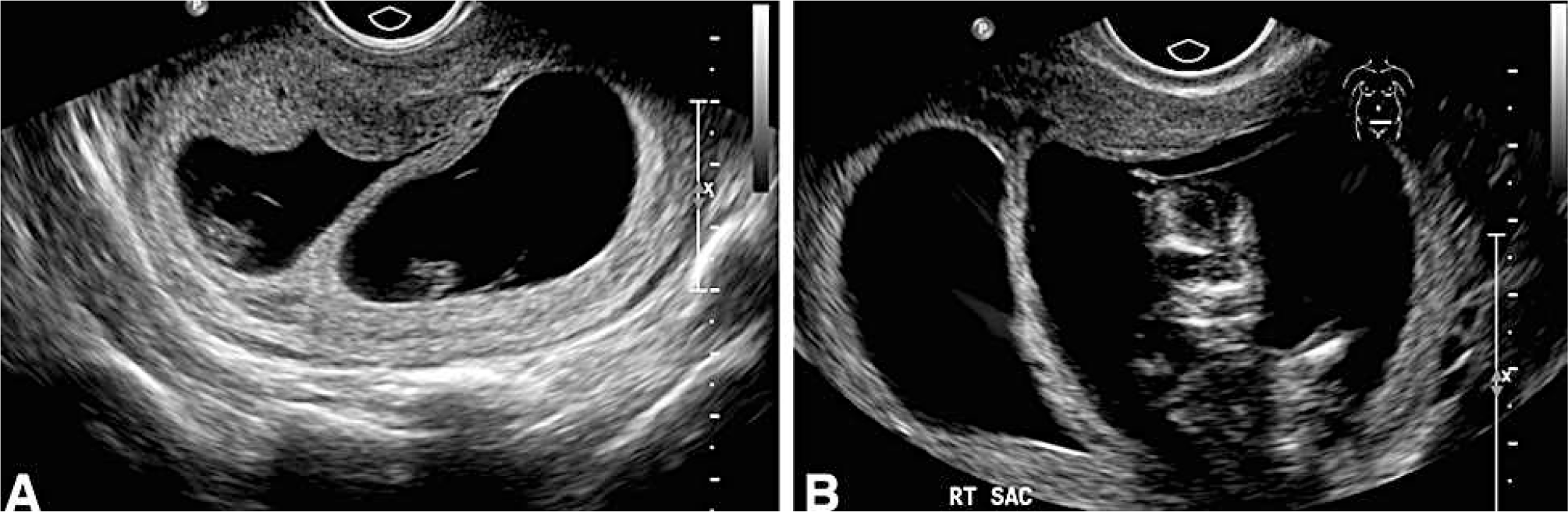
A 29-year-old woman, G3P3, with chronic renal impairment secondary to reflux nephropathy, had a dichorionic twin pregnancy with viable embryos diagnosed by sonography at 8 weeks' gestation (Fig. 1A). At 12 weeks, a repeat ultrasound scan showed death of one embryo with an “essentially empty” gestational sac, consistent with a vanishing embryo, and a normal 2nd fetus (Fig. 1B). A healthy preterm male infant was delivered by elective caesarean section at 28 weeks because of worsening maternal renal function.
Sonographic findings at 8 weeks (
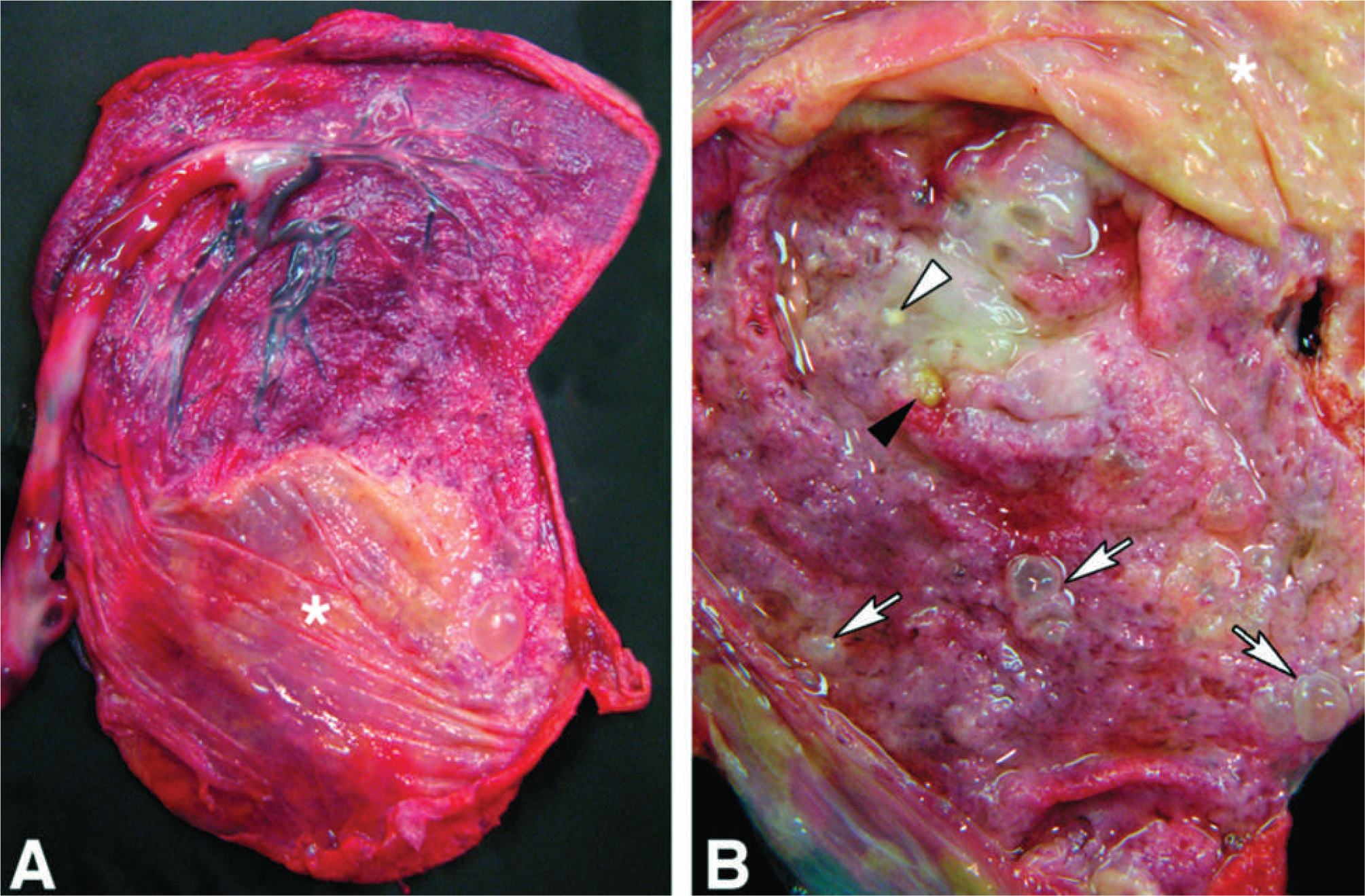
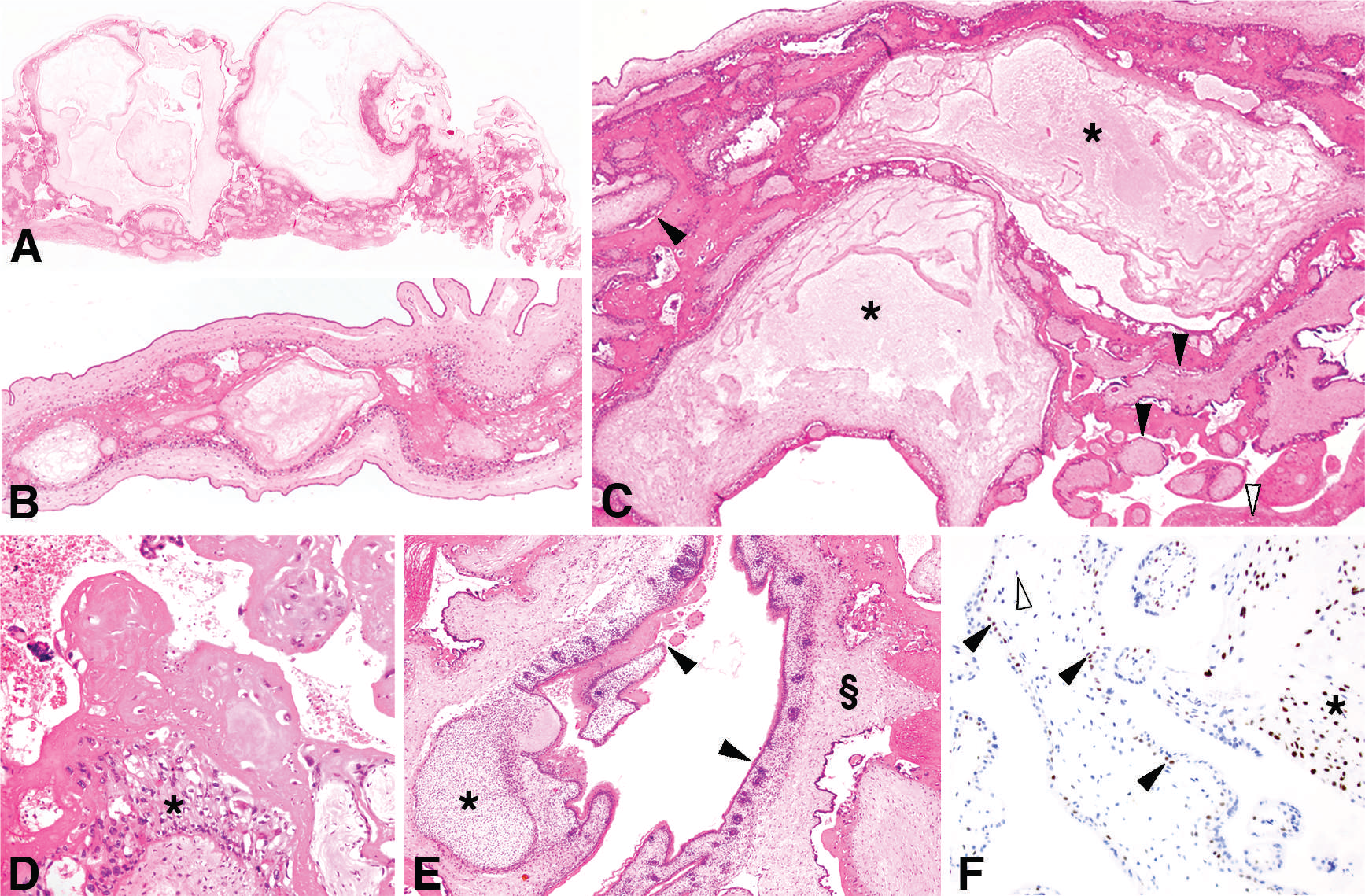
The dichorionic diamniotic fused twin placenta was composed of a normal 117-g part and a flattened fibrotic 39-g part with an intact chorionic sac, absent umbilical cord, calcified yolk sac remnant, and a 4-mm C-shaped embryo fused with the chorionic plate, the latter studded with vesicles up to 8 mm (Fig. 2). Microscopically, placental tissue from the smaller and grossly fibrotic part showed a double population of chorionic villi, some with hydatid change and cistern formation, and others small and fibrotic (Fig. 3A–C), with focal