
Abstract
Hirschsprung disease (HD) is reported in patients with Down syndrome with a frequency between 2% and 10%. The incidence of HD is 2% in our community-based registry that contains >700 patients with Down syndrome. We reviewed rectal biopsy findings in 32 of these patients who had suction rectal biopsy performed between 1980 and 2009 to investigate the cause of chronic constipation. We confirmed that 15 patients had diagnostic histologic and histochemical features of HD. More challenging were findings in 5 of 17 patients, in whom ganglia coexisted with equivocal acetylcholinesterase reaction patterns and/or hypertrophic submucosal nerves. In this retrospective study, we were able to resolve most of these discrepant findings by demonstrating normal calretinin-positive nerve twigs in the lamina propria and muscularis mucosae. The clinical significance of these unexpected findings in suction rectal biopsy specimens that did not satisfy strict criteria for a tissue diagnosis of HD is unknown. We speculate that a minority of these patients have transition zone morphology or an incomplete/atypical form of HD. Further investigations may help resolve discrepancies that arise when suction rectal biopsy is used to investigate chronic constipation in Down syndrome.
Keywords
INTRODUCTION
Hirschsprung disease (HD), which occurs in 1 per 5000 live births, is characterized by functional obstruction and colonic dilatation proximal to a distal colonic segment that lacks ganglion cells in the myenteric and submucosal plexus [1,2]. Arrest in distal migration of enteric neurons during development is thought to be the underlying abnormality in HD. The male:female ratio of sporadic cases is 4:1, but familial/syndromic HD has reduced male predominance with transmission as an autosomal dominant or recessive trait, and familial HD more often involves the entire colon than does sporadic HD. The genetics of HD is complex; links to other genetic disorders are numerous; and multiple genes may be involved in pathways involving RET receptor–, endothelin receptor B–, and SOX10-mediated transcription [3,4]. Receptors indirectly may influence transcription but also may affect cell behavior independent of transcriptional regulation.
Down syndrome (DS), which occurs in 1 of 700–1000 live births, is a chromosomal disorder caused by the presence of all or part of an extra chromosome 21 that manifests typical facial appearance, short stature, cognitive impairment, cardiac septal and valve defects, duodenal atresia, thyroid dysfunction, leukemia, and early-onset dementia [5]. The error in meiosis responsible for most cases of trisomy 21 links to advanced maternal age. Genotype-phenotype correlation in DS has been a frustrating search to determine whether overexpression or mutation of specific genes, such as DSCR1, DRYK1A and APP, or clusters of genes on human chromosome 21 or in syntenic portions of mouse chromosomes are responsible for particular components of the phenotype [6]. Interaction between a RET enhancer and chromosome 21 is reported [7]. Recent evidence suggests that overexpression of miRNAs in trisomy 21 may result in haploinsuffiency of target proteins that contribute to the DS phenotype [8].
Numerous studies suggest that 2%–10% of patients with DS have HD [9–13], but none are population based. Despite the lack of a more precise estimate, the association is sufficient to warrant investigation for HD in any patient with DS who has chronic constipation. Among 713 patients with DS registered at the Jane and Richard Thomas Center for Down Syndrome in the Division of Developmental and Behavioral Pediatrics at Cincinnati Children's Hospital Medical Center between 1980 and 2008, 32 patients with severe chronic constipation had rectal suction biopsy (RSB), of whom 15 had HD (2%). The findings in these patients are the basis for this report.
Rectal suction biopsy specimens are convenient for reliable recognition of stigmata of HD, such as absent ganglia, hypertrophic nerves, and abnormal acetylcholinesterase (ACE) activity [14–18]. More recently, immunohistochemistry for calretinin on paraffin sections has been advocated as a alternative method for diagnosis of HD [19,20].
Recognized general pitfalls in the use of ACE to evaluate RSB for HD include technical difficulty and variability related to the age of the patient. More recently, millimeter variability in the ACE pattern in RSB from patients with HD, with or without DS was cited as a potential pitfall [19]. In that study, overall findings in DS with HD did not differ from nonsyndromatic HD, with the possible exception that some patients with DS and HD had more numerous small submucosal nerves than non-DS normal controls. We now extend those observations by comparing RSB findings in a larger group of patients with DS and chronic constipation. Those with RSB diagnostic for HD had distal colon resections; those with normal or equivocal RSB findings have been managed without surgery. We also evaluated the utility of an immunostain for calretinin applied to RSB specimens to help recognize HD in the context of DS and to resolve discrepant findings.
MATERIALS AND METHODS
The study population consisted of 15 DS patients who subsequently had an anorectal pull-through procedure for HD, 17 DS patients whose RSB specimens did not meet strict criteria for a diagnosis of HD, and published data from 26 previously reported ganglionated control specimens from non-DS patients obtained because of clinical suspicion for HD. Review of surgical pathology reports from distal colonic resections in 15 patients with DS confirmed the diagnosis of short-segment HD in each instance.
We reviewed archived slides from 35 rectal biopsy specimens, of which 32 were RSB and 3 were full-thickness rectal biopsies. At least 2 suction mucosal specimens had been obtained in most study cases. When a single specimen was submitted fresh, it was divided by a pathologist; one half was processed into paraffin, and 3 slides with 4–8 paraffin sections each were stained with hematoxalin and eosin. The paraffin sections were re-examined for this study to verify ganglia and to identify hypertrophic nerves. The frozen samples had been cut at a microtome setting of 8 μm, and 8 slides prepared with 4–8 frozen sections per slide. Abnormal acetylcholinesterase histochemistry had been performed using the method of Lake [14]. A representative frozen section stained for ACE from each specimen was selected based on orientation, representation of the full depth of the specimen, and technical quality. Abnormal acetylcholinesterase histochemical activity was evaluated, 1 mm at a time, as previously described, for abnormal distribution and intensity of the staining reaction in nerve twigs of the lamina propria and muscularis mucosae, for excess numbers of small submucosal nerves defined as >3 small nerves per linear mm of biopsy specimen, and for presence of large (>35 μm) submucosal nerves [15]. Minimum transverse diameter of submucosal nerve profiles was assessed using a calibrated ocular. For the purpose of calretinin immunohistochemistry (IHC), archived paraffin blocks were recut or (if the tissue was inadequate) frozen tissue was re-embedded in paraffin. Calretinin IHC was performed using a primary antibody obtained from Cell Marque (Austin, TX, USA) using DAKO methodology at a dilution of 1/2000. The calretinin-immunostained sections were evaluated for reactive terminal nerve twigs in the lamina propria and muscularis mucosae and for submucosal neurons. Two DS/HD biopsy specimens and 6 controls were excluded from the calretinin analysis because insufficient tissue remained in paraffin to perform calretinin IHC or because the specimen contained anal mucosa.
