
Abstract
Sodium is usually included in hospitals' critical values lists; however, the values at which sodium is considered to be life threatening (critical) vary among hospitals. Studies of outcomes associated with hyponatremia and hypernatremia in pediatric patients have not been published. We performed a retrospective chart review of sodium values of <124 mmol/L and >155 mmol/L that occurred during a 6-month period. Univariate and multivariate analyses for mortality risk were performed with the different variables. A total of 702 (1.32%) sodium tests fell in the study reference range, with 166 being <124 mmol/L and 536 being >155 mmol/L. Although not statistically significant, mortality was higher (38.5%) in patients with sodium values ≤120 mmol/L than in those with values ≥170 mmol/L (25%) or in patients with other values (<14%). Underlying conditions prevented assessment of morbidity associated with hyponatremia or hypernatremia. Treatment was instituted within 4 hours in 80% of cases (50% within 1 hour). Multivariate analysis showed increased risk of death for hyponatremic patients if they were premature or had heart abnormalities, while for hypernatremic patients the risk increased when other critical values were present. In conclusion, sodium levels of ≤120 mmol/L and ≥170 mmol/L have increased mortality in children; however, the risk of death is not statistically different when compared to risk in patients with milder hyponatremia and hypernatremia. Risk factors for death in hyponatremic and hypernatremic patients may primarily reflect the severity of the underlying conditions present in these children, such as prematurity and heart abnormalities, rather than the sodium derangement.
INTRODUCTION
Most clinical laboratories include sodium in their critical values lists. Critical values are defined as those that indicate that the patient is in imminent danger unless appropriate treatment is instituted promptly [1]. Two surveys of pediatric hospitals designed to determine the analytes that are considered in the hospitals' critical values lists and the limits used for emergency notification have been published [2,3]. For sodium, the low cutoff critical value ranged from 110 to 130 mmol/L, while the high cutoff value ranged from 150 to 170 mmol/L. The mean low critical value cutoff was 121 mmol/L, while the mean high cutoff value was 156 mmol/L. Howanitz and Howanitz [4] evaluated clinical outcome and health care provider responses to different sodium values in adults. In their institution, 0.6% sodium results fell <120 mmol/L or were >155 mmol/L, clinicians responded to more than 50% of results within 4 hours, and mortality rates of hyponatremic and hypernatremic inpatients were 19% and 48%, respectively. To our knowledge, studies evaluating clinical outcome and health care provider responses to critical sodium values in pediatric populations do not exist.
Hyponatremia and hypernatremia are associated with an increased mortality risk in a wide range of conditions [5–9]. The clinical features of hyponatremia are linked to cerebral edema, while net water loss or, less commonly, use of hypertonic solutions are the causes of hypernatremia [10]. The severity of symptoms depends on the rate and extent of decrease or increase in serum sodium. In pediatric patients, symptoms of hyponatremia and hypernatremia are frequently not obvious as a result of young age and underlying neurologic conditions; thus, pediatricians rely heavily on laboratory values for diagnosis.
Changing the critical value list in a hospital is a labor-intensive process that requires consultation with clinicians to assess that the values are acceptable for the practice [11]. We recently revised the critical values list for our pediatric institution, which includes an academic hospital and a community physician hospital. Several physicians suggested that the low cutoff value for sodium should be raised to <124 mmol/L instead of the previously used <120 mmol/L. This study was performed to assess morbidity, mortality, and physician response to sodium values <124 mmol/L and >155 mmol/L in our pediatric hospitals. Cases with sodium values between 121 and 124 mmol/L were compared to cases with sodium values <120 mmol/L, and cases with sodium values between 155 and 170 mmol/L were compared to those with values >170 mmol/L.
PATIENTS AND METHODS
We performed a retrospective chart review of patients with plasma sodium values of ≤124 mmol/L and ≥155 mmol/L during a 6-month period (January 1, 2008, to June 30, 2008). Plasma sodium assays were performed using automated chemistry analyzers (Vitros 5,1 FS Chemistry System, Ortho Clinical Diagnostics, Raritan, NJ, USA). During the study, the critical sodium values were <120 mmol/L and >160 mmol/L. Per policy, the laboratory called critical results to health care providers and documented the calls in the laboratory computer system.
