
Abstract
Postmortem examination remains the gold standard for the correct diagnosis of many diseases and for unraveling unexplained causes of death. This paper reports on the poor utilization of autopsy services and encourages parents/caregivers and practitioners to perform postmortem examinations on deceased neonates in sub-Saharan Africa. In a retrospective study, the records of 1093 neonates (653 males and 440 females, ratio 1.5:1) who died at the University of Benin Teaching Hospital and who were brought to the mortuary between 2006 and 2010 were reviewed to determine the utilization of and factors influencing postmortem examination. Sixty-two percent of the neonates died within the 1st week of life, and only 9 (0.8%) underwent a postmortem examination. Findings in the 9 postmortem studies performed on 7 males and 2 females provided additional information on the causes of death. The religious beliefs that neonates should not be subjected to postmortem study and beliefs that dead neonates are taboo and a punishment by the gods for past wrongdoings influenced 511 (46.8%) parents/caregivers to refuse postmortem analysis. The practitioners did not request postmortem study in 281 (25.7%) of the cases. The utilization of postmortem examination was marginal in this setting. We advocate the need for public enlightenment campaigns to modify the attitudes of parents/caregivers toward the postmortem study of deceased neonates. Policies should be formulated to mandate postmortem examinations of deceased neonates to enhance insight into neonatal disease, unravel unexplained causes of death, and improve the standard of neonatal care in this subregion.
INTRODUCTION
In recent decades, neonatology has evolved into a multidisciplinary independent field of medicine. It is possible to gain insights into the etiopathology of many genetic, metabolic, chromosomal, and congenital anomalies [1–3]. These insights have led to improvements in the standard of care, clinical outcome, and life expectancy of affected children. Even with the advent of modern sophisticated diagnostic facilities, postmortem examination remains the gold standard for correctly diagnosing many diseases and unraveling unexplained causes of death in neonates [4–6]. The beneficial effects of postmortem study include advising parents regarding the cause of death of their neonate, which may help them adjust to the stress of bereavement [3,7].
Despite the pivotal role that the postmortem examination plays in modern medicine, its use in neonatology is not common in many developing countries, particularly in sub-Saharan Africa, where many centers lack modern sophisticated diagnostic tools. This lack of use is a major drawback and represents a veritable source of lost vital information that is required to advance the knowledge base in the field of neonatology [6,8,9]. Although data from postmortem analysis are important for health institutions and neonatologists in formulating management strategies to improve outcomes in neonates [4,8–11], there are not many publications addressing the current utilization of postmortem examination on neonates in this African subregion.
This study retrospectively reviewed 5 years of clinical records and the mortuary pathologic day book from a Nigerian referral pediatric center to determine the utilization of postmortem study in neonates. The aim of the study was to emphasize the importance of postmortem examinations and to encourage parents/caregivers and practitioners to conduct analyses on dead neonates.
MATERIALS AND METHODS
This retrospective study included 1093 deceased neonates who were brought to the mortuary unit of the University of Benin Teaching Hospital between January 2006 and December 2010. The hospital, which is located in the Edo state in Nigeria, provides standard mortuary services to Edo and neighboring states. There was a turnaround time of 1 day for preliminary autopsy reports and 30 days for complete reports. Deceased neonates from the neonatal intensive care units, pediatric emergency department, pediatric surgical wards, and pediatric medical wards of the hospital were brought to and preserved in the mortuary unit pending collection by their parents/caregivers for formal burial. The hospital, which did not receive or preserve dead neonates from other hospitals during the study period, has a policy that requires written permission to be obtained from the parents/caregivers of deceased neonates before an autopsy can be performed. There were 6 consultants and 18 resident pathologists in the center who routinely performed complete autopsies using the modified Ghon technique, with sampling of all organs for histopathology to confirm definitive diagnoses. Cultures, radiography, or other specialized procedures were not performed. Placental specimens were not available for histologic sampling, because they were discarded from the labor wards and theater prior to the death of the neonates. Information regarding the age, sex, clinical diagnosis, factors that influenced death, and details on postmortem utilization and causes of deaths were collated from the clinical records from the Medical Records Department and the mortuary day book from the Pathology Department. Six neonates were excluded from the study because of insufficient records.