Three pathologists independently reviewed the hemotoxylin and eosin, ACE, and calretinin IHC slides and for each technique scored the case as HD, not HD, or equivocal. The primary criterion for a diagnosis of HD at this institution for the duration of this study has been absent ganglia in the submucosa, supported by unequivocally abnormal ACE histochemistry. We verified the presence of hypertrophic submucosal nerves, a feature that supports a diagnosis of HD or HD transition zone, by direct measurement; submucosal nerves with a short diameter of ≥35 μm were classified as hypertrophic. We assessed one other useful diagnostic feature, the presence (normal) or absence (abnormal) of calretinin-reactive nerve twigs in the lamina propria and muscularis mucosae in most cases, depending on availability of tissue in archived blocks. We also assessed the frequency of linear segments of submucosa with >3 small nerves/mm, a finding that we had previously observed with increased frequency in RSB that met strict criteria for HD in patients with DS. After independent reviews, equivocal findings were adjudicated by consensus and assigned to the following categories: HD, not HD, or equivocal/? transition zone morphology.
The study was conducted in accordance with federal patient privacy regulations and with approval from the hospital's institutional review board.
RESULTS
The incidence of HD is 2% (15/713) in our comprehensive community-based local registry that contains a much larger number of patients with DS than any series previously reported. Four percent (32/713) of our registered patients with DS had chronic constipation of unknown etiology but of sufficient severity to prompt an investigation for possible HD. Fifteen of these patients (2%) had diagnostic histologic and histochemical features of HD and subsequently had short-segment HD diagnosed in resection specimens from the distal colon. The cause of severe chronic constipation in the other 17 patients with DS was not determined.
Eleven of the 15 patients with DS and HD were diagnosed at <3 weeks of age, which is comparable to age at diagnosis of HD in non-DS patients at our institution. The median age for diagnosis of HD in DS was 7 days and for non-HD in DS was 5 months, based on the clinical presentation and findings in RSB. However, diagnosis of HD was delayed until age 2 months, 7 months, 27 months, and 8 years in the other 4 patients with DS. The mean age at rectal biopsy in patients with chronic constipation whose biopsies were not diagnostic for HD was older in DS controls (642 days) and in previously reported non-DS normal controls (572 days).
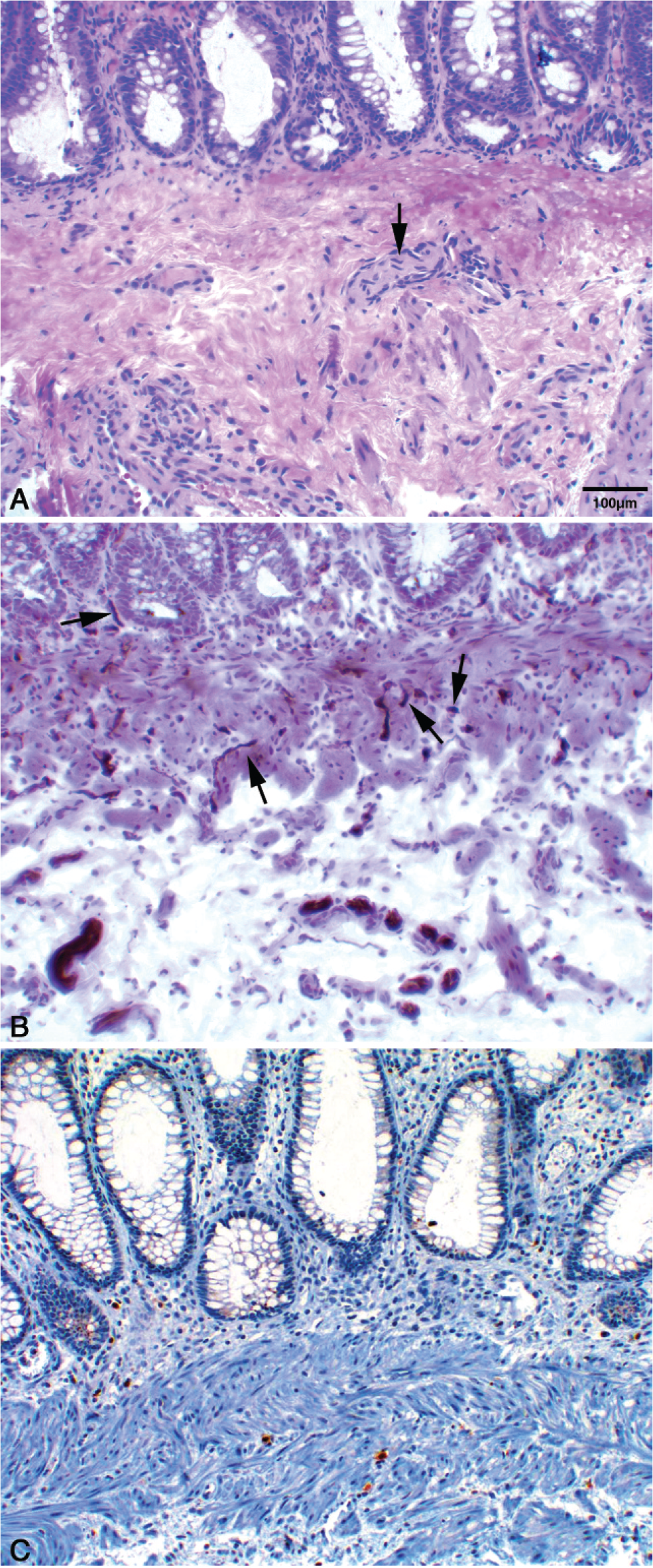
The detailed findings in RSB specimens in DS/HD and DS/non-HD are provided in Tables 1 and 2, respectively. All 15 patients with DS and HD lacked submucosal ganglia. Eleven of these 15 patients had an abnormal ACE pattern, 2 had an equivocal reaction, and 2 had a normal ACE reaction. In 1 of the latter patients, a 5-day-old infant, the ACE histochemistry was normal; however, no ganglia were found, hypertrophic nerves were present, and calretinin-positive nerve twigs were absent from the lamina propria and muscularis mucosae (Fig. 1). In the other patient with normal ACE histochemistry, a diagnosis of HD was based upon absent ganglia in conjunction with hypertrophic nerves. In the 2 oldest patients, a second RSB was performed. In 1, a 27-month-old child, the ACE was inconclusive in the first specimen and abnormal in the second; hypertrophic nerves were present in both specimens. Calretinin-positive nerve twigs were subsequently determined to be absent in the lamina propria and muscularis mucosae of both specimens. In the second instance, lack of submucosa in the first specimen from an 8-year-old child prompted a second biopsy, despite abnormal ACE reactivity in the muscularis mucosae; the second specimen contained a hypertrophic nerve in the submucosa. Subsequent calretinin IHC was abnormal in both specimens.