The following clinical variables were evaluated: patient age, primary diagnosis, symptoms of hyponatremia (including nausea, vomiting, headache, confusion, seizures, and coma) or hypernatremia (including anorexia, muscle weakness, nausea, vomiting, lethargy, and coma), possible sequelae, location where the value occurred, other critical laboratory results in the same sample (including glucose of <2.77 or >24.97 mmol/L or >8.32 mmol/L during the 1st week of life, potassium of <2.5 or >6.5 mmol/L, CO2 of <10 or >40 mmol/L, calcium of <1.5 or >3.5 mmol/L), number of sodium results in the study range for each patient, time of clinician response to result (from release of result to intervention), intravenous and enteral fluids the patient was receiving, length of stay, whether the patient died, and the cause of death. Spurious hyponatremic results that occurred in seven patients as a consequence of contamination with intravenous fluids were not excluded from the study; however, mortality was adjusted if the sodium value was a spurious result or if the family asked for the patient not to be resuscitated. Response to a critical result was defined as reordering plasma sodium levels (either in the laboratory or by point-of-care testing) or change in the concentration and rate at which fluids were being received, as documented in the electronic medical record.
Data were entered in Microsoft Excel 2000 (Microsoft Corp, Redmond, WA, USA), and statistical analyses were performed using SAS software (version 9.1; SAS Institute Inc, Cary, NC, USA). We divided the patients in 2 groups, hyponatremia and hypernatremia, based on the 1st value that fell in the study range. Then the hyponatremia group was subdivided into those patients with sodium values <120 mmol/L and those with values between 121 and 124 mmol/L. The hypernatremia group was also subdivided into 2 groups, those patients having >170 mmol/L and those with 155 to 170 mmol/L. We performed Fisher exact and Wilcoxon 2-sample tests to determine if there were differences between the hyponatremia subgroups (the 121–124 mmol/L group compared to cases with sodium values <120 mmol/L) and hypernatremia subgroups (the 155–170 mmol/L group compared to those cases with values >170 mmol/L). Univariate odds ratios were calculated with the Mantel-Haenszel test to determine risk factors for mortality among patients with hyponatremia and hypernatremia. Factors significantly associated with mortality in univariate analysis were entered in a multivariate logistic regression model. Backward elimination was used to arrive to the final model. Goodness-of-fit was assessed using the Hosmer and Lemeshow Goodness-of-Fit test. A P value of ≤0.05 was defined as statistically significant. The study was approved by the Children's Healthcare of Atlanta Institutional Review Board.
RESULTS
A total of 53 099 plasma sodium tests were performed during the study period, and 702 (1.32%) fell in the study range, with 166 being ≤124 mmol/L and 536 being ≥155 mmol/L. There were 70 patients with sodium values ≤124 mmol/L, 99 patients with values ≥155 mmol/L, and 8 patients with values in both study ranges (5 with their 1st value being <124 mmol/L and 3 with their 1st value being >155 mmol/L). There were 88 patients in whom only 1 value fell in the study range, 20 with 2 sodium values in the study range, 54 with 3 to 10 values in the study range, and 15 patients with more than 11 measurements in the study range. In Figure 1, we present the number of patients alive and dead using their 1st sodium value.

* indicates that mortality was not corrected for spurious results. Mortality rate increases to 42% when the 4 patients (including a death) with spurious results are subtracted (5 deaths in 12 patients).
Although hyponatremia and hypernatremia were associated with high mortality, we could not establish a causal relationship between a specific sodium level and increased morbidity due to the underlying conditions. Table 1 presents the demographic data, diagnostic group, location, presence of other critical values, time to treatment, length of admission, and numbers dead for patients for the 4 subgroups. The mortality rate in patients with sodium values ≤120 mmol/L was 38.5%, for those patients with values ≥170 mmol/L it was 25%, while it was 14% for the other patients. However, there was no statistically significant difference for mortality. Patients with hyponatremia frequently had complications of prematurity, while patients with hypernatremia had central nervous system disorders, including head injuries, hydrocephalus, and brain neoplasias. When the 1st sodium value occurred, 53% of the patients were in an intensive care unit (ICU), and 23% were in the emergency department or operating room. There were statistically significantly more patients with sodium ≥170 mmol/L in the emergency and operating rooms (P = 0.03). The combination of sodium results in the study range and other critical laboratory results (most frequently glucose and potassium) was present in 41 patients. The presence of other critical values was significantly higher in patients with sodium ≤120 mmol/L (P = 0.03).