trophoblastic proliferation without atypia, suggestive of PHM (Fig. 3D). The embryonal tissue contained disorganized skin and cartilage (Fig. 3E). Histologic examination of placental tissue from the viable infant was normal for the gestational age. Immunohistochemistry for p57 was positive in the molar (Fig. 3F) and nonmolar placentas.
Microscopic findings.
Conventional karyotyping was not performed but FISH of molar and embryonal tissue showed trisomy 13, 18, 21, and X, and therefore a presumed 69,XXX karyotype. The FISH of the normal placenta showed disomies of chromosomes 13, 18, and 21 and single chromosomes X and Y, therefore a presumed 46,XY karyotype.
Retrospective evaluation of the antenatal ultrasound at 8 weeks' gestation revealed a dichorionic pregnancy with 2 viable embryos and subtle cystic structures in 1 placenta (Fig. 1A), but both the embryo and the cystic structures were absent at the 12-week ultrasound, which showed a twin pregnancy with a vanished embryo (Fig. 1B). The maternal β-hCG 1 year after delivery was within the normal range (<2.0 IU/L).
DISCUSSION
To our knowledge, this is the 1st report of a twin pregnancy with a normal diploid fetus and a vanishing triploid embryo that eluded antenatal diagnosis of PHM because of lack of clinical or obvious ultrasonographic indicators of molar pregnancy. The diagnosis was made by gross and microscopic examination of placenta delivered at the turn of the 2nd and 3rd trimesters of pregnancy and was confirmed by FISH. Rare cases of PHM complicating twin and triplet pregnancies have been reported but, unlike our case, they were diagnosed antenatally in the 2nd and 3rd trimesters and not as a component of a vanishing twin [9,12]. This case is illustrative of some important points in the diagnosis of PHM in general and that associated with twin pregnancy in particular.
In the 1st trimester, many cases of PHM are either asymptomatic, as was our case, or present with nonspecific findings of vaginal bleeding or missed abortion. Ultrasound examination in early pregnancy may detect HM before the onset of clinical manifestations but only about half of the cases of HM are identified in this way, with the sensitivity for PHM being 20% compared with 95% for CHM [13]. The reversed incidence of CHM and PHM in singleton and multiple pregnancies [7,10] indicates that many cases of PHM are underdiagnosed in early multiple pregnancies.