Rectal biopsy findings in Down syndrome with Hirschsprung disease
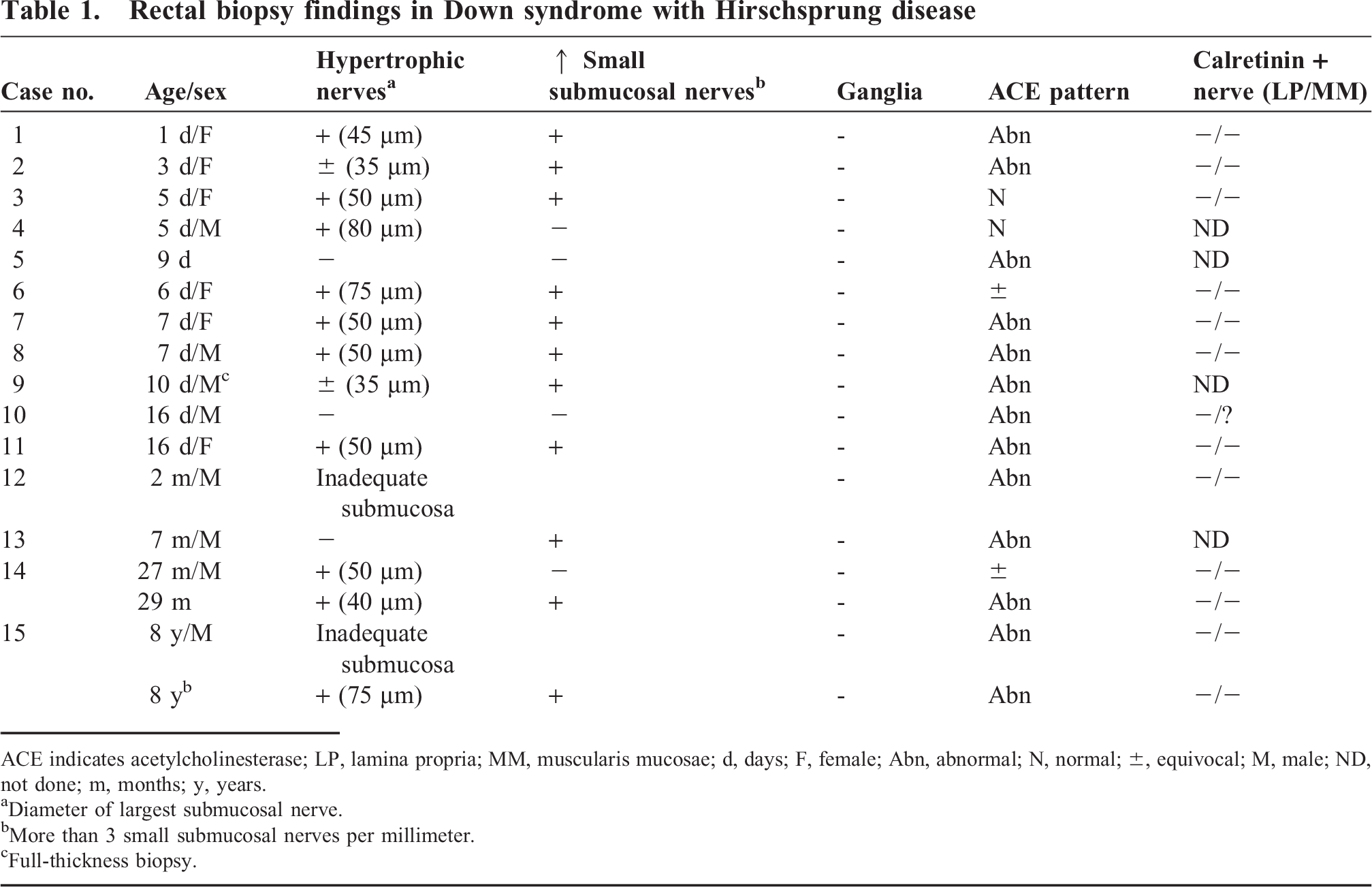
ACE indicates acetylcholinesterase; LP, lamina propria; MM, muscularis mucosae; d, days; F, female; Abn, abnormal; N, normal; ±, equivocal; M, male; ND, not done; m, months; y, years.
Diameter of largest submucosal nerve.
More than 3 small submucosal nerves per millimeter.
Full-thickness biopsy.