Demographic data, clinical diagnosis, presence of other critical values, and death rate of patients with hyponatremia or hypernatremia (N = 170)
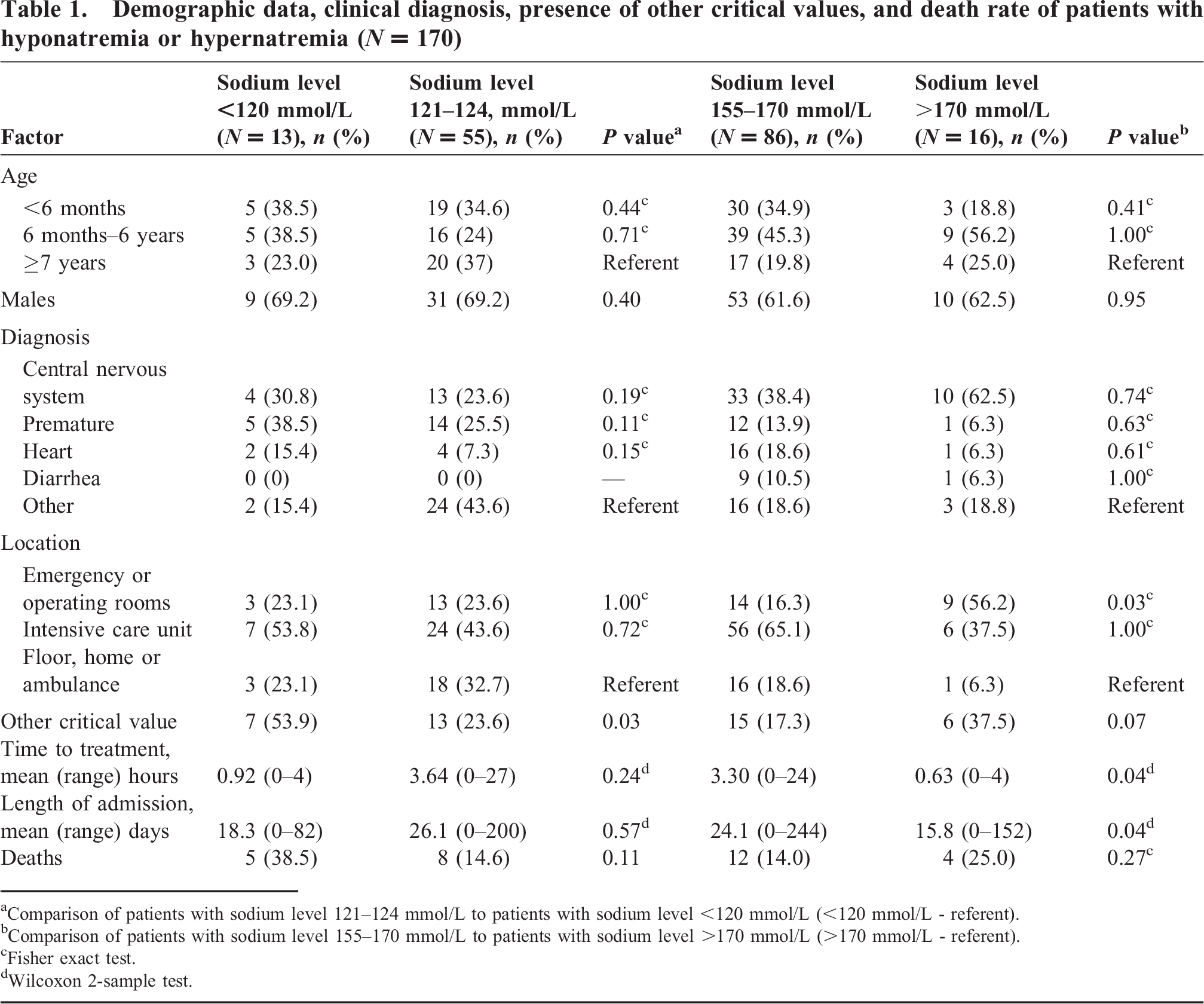
Comparison of patients with sodium level 121–124 mmol/L to patients with sodium level <120 mmol/L (<120 mmol/L - referent).