The data were analyzed using SPSS software. Continuous data were expressed as mean and standard deviations, and categoric data were analyzed using the chi-square test, with a P value ≤ 0.05 regarded as statistically significant.
RESULTS
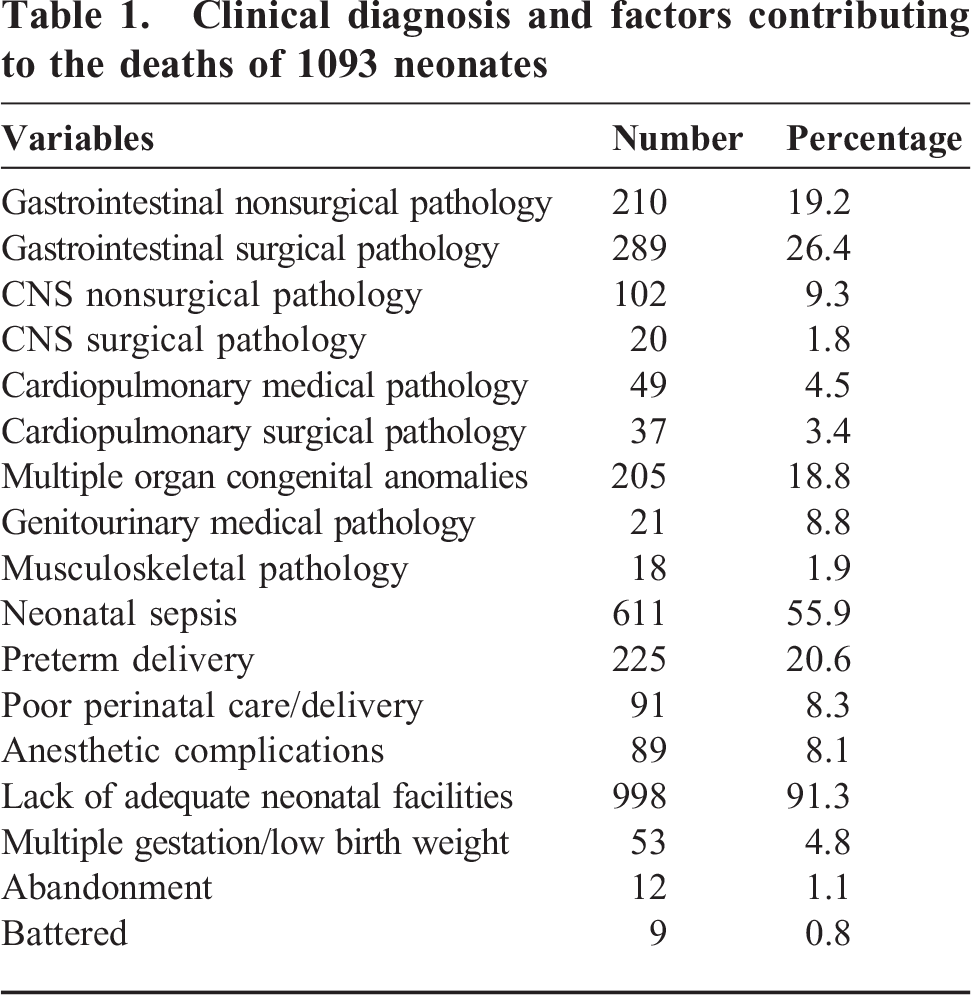
Of 4781 neonates treated over 5 years, 1093 (22.9%) mortalities were recorded. The dead neonates, consisting of 653 males and 440 females (ratio 1.5:1), were brought to the mortuary and preserved pending collection by their relatives for formal burial. There were no deceased neonates admitted to the mortuary from other health institutions during the study period. As shown in Figure 1, 682 (62%) of the dead neonates were 7 days old and younger. The mortality rate was inversely proportional to age, with 63 (6%) neonates that were at least 22 days old. Clinical causes and factors that contributed to the deaths included inadequate facilities to manage severely ill patients in 998 (91.3%) of the neonates, neonatal sepsis in 611 (55.9%), and battery in 9 (0.8%) (Table 1). Congenital anomalies involving multiple organs, particularly the heart (eg, transposition of great vessels, tetralogy of Fallot, septal defect), central nervous system (eg, spinal dysraphism, hydrocephalus), the gastrointestinal system (eg, intestinal atrasia, tracheoesophageal fistula, congenital diaphragmatic hernia, anorectal anomaly), were major surgical causes of death in 205 (18.8%) neonates.