Rectal biopsy findings in Down syndrome without Hirschsprung disease
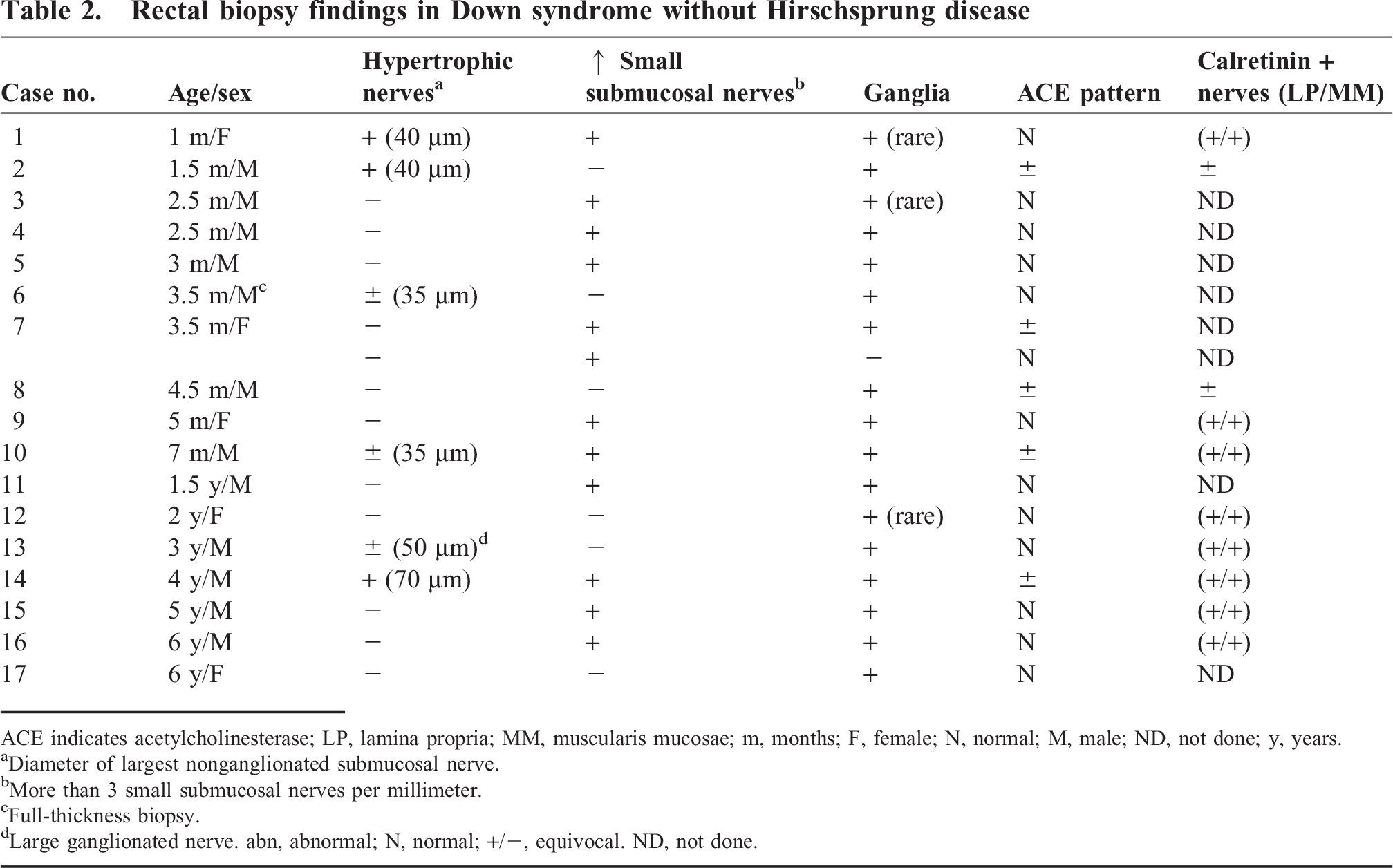
ACE indicates acetylcholinesterase; LP, lamina propria; MM, muscularis mucosae; m, months; F, female; N, normal; M, male; ND, not done; y, years.
Diameter of largest nonganglionated submucosal nerve.
More than 3 small submucosal nerves per millimeter.
Full-thickness biopsy.
Large ganglionated nerve. abn, abnormal; N, normal; +/–, equivocal. ND, not done.
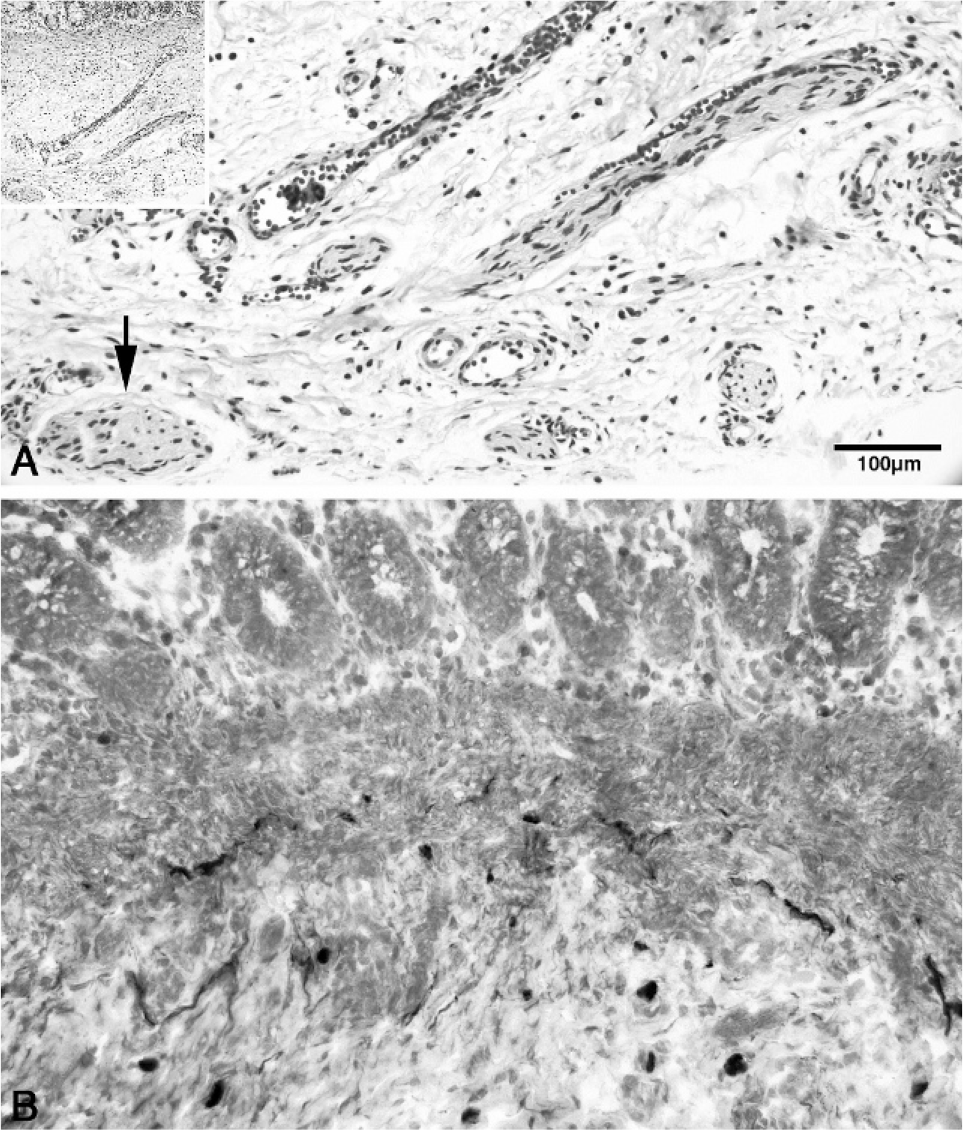
Hirschsprung disease, Table 1, case 3.