Comparison of patients with sodium level 155–170 mmol/L to patients with sodium level >170 mmol/L (>170 mmol/L - referent).
Fisher exact test.
Wilcoxon 2-sample test.
Response to treatment was instituted within 1 hour in 50% of cases and within 4 hours in 80% of cases. Six percent of patients did not appear to have had a response by a health care provider. The mean response time for critically low values (thus called to health care providers) was 55 minutes, and for the hyponatremia values that were not called because they were not critical the mean response time was 3 hours 38 minutes; however, the difference was not statistically significant. Response time for hypernatremia values between 155 and 170 mmol/L was 3 hours 18 minutes, and for hypernatremia values >170 mmol/L the response time was 38 minutes (P = 0.04). Length of stay varied from 0 to 244 days. The mean length of stay was shorter for patients with >170 mmol/L values, and the comparison of these patients to those with sodium values between 155 and 170 mmol/L was statistically significant (P = 0.04). Table 2 presents the fluids being administered when hyponatremia or hypernatremia occurred. It should be noted that most patients were receiving hypotonic intravenous solutions or were on oral or enteral fluids.
Fluids being administered when hyponatremia or hypernatremia occurred
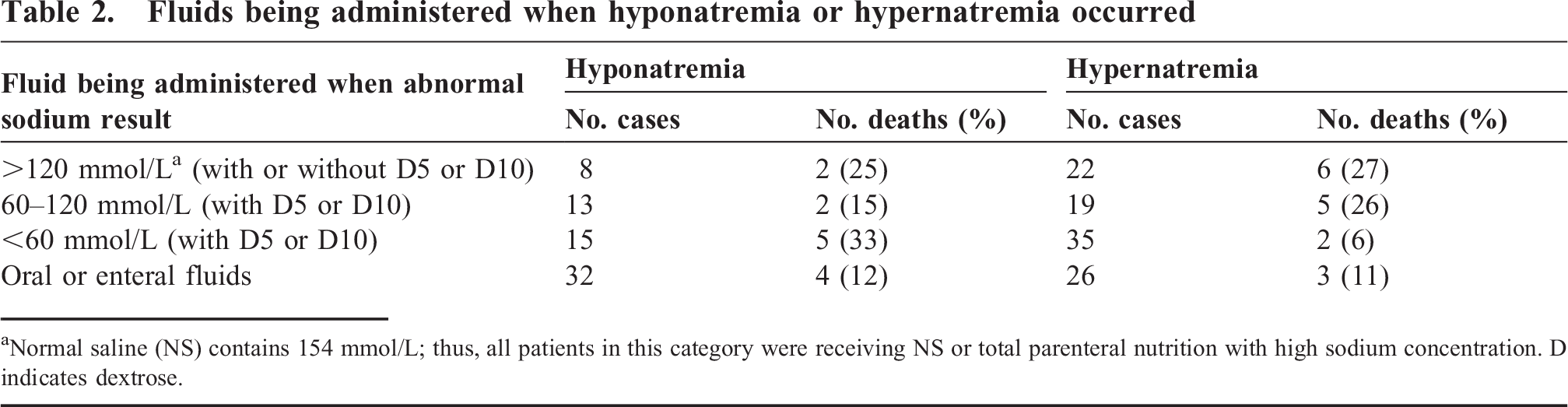
Normal saline (NS) contains 154 mmol/L; thus, all patients in this category were receiving NS or total parenteral nutrition with high sodium concentration. D indicates dextrose.
Table 3 presents the demographic data, clinical diagnosis, hospital location, presence of other critical values, and response time for the 29 patients who died. The 2 patients whose sodium derangement was most likely due to diarrhea had other preexisting conditions that could have contributed to their demise (one had Dandy Walker syndrome with sepsis and the 2nd had DiGeorge syndrome with tetralogy of Fallot).