In our case, the early ultrasound revealed twin pregnancy but not molar pregnancy. Only retrospective review of sonograms identified small cystic changes in the placenta of 1 fetus. Such cystic changes, however, even if noticed, do not allow one to antenatally distinguish between PHM and placental mesenchymal dysplasia, and antenatal karyotyping by amniocentesis and different gross and microscopic appearances of these 2 conditions are helpful [2].
Because of this, the gold standard for diagnosis of PHM is histopathologic examination of products of conception. A recent study of 1606 women undergoing a surgical evaluation in which HM was not suspected showed the incidence of HM to be 2.5% [13], indicating that a significant proportion of HM cases demonstrate minimal hydropic change in the 1st trimester and are therefore likely to remain unidentifiable by ultrasound examination prior to evacuation.
In such difficult cases, the p57 immunostaining is extremely helpful in exclusion of CHM in which villous trophoblasts and stromal cells show no nuclear positivity [14]. However, p57 immunostaining alone cannot differentiate between PHM, placental mesenchymal dysplasia, hydropic abortus, and nonmolar pregnancy, in which, as in our case (Fig. 3F), the nuclear positivity is observed in villous cytotrophoblasts and stromal cells. The maternal placental tissue (decidua) and extravillous trophoblasts are positive in all pregnancies, molar and nonmolar. Therefore, CHM could be excluded in our case solely on the basis of p57 immunostaining, but of course the CHM was not in the differential diagnosis in the first place based on the gross examination and conventional hematoxylin and eosin histologic examination.
It almost goes without saying that histologic diagnosis of HM can be more complicated in the 1st-trimester products of conception of multiple pregnancy in which various proportions of molar tissue can be admixed with normal chorionic villi of a co-twin. The p57 immunostaining can be helpful when CHM is a component of multiple pregnancy, but diagnosis can be very difficult when PHM or placental mesenchymal dysplasia is present. In such cases only cytogenetics, flow cytometry, FISH, or even more complex genetic studies for abnormal imprinting may be needed. As the incidence of multiple pregnancies has increased because of assisted fertilization techniques, so should the incidence of PHM, which can even be recurrent in such situations [15].
Partial hydatidiform mole is easier to be diagnosed in the 2nd trimester, if symptomatic, but usually at a later gestational age than CHM [10]. In our totally asymptomatic case, the diagnosis was made only on routine placental examination, which stresses the importance of a careful gross and histologic examination of placentas in general, and of vanishing twins and their placentas in particular, as an unexpected PHM potentially associated with persistent GTD and/or choriocarcinoma may be disclosed [3]. Because of the small number of reported cases of twin pregnancies including PHM and a normal twin, there are insufficient data to predict the risk of developing persistent GTD in this group [8], and thus there is even more uncertainty as to how to manage such patients.
The risk of choriocarcinoma is over 1000 times higher following HM than any other type of pregnancy, but the persistent GTD occurs less commonly in association with PHM (approximately 4%) than with CHM. The literature is conflicting regarding the risk of choriocarcinoma in the context of PHM [7]. Among 3000 patients with PHM, 3 (0.001%) progressed to have choriocarcinoma in subsequent endometrial samplings [3]. Although there are only a few well-documented cases of concurrent PHM with choriocarcinoma (<0.5%), extensive sampling of placentas with PHM for isolated foci of choriocarcinoma is needed [7]. The presence of viable PHM tissue at 28 weeks of pregnancy in our case raises the question whether the risk of persistent GTD and choriocarcinoma in cases like ours is higher than in PHM aborted earlier. As there are no “normal” values for weight of PHM placentas, it is simply impossible to determine whether the molar placenta of the vanished twin (35 g) was large for gestation. Of course, the placenta was much smaller than normal for 28-week pregnancy, but the embryo died somewhere between the 8th and 12th weeks, and the average normal placental weight for this gestational age interval is comparable to our molar placental part. Although the placenta was still viable histologically and with trophoblastic proliferation, there are no data to conclude whether a “vanished” triploid twin carries more risk of persistent GTD and choriocarcinoma to the mother than an aborted PHM. In PHM received as abortion specimens, the placental tissue is usually disrupted and the completeness of curetting is impossible to assess. In our case, despite the histologic viability of the molar tissue, the placenta looked complete. Even if the persistence of the viable PHM until completion of the other twin's pregnancy increased the mother's risk compared with immediate abortion, it certainly did not happen in our case as there was no clinical or serologic evidence of persistent GTD.
In conclusion, careful gross and microscopic diagnosis of placentas of a multiple pregnancy, particularly those with an earlier sonographic diagnosis of a vanishing twin, cannot be overemphasized because an unexpected PHM carries a risk, albeit small, of persistent GTD and/or choriocarcinoma [3]. Retrospective studying of sonography tapes may also help to refine diagnostic sonographic criteria for very early PHM.