Inconclusive ACE patterns (Figs. 2,3) were associated with lack of ganglia and hypertrophic nerves in 2 patients. Both samples lacked calretinin-reactive nerve twigs in the lamina propria and muscularis mucosae, typical for HD.
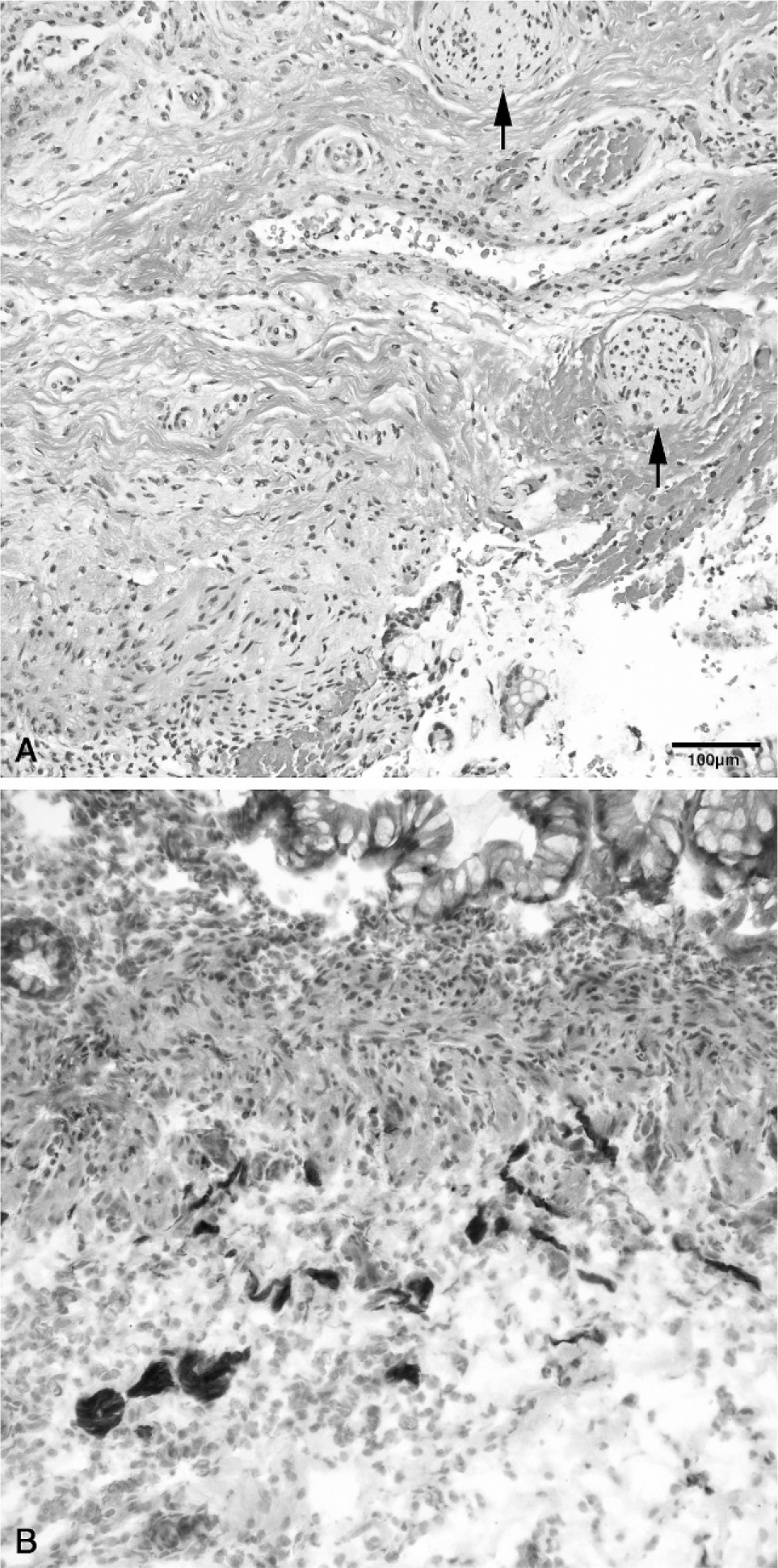
Hirschsprung disease, Table 1, case 6.
Hirschsprung disease, Table 1, case 14.
Large (≥35 μm) submucosal nerves in minimum transverse diameter were more frequent in RSB from patients with DS and HD than previously reported from this institution in nonsyndromic HD (80% vs 54%). However, the difference was not statistically significant and is probably related to variation in depth of biopsy.