Demographic data, clinical diagnosis, location in hospital, presence of other critical values, and response time for the 29 deceased patients
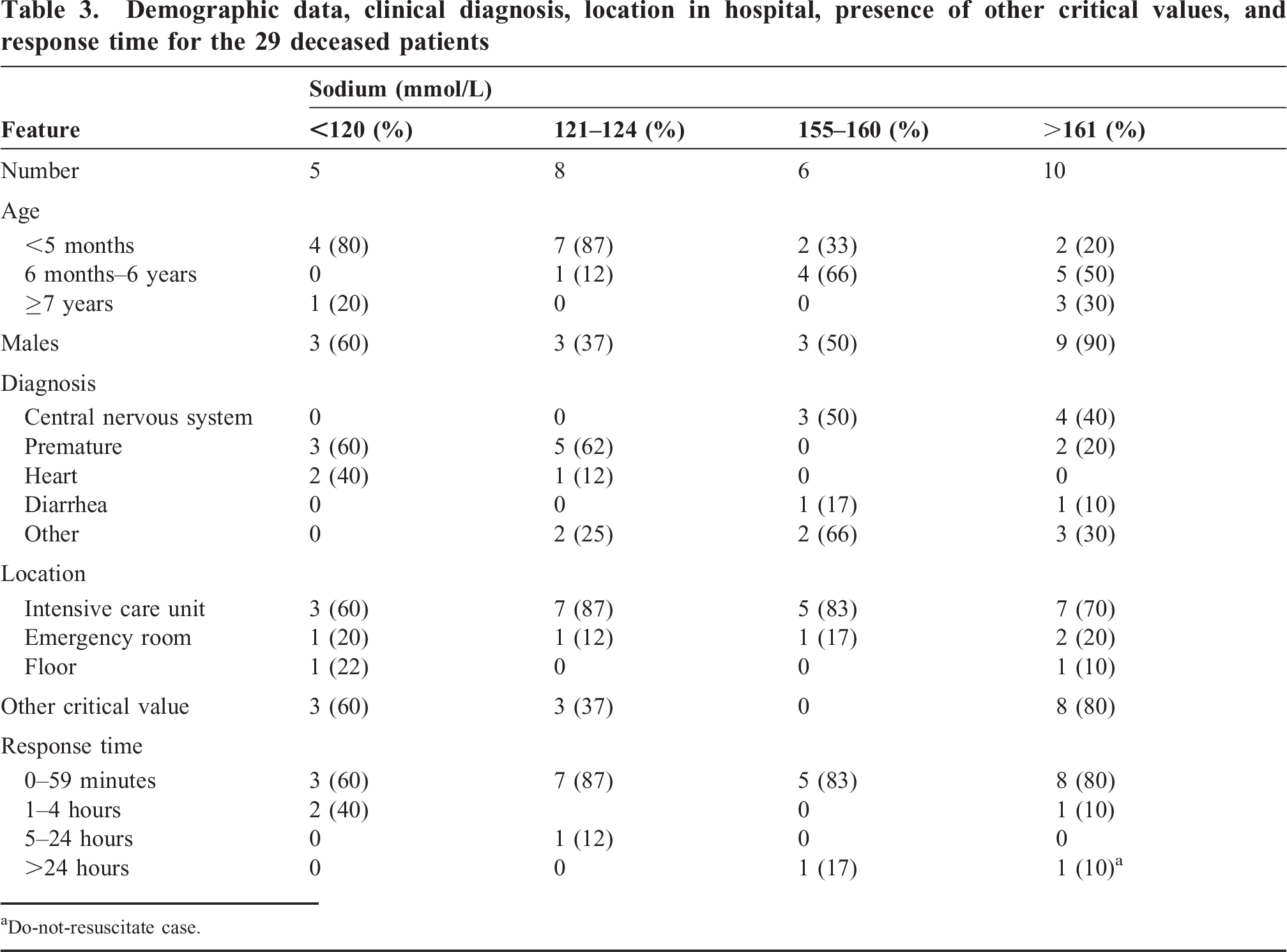
Do-not-resuscitate case.
Table 4 presents the factors that are associated with increased risk of death based on the univariate analysis. For hyponatremia, the highest odds ratio (OR; 18.62) was with children who were <6 months of age. Being premature, having a heart condition, or being in the ICU was statistically associated with death (OR of >8). For hypernatremia, the highest risk of death was associated with having other critical values (OR of 5.62). In patients with hyponatremia, shorter response to treatment was statistically associated with death (P = 0.03), while for hypernatremia, a statistically significant association was found with shorter length of stay (P = 0.002).