Clinical diagnosis and factors contributing to the deaths of 1093 neonates
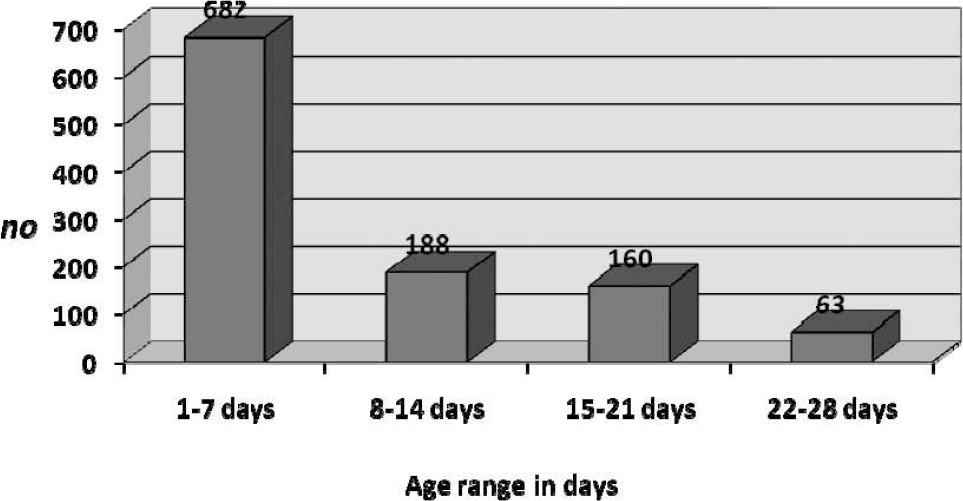
Age distribution of deceased neonates.
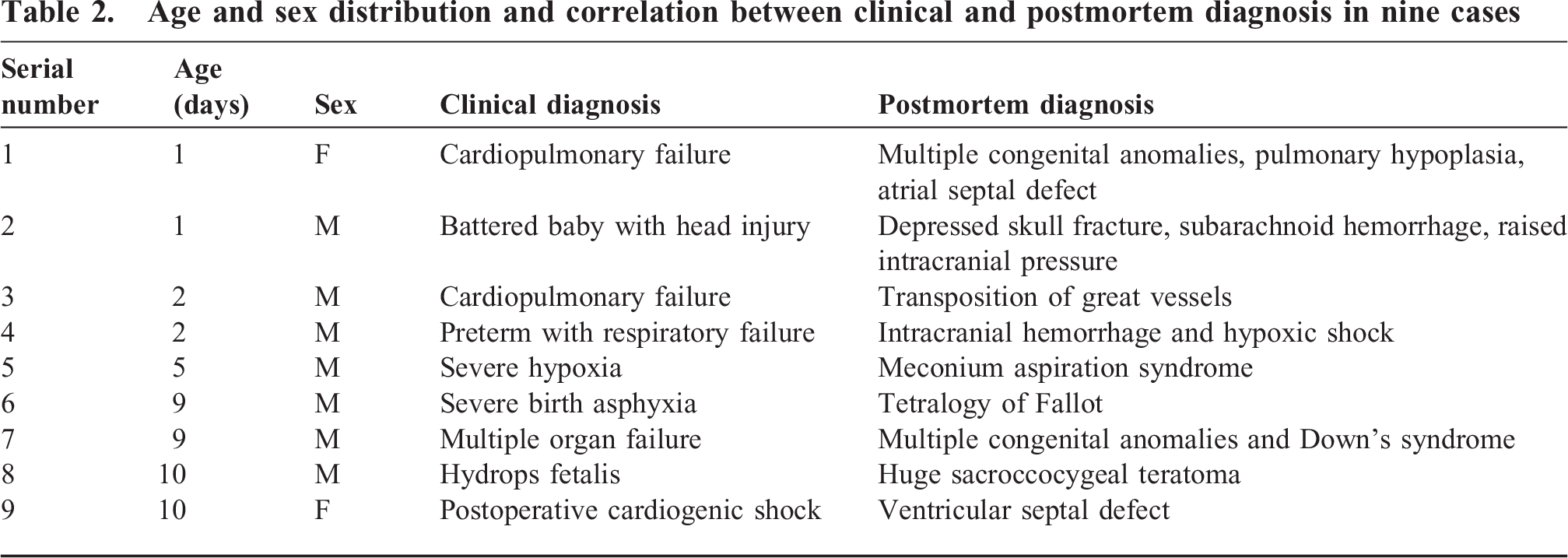
Of the 1093 deceased neonates brought to the mortuary during the study period, only 9 (0.8%), consisting of 7 males and 2 females (ratio 3.5:1), had a postmortem examination. Table 2 shows the correlation between the clinical and postmortem diagnosis of the neonates. Postmortem findings that were informative in unraveling the causes of death and clinical diagnosis of the 9 neonates included meconium aspiration syndrome, tetralogy of Fallot, transposition of great vessels, multiple congenital anomalies (VACTERL association), intracranial vascular rupture/hemorrhage, hydrops fetalis, depressed skull fracture, subarachnoid hemorrhage, and Down syndrome. The parents/caregivers of 618 (56.5%) of the deceased neonates were illiterate and from a low socioeconomic class. However, the educational levels and socioeconomic classes did not influence requests or consent for postmortem studies (P = 0.0921). The religious beliefs that neonates should not be subjected to postmortem examination and that dead neonates are taboo and a punishment by the gods for past wrongdoings were major reasons for parents/caregivers to refuse to provide informed consent for postmortem examination. Informed consent was refused by the parents/caregivers of 511 (46.8%) babies, despite requests for postmortem analysis by the attending physicians. A total of 281 (25.7%) neonates with surgical or radiologically confirmed pathologies of gut perforation, intestinal atrasia, tracheoesophageal fistula, congenital diaphragmatic hernia, anorectal anomaly, necrotizing enterocolitis, or confirmed cultures indicating neonatal sepsis (caused mainly by Staphylococcus aureus, Pseudomonas aeroginosa, Escherichia coli, Klebsiella pneumoniae, Neisseria meningitides, and K. pneumonia) and the preterm extremely low birth weight babies were not subjected to postmortem examination. The attending physicians did not request postmortem examination in these cases.
Age and sex distribution and correlation between clinical and postmortem diagnosis in nine cases
DISCUSSION
The high neonatal mortality rate of 22.9% recorded in this study, which occurred primarily in neonates who were 7 days old and younger, corresponds with previous reports in this African subregion [12,13]. Very few of the cases (0.8%) benefited from postmortem examination, which led to a massive loss of useful information regarding the possible causes of deaths that could have aided in the future management of babies with similar pathologies, as has been reported in earlier studies [3–8]. Obtaining written permission and consent was challenging because of religious beliefs and cultural influence, except for a few enlightened parents/caregivers who requested an autopsy to know the cause of death of their neonates [10]. Intense counseling and persuasion by social workers, obstetricians, and pediatricians for the more difficult clinical cases and legal requirements in the cases of battered babies led to several of the postmortem studies.
More dead male neonates (1.5:1) were brought to the mortuary, and more male neonates (3.5:1) underwent postmortem examination. This is a direct reflection of the number of male neonates treated in the study center during the period reviewed. Bodies of neonates from other health institutions were not received at the mortuary during the study period, which may have been due to the nonreferral of deceased neonates to the mortuary, inadequate mortuary space, insufficient facilities, and shortage of manpower. In this African subregion, dead neonates outside the referral center, particularly in peripheral hospitals, are not brought to the mortuary, and their deaths are usually not officially recorded. The neonates are generally buried immediately to avoid the cost of preservation in the mortuary [10,12]. These circumstances, which have also been reported by others in a similar setting, make it difficult to maintain a neonatal mortality database [10,12,13].
The lack of facilities required to manage very sick neonates, the high rate of neonatal sepsis, battered neonates, and neonates with multiple congenital anomalies (especially those involving the gastrointestinal, cardiovascular, pulmonary, and central nervous systems) were factors that significantly influenced the high mortality rate recorded in this study [12]. Postmortem findings in the 9 cases correlated with the clinical diagnosis, answered difficult clinical questions, and unraveled unexplained clinical causes of death. In the case of suspected battering, postmortem findings of depressed skull fracture, subarachnoid hemorrhage, and increased intracranial pressure assisted in confirming the cause of death when a history of battering was denied by the parent. Additionally in 1 case, postoperative cardiogenic shock that resulted in the death of a 10-day-old infant after successful repair of omphalocele minor was further explained as a ventricular septal defect after postmortem analysis. The information provided by these postmortem studies can significantly augment the knowledge base at the study center [1–11,14,16]. However, because postmortem study was not performed in the majority of cases, the causes of death were often neither confirmed nor refuted [3–5,9–11,14,15]. This lack of data constitutes a major drawback and a veritable source of lost vital information that is readily available in other cultural settings and more organized centers [6,8,9].
The usefulness of autopsy in establishing the cause of death, ascertaining unrelated diagnoses, and assisting in the grieving process was also documented by other researchers [3,4]. Perinatal autopsy has been used as a gold standard in clinical practice and provides information for genetic counseling, which is useful in the management of future pregnancies [1–5]. In this study center, however, detailed placental examination; radiography; and chromosomal, genetic, and other sophisticated postmortem studies were not feasible because of the lack of cooperation by parents/caregivers and the lack of required facilities [10,12].
The effects of religion and culture on the attitudes of parents/caregivers toward dead neonates, particularly those with congenital anomalies, are still obvious in sub-Saharan Africa [17]. Religious beliefs that neonates are not to be subjected to postmortem examination and that dead neonates are taboo and a punishment by the gods for past wrongdoings were notable factors that played prominent and determinant roles in obtaining informed consent from parents/caregivers for postmortem examination on their neonates [17]. The religious beliefs were irrespective of educational levels and socioeconomic status, because the level of parental education did not influence requests for or initiation of postmortem examination. Similar challenging experiences in obtaining informed consent for and reactions toward performing autopsies on neonates have also been reported by authors in different cultural and religious settings [18–20].
Previous studies [17,21–23] in this subregion revealed that religion, culture, ignorance, and poverty influenced the attitudes of the parents/caregivers of sick neonates toward seeking health care. These factors also increased the incidence of abandoned sick or dead neonates, especially those with obvious congenital anomalies, and the low number of postmortem studies performed on neonates. Public enlightenment campaigns targeted mainly at religious and traditional leaders, organized counseling for expectant parents/caregivers, and provision of free medical services for sick neonates and incentives for their parents were emphasized as important steps to reduce the incidence of abandoned babies and increase the rate of postmortem studies on deceased neonates [17,21–23]. Nevertheless, clinical findings at the time of death in this study were important in determining the causes of death in many neonates, which has also been reported by others [9,11,15].
In conclusion, the minimal use of postmortem examination in this African subregion resulted in a massive loss of vital information regarding the disease profiles and causes of death of many neonates. There is a need for public enlightenment campaigns to modify the current attitudes of parents/caregivers toward postmortem examination on deceased neonates. Efforts should be made by neonatologists, neonatal surgeons, and family physicians to educate designated law makers and government agencies regarding the need to formulate policies that will make postmortem examination compulsory for deceased neonates to enhance the insight into neonatal diseases, unravel the many unexplained causes of death, and improve on the current standard of neonatal care in this and similar subregions.