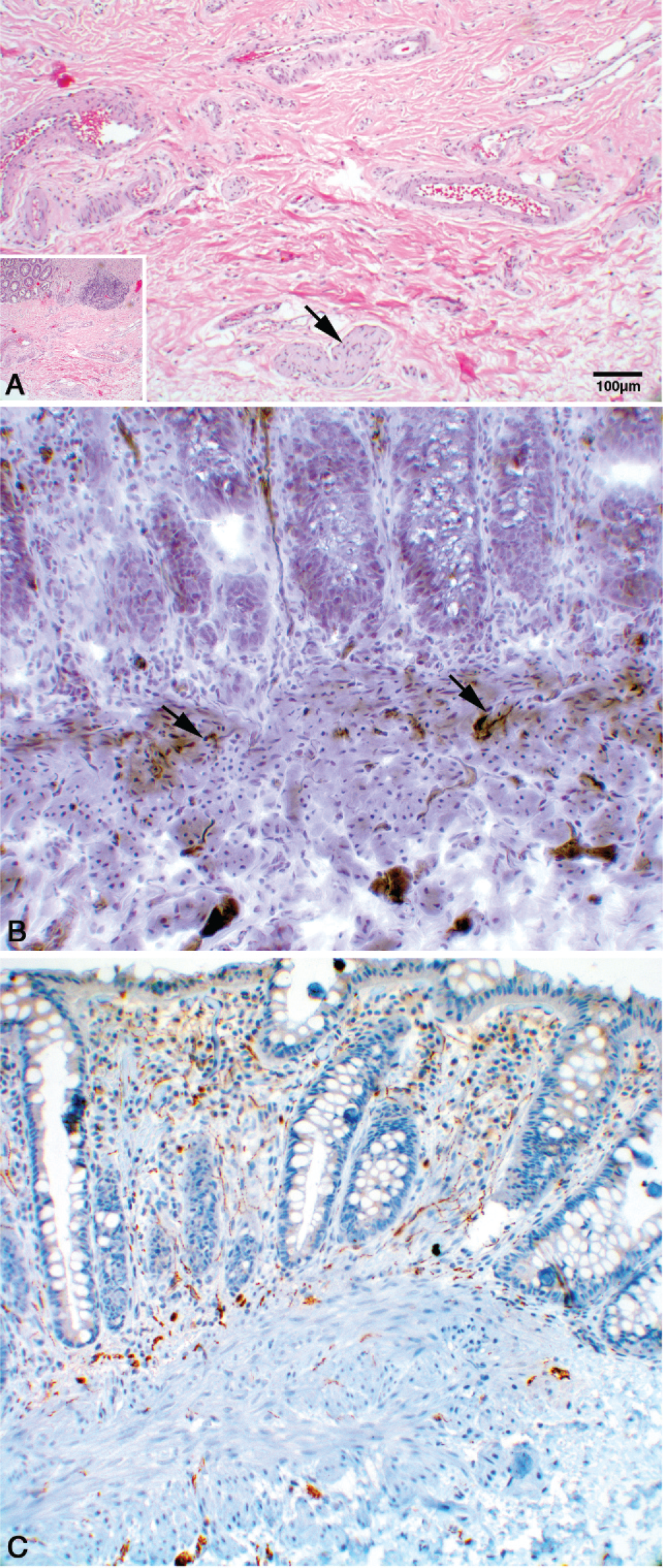
The RSB findings in 17 DS patients with chronic constipation who were not considered to have HD are listed in Table 2. Included in this group are many specimens that presented diagnostic dilemmas. Only 9 specimens met strict criteria for excluding HD; ganglia were rare in 3 of these specimens. One adequate specimen with only 1 gangion also had a single hypertrophic nerve, but the ACE histochemistry and calretinin IHC were normal (Fig. 4). Large (≥40 μm) submucosal nerves, including 3 instances that were unequivocally hypertrophic, were identified in 6 of 17 specimens, all of which contained ganglia; the ACE reaction was equivocal in 3 of these 6 specimens. These variable inconsistencies, in retrospect, were resolved by the finding of normal calretinin-reactive nerve twigs in the lamina propria and muscularis mucosae of 3 specimens (1, 10, and 13) with normal ACE patterns and hypertrophic nerves. One specimen from an older patient with an equivocal ACE reaction and hypertrophic nerves had what we regard as an unusual plethora of calretinin-positive nerve twigs in the lamina propria (Fig. 5A-C). The calretinin reaction was atypical in 2 ganglionated specimens in that no nerve twigs were demonstrated in the lamina propria or muscularis mucosa, whereas submucosal ganglia were reactive, although weakly so.
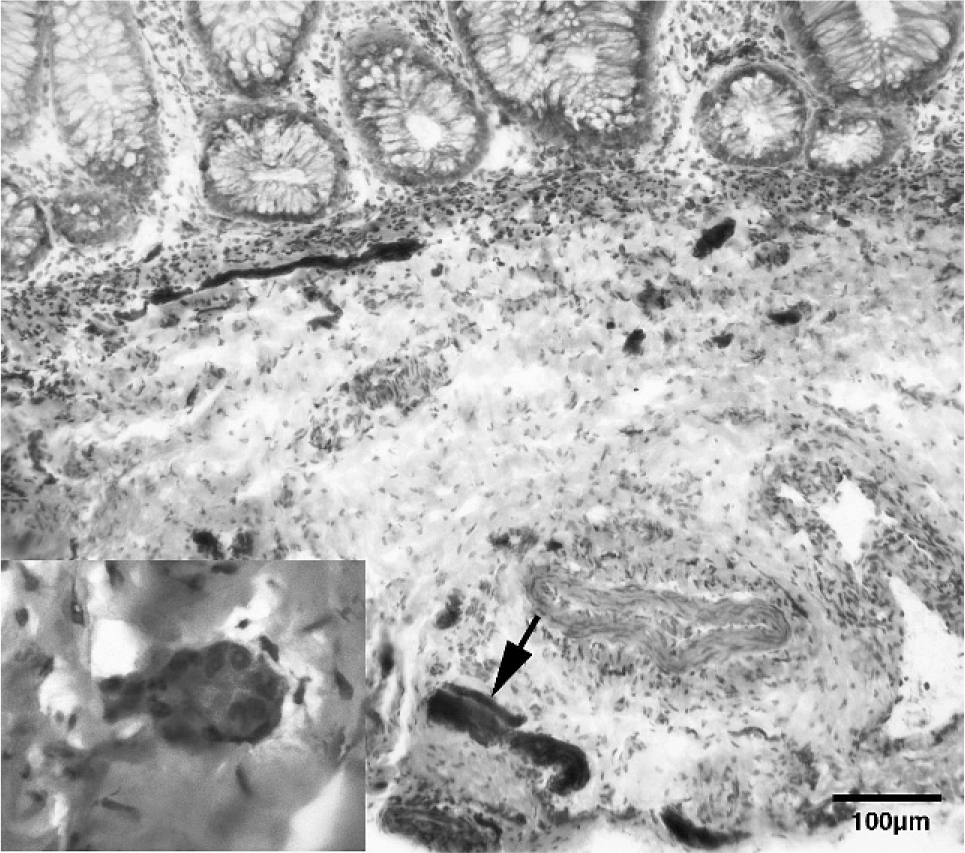
Not Hirschsprung disease, Table 2, case 1. Minimum diameter of the hypertrophic nerve in deep submucosa (arrow) is 35 μm. This representative histochemical reaction identifies numerous small submucosal nerves, including several intensely stained small nerves in close contact with the muscularis mucosae. Small nerve twigs in the muscularis mucosa and lamina propria were rare and delicately stained. Although worrisome for Hirschsprung disease, ganglia were present in the submucosa (inset, H&E, ×400) and the reaction was interpreted as normal. Acetylcholine esterase, ×200.
Not Hirschsprung disease, Table 2, case 14.
The borderline abnormal/equivocal ACE pattern in 5 of 17 non-HD ganglionated specimens was characterized by a mixed pattern of a few normal delicate twigs in the muscularis mucosae intermixed with a few coarse heavily stained ACE-positive nerve twigs entering the muscularis mucosae. This pattern resembles the least frequent pattern in our previous normal series and is difficult to distinguish from a relatively uncommon focal pattern in HD (pattern B), as previously described by Pacheco and colleagues [19]. Twelve of 17 RSB samples listed in Table 2 from DS patients who lacked diagnostic morphologic evidence for HD had at least 1 linear mm of biopsy sample with prominent ACE-reactive small nerves and nerve twigs, often limited to the junction of the submucosa and muscularis mucosae. We interpret this feature as a normal variant that has no particular significance for DS, because it was no more frequent than we previously reported in non-DS normal control RSB.
Interpretation of such equivocal ACE reaction patterns is always problematic but is particularly so when found throughout a RSB specimen.
DISCUSSION
Hirschsprung disease is observed in DS patients with a frequency between 2% and 10% [9–12]. Conversely, 0.8% of individuals with HD are estimated to have DS [13]. Fifteen of 32 patients who had RSB performed to investigate the cause of chronic constipation in our registry population (2%) had diagnostic histologic and histochemical features of HD. The cause of severe chronic constipation in the other 17 patients with DS was not determined.
Our institutional experience with RSB in investigation for HD is that most RSB, if adequate in size and location, are readily classified as normal or abnormal by combining lack of ganglia with abnormally enhanced ACE histochemical activity, as judged by experienced pathologists [17,21]. Our findings in this study reconfirm the morphologic similarity between sporadic HD and HD in DS. However, we found many troublesome features in this retrospective review that may cause diagnostic difficulty in patients with DS and chronic constipation whose RSB contain ganglia. We observed an unexpectedly high frequency of 2 findings in nondiagnostic RSB from patients with DS. Equivocal patterns of ACE activity and/or isolated borderline or unequivocally hypertrophic nerves were seen in the muscularis mucosa or submucosa respectively of 6 or 17 patients with DS whose specimens did not satisfy strict criteria for a tissue diagnosis of HD. These findings coincided in 3 patients and, in retrospect, are suspicious for transition zone morphology. The calretinin IHC pattern was normal in 8 of 10 of cases in which there was sufficient material for testing remaining in the paraffin block, including 3 of 5 patients whose RSB are, in retrospect, suspicious for transition zone morphology, either because of borderline or unequivocally hypertrophic submucosal nerves or equivocal ACE histochemistry. In the other 2 patients with inconclusive RSB findings, calretinin IHC was weaker than expected and difficult to interpret, probably for technical reasons.
Larger-than-normal nonganglionated submucosal nerves are a useful marker for HD, but strict criteria must be used for this feature to be reliable. The upper limit of normal diameter is reported to be 35 μm [16]. A single nonganglionated nerve or a ganglionated nerve that only slightly exceeds this measure may or may not be abnormal. Our experience with measuring submucosal nerves in frozen sections [19] supports a previous finding that submucosal nerves >40 μm in diameter are probably abnormal [20]. However, the relatively small numbers of cases previously studied, the difficulties of measuring diameter of obliquely section nerves, and the shrinkage factor of approximately 20% associated with paraffin embedding are serious concerns. We recommend that submucosal nerves 35–50 μm in diameter, lacking neurons, in either frozen or paraffin sections should raise suspicion. In a RSB performed because of suspicion for HD, one submucosal nerve with a diameter of ≥50 μm in a paraffin or frozen section is a reliable indicator of abnormal innervation.
A significant number (7/17) of our DS patients without HD were biopsied beyond 1 year of age, compared with only 2 of 15 patients with HD. Equivocal findings in the older patients in both groups do not seem to be related to age at biopsy in either group, but the numbers are small. However, anecdotal experience suggests that difficulties are more common in RSB from older children. Age of the child at the time of biopsy influences at least 1 of the 4 parameters that contribute to a diagnosis of Hirschsprung disease, that is, the concentration of nerve twigs with excessive ACE activity in the muscularis mucosae and possibly in the lamina propria, although the latter is less certain. In very young infants with HD, the large number of abnormal nerve twigs in the muscularis mucosae is often spectacular, whereas the number of strongly reactive nerve twigs in the lamina propria is usually not impressive. The opposite tends to occur in many older patients with HD. Regardless of whether age influences the frequency of diagnostic hypertrophic nerves, the criteria for designating a given nerve as hypertrophic or the concentration of ganglia remain uncertain.