Factors associated with increased risk of death for hyponatremia and hypernatremia
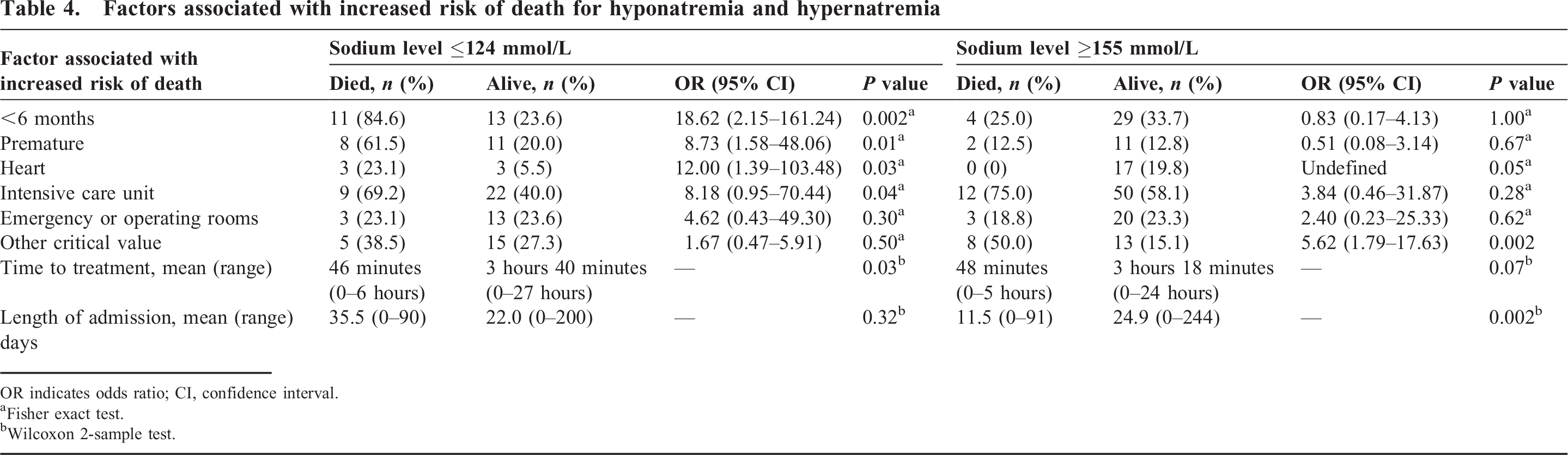
OR indicates odds ratio; CI, confidence interval.
Fisher exact test.
Wilcoxon 2-sample test.
In the multivariate analysis, when controlling for age and time to treatment, being premature or having heart anomalies was independently associated with risk of death for patients with hyponatremia (OR = 16.84; 95% confidence interval, 2.80–101.42). For patients with hypernatremia, when controlling for diagnosis, having other critical values was independently associated with death in multivariate analysis (OR = 6.19; 95% confidence interval, 1.91–20.07).
There were 28 patients in which the 1st abnormal sodium occurred within the first 30 days of life. Hyponatremia was present in 14 neonates; 8 (57%) were premature. Hypernatremia was present in 13 patients, 6 (46%) had congenital heart defects, 4 (31%) had brain problems, and 1 (8%) was premature. Mortality was 35% (5 of 14) for the neonates with low sodium and 15% (2 of 13) for those with high sodium values. One neonate had high and low sodium levels, was premature, and died. There was a statistically significant difference (P = 0.028) in mortality for neonates with plasma sodium levels in the study range compared to older patients. Except for 1 patient, all of these neonates were in an ICU (24 patients), emergency room (2 patients), or operating room (1 patient) when the abnormal sodium level occurred, with concomitant rapid response.
DISCUSSION
This analysis demonstrates that sodium levels ≤120 mmol/L and >170 mmol/L are associated with mortality above 25%. Although mortality in the other hyponatremia and hypernatremia subgroups was much lower, the difference was not statistically significant, which may be a reflection of the small sample size. Mortality rates in pediatric ICUs range between 6% and 22%, depending on the patients' diagnoses [12]. We found that risk factors associated with hyponatremia and death included being <6 months old, prematurity, having a heart condition, or being in the ICU unit, while for hypernatremia, having other critical laboratory results was associated with increased mortality. Despite this high mortality rate, a causal relationship between the abnormal sodium level and morbidity or mortality in our population could not be established because the preexisting conditions can result in similar consequences to those found with sodium derangements. In fact, the associations, particularly location and short response time, indicate that these children had extremely severe preexisting conditions that required intensive care.
