
Abstract
To examine the clinicopathologic correlations of three histological patterns of diffuse chronic hypoxic placental injury (preuterine [PR], uterine [UH], and postuterine [PU]), a retrospective statistical analysis of a large 14-year placental database was performed. Of 5097 placentas between 20 and 43 weeks of gestation examined consecutively, 4413 did not feature histological chronic placental hypoxia, while 684 did. In the latter, maternal hypertensive disorders, diabetes mellitus, abnormal cardiotocography and Dopplers, cesarean sections, inductions of labor, and fetal growth restriction, as well as other placental hypoxic lesions and decidual arteriolopathy, were statistically significantly more common than in the remaining placental material. Two hundred eighty-nine PR cases featured the most advanced gestational age and meconium staining; 237 UH cases featured severe preeclampsia, decidual arteriolopathy, villous infarction, membrane laminar necrosis, microscopic chorionic pseudocysts, excessive extravillous trophoblasts, and maternal floor multinucleate trophoblastic giant cells; and 158 PU cases featured the lowest placental weight and the highest prevalence of abnormal Dopplers, umbilical cord compromise, fetal growth restriction, cesarean section rate, and complicated 3rd stage of labor. The specificity of chronic hypoxic patterns of placental injury was much higher than the sensitivity, with the highest specificity for an excessive amount of extravillous trophoblasts. Diagnosing various hypoxic patterns of placental injury by histology may help to clarify the etiopathogenesis of a significant proportion of complications of pregnancy and abnormal fetal or neonatal outcomes. The patterns should help to retrospectively diagnose placental hypoxia, even in clinically unsuspected cases.
Keywords
INTRODUCTION
While acute focal placental hypoxia manifesting as placental infarction is well recognized, there is no universally accepted system of histological classification of patterns of diffuse (global) placental injury. The terms “ischemic change” [1,2] and “maternal vascular under-perfusion” [3,4] are commonly used by various authors, but definitions of these terms are sometimes vague. More specific descriptions, such as distal villous hypoplasia (terminal villous deficiency) [2], distal villous immaturity [3], chorangiosis [5], agglutinated terminal villi [3], increased number of implantation site trophoblasts (placental site giant cells) [4,6], increased number of immature proliferative intermediate trophoblasts [3,7], increased number of extravillous trophoblasts in placental membranes [8] and chorionic disc [9], microscopic chorionic (pseudo)cysts [8,10,11], increased syncytial knotting (Tenney-Parker change) [1,12,13], deficiency of vasculosyncytial membranes [14,15], excessive number of villous cytotrophoblasts [16,17] and Hofbauer cells [16,17], and villous fibrosis [16–18], have been frequently linked to specific conditions of high-risk pregnancy known to be potentially complicated by or caused by chronic in utero hypoxia. Although such histological lesions as maternal decidual arteriolopathy or choriodecidual hemosiderosis may indicate the etiology of placental hypoxia, they are not always clearly separated from their placental sequelae such as acute and chronic placental injury, adaptive changes