Calretinin, a calcium-binding protein, stains ganglion cells of the submucosal and myenteric plexus and nerves in all regions of the human gastrointestinal tract, including delicate terminal nerve twigs that project into the mucosa. In 2004, Barshack and colleagues [22] showed absent calretinin immunoreactivity in enteric nerves in the lamina propria of aganglionic resection specimens. Most recently, Kapur and colleagues [21] in a comprehensive study concluded that calretinin IHC appears to be a reasonable alternative to ACE as an adjunctive diagnostic method for evaluating RSB for HD. In our patients with DS and chronic constipation, normal calretinin IHC reactivity usually coincided with the presence of ganglia and a normal ACE reaction. Furthermore, calretinin IHC helped to resolve diagnostic issues posed by hypertrophic submucosal nerves or equivocal patterns of ACE reactivity in most specimens in which adequate tissue remained in the block for testing. However, 2 patients with ganglia had equivocal ACE reactions and lacked calretinin -positive nerve twigs in the lamina propria and muscularis mucosae. Weaker-than-expected reactivity in cytoplasm of ganglia was observed in these 2 patients. This discrepancy may have been technical rather than substantive. An alternative possibility is that both the cholinergic and the calretinin-related components of the autonomic nervous system in the colon of some patients with DS may be abnormal.
Whether calretinin IHC can be relied upon to distinguish normal from abnormal in RSB that contain transition zone is not entirely clear; additional careful studies of the transition zone in resection specimens would help to place the calretinin IHC on a more secure footing as a diagnostic tool for this purpose.
Our experience with DS rekindles vexing questions. What is the most efficient algorithm for evaluating a RSB for HD and how should that approach be modified in the face of equivocal or conflicting results? Two of the 4 features that support a diagnosis of HD (absence of ganglia and presence of submucosal hypertrophic nerves) are contingent upon sample size and depth, a quality in RSB specimens that may be elusive in older children. Both ACE histochemistry and calretinin usually yield decisive results on superficial specimens that include only muscularis mucosae and lamina propria.
For 3 decades, we have divided specimens for frozen sections and paraffin sections and used a relatively small number of paraffin sections, relying mainly on identification of ganglia plus the ACE reaction in frozen sections to classify as normal or abnormal. This approach severely reduces the number of cases in which the responsible pathologist has chosen to order exhaustive sectioning of the paraffin block. Although not without pitfalls, substantial technician and pathologist time is conserved. Persistent uncertainty indicates the need for a repeat biopsy.
Committing entire specimens to paraffin, as many others prefer, followed by routine exhaustive sampling may produce similar results but eliminates one very useful source of diagnostic information: ACE histochemistry. Calretinin IHC is very useful to those who choose to rely on paraffin sections.
We propose that there is a place for a prospective study to evaluate the cost and benefits of the 2 approaches in RSB specimens that are deemed large enough to divide. In such a study, one would assess frozen sections for ganglia, ACE activity, and size of submucosal nerves. In addition, on would perform a parallel assessment in paraffin sections using calretinin IHC in the first few sections to guide the decision whether to stain and examine all remaining precut sections from the exhausted paraffin block.
Our findings in RSB of patients with DS and chronic constipation who lacked diagnostic features of HD suggest that a significant minority of these children have one or more features usually associated with HD or transition zone morphology, namely hypertrophic submucosal nerves and borderline abnormal ACE reactions in the muscularis mucosae. The role of such features in chronic constipation in children with DS, if any, remains to be determined. However, we conclude that the presence of ganglia in the distal rectum of a patient with DS and chronic constipation may be insufficient to exclude a HD-like disorder, in the presence of even one hypertrophic nerve. We further caution that it is necessary to actually measure the diameter of submucosal nerves to reliably identify those that are hypertrophic using a minimum short diameter of 50 μm as a confident marker of hypertrophy based upon our own experience and that of others who had previously presented data indicating that nerves with a diameter of 35 μm top the normal range [16]. An equivocal ACE reaction in the presence of ganglia always should stimulate further search for hypertrophic submucosal nerves.
Our experience suggests that RSB performed to investigate chronic constipation in DS are more often inconclusive than ganglionated RSB obtained from patients who do not have DS, as previously reported from our institution. To further investigate the cause of chronic constipation in DS patients when RSB is inconclusive for HD, we propose that patients with DS and chronic constipation who exhibit one or more features of transition zone morphology in the presence of ganglia are candidates for rebiopsy at multiple levels of the rectum. Suspiciously large submucosal nerves should be measured. Calretinin IHC should be performed. Anorectal manometry should be considered. To provide more data on prevalence and extent of transition zone morphology, or other abnormal features in DS, we suggest that colectomy specimens from patients with DS and HD be carefully compared with resection specimens from sporadic HD, including a detailed assessment of the calretinin-linked component of the autonomic nervous system.
The relatively high frequency (minimum 2%) of a disorder that meets clinical and morphologic criteria for HD in patients with DS (the HD phenotype) does not mean that the underlying pathobiology is identical to that of sporadic or familial HD. Indeed, the molecular abnormalities defined in non-DS–associated HD show minimal overlap with the genetic abnormalities in DS as currently known. Our morphologic data suggest that a HD-like disorder may exist in more children with DS than can be ascertained by application of traditional morphologic criteria to a distal RSB. In this regard, clinical follow up in our patients with DS who lacked diagnostic features for HD would obviously be of great interest.
In summary, in DS, the diagnosis of HD in a RSB is usually straightforward. However, in ganglionated specimens from patients with DS, hypertrophied submucosal nerves are often encountered and the number of small ACE-reactive nerve twigs in the muscularis mucosae is often at the upper normal limit and may include focally intense ACE activity in a few nerve twigs, a feature that overlaps with findings in HD. In this retrospective study of patients with DS and chronic constipation, a minority of RSB that were originally classified as non-HD have findings that in retrospect are suspicious for transition zone or for a related disorder or imbalance of the autonomic nervous system. In retrospect, we were able to partially resolve concern in many problematic RSB specimens by demonstrating normal calretinin-positive nerve twigs in the muscularis mucosae and lamina propria. Although a legitimate question persists about the utility of calretinin IHC in the transition zone, our experience extends to patients with DS the general conclusion of Kapur and colleagues [21]: the sensitivity and specificity of calretinin IHC in children with HD may be equivalent to ACE histochemistry, and calretinin IHC may be informative in rectal biopsy specimens with equivocal ACE histochemistry or when inadequate tissue is available to establish a hemtoxylin and eosin–based diagnosis of absent submucosal ganglia.