We found a 38.5% mortality in children with sodium levels of ≤120 mmol/L, while the rate is 19% in adults with the same level of sodium [4]. Mortality was particularly high (35%) at any level of hyponatremia if it occurred in the first 30 days of life. In many adult patients, hyponatremia occurred as a result of hyperglycemia, which may be associated with lower mortality. In our series none of the 8 patients with hyponatremia and hyperglycemia died. The mortality risk is reversed for hypernatremia, in which case children showed a 25% mortality rate with sodium levels >170 mmol/L, compared to 47% to 75% in adults with sodium levels of >155 mmol/L [4,7].
In our patient population response to the abnormal sodium concentration occurred within 1 hour in 50% of cases and within 4 hours in 80% of cases. Even though the response time to treatment was most frequently 1 hour or less, it should be noted that for those values that were not called to the health care providers the mean response time was more prolonged. The fast response time in our study was probably due to a high percent of patients being in the ICU or the emergency department. The response rate to critical sodium values in the only adult population that has been studied [4] was 50% of cases within 4 hours. It must be noted that response times recorded may not necessarily reflect all clinical interventions, such as water restriction, which is difficult to assess in a retrospective study.
Calling critical values is a labor-intensive procedure that requires the laboratory to retest the samples, make a call to the health care provider, and document what was done, as stipulated by regulatory agencies [13]. Using percent mortality alone, the critical values could be set at ≤120 mmol/L and >170 mmol/L, even though mortality at these levels of sodium was not statistically different from lesser hyponatremia or hypernatremia values studied. What is evident from our study is that having a different set of critical values for neonates, particularly those that are premature or have heart abnormalities, should be considered because of their higher mortality. However, setting critical values becomes more complex if morbidity and sequelae are taken into consideration since researchers [14,15] have documented that in preterm neonates it is the amount of change in the levels of sodium (>8 mmol/L) that is associated with impaired neurologic outcomes.
A great amount of concern exists in the pediatric literature [16–20] regarding iatrogenically induced hyponatremia. In our patient population, being in the ICU was associated with a statistically significantly increased risk of death for patients with hyponatremia. We also found that nearly one half of hyponatremic patients were initially receiving hypotonic fluids. It is recognized that hypotonic fluids can worsen the clinical outcome [21–23]. On the other hand, hypernatremia in pediatric patients is usually caused by dehydration, and any fluid that can be administered will result in correction of the hypernatremia [24]. Hypernatremic patients in our series usually had central nervous system abnormalities that lead to diabetes insipidus or congenital heart disease that required decreased cardiac load. Vigilant attention with fluid replacement protocols needs to exist so as to avoid iatrogenically induced electrolyte disturbances.
Several limitations to this study need to be mentioned. This is a retrospective study, and complete documentation of evaluation of signs and symptoms specific to sodium derangements and all interventions was not always present in the charts. In addition, not all patients had the same array of laboratory studies performed. As a result of the complexity of these patients, determination of morbidity associated with the sodium value was very difficult. We used the 1st sodium value that was in the range studied, which may not have been the most extreme value for some of the patients. Because we studied abnormal sodium results, comparisons did not include a control group of patients with normal sodium values. Lastly, the absolute number of patients with extreme sodium derangements who died was small, restricting the multivariate analysis model to 2 to 3 variables and disallowing comparisons between deceased patients.
In summary, although sodium levels of ≤120 mmol/L and ≥170 mmol/L are associated with increased mortality in children, the difference in mortality is not statistically significant compared to that of other patients with hyponatremia and hypernatremia, and no causal relationship could be established with regard to morbidity and mortality. Univariate analysis showed that risk factors for mortality in patients with hyponatremia included being <6 months old, prematurity, heart abnormalities, and being in the ICU; for hypernatremia, increased mortality was associated with having other critical values and a shorter length of stay. Univariate analysis showed that shorter response time by health care providers was associated with mortality in the hyponatremia patients, indicating the need for urgency of treatment in these patients. Multivariate analysis showed that risk factors for death in patients with hyponatremia included being premature and having heart abnormalities, while for hypernatremia, risk factors included other critical values. This indicates that risk factors for death in hyponatremic and hypernatremic patients may primarily reflect the severity of the underlying conditions present in these children rather than the sodium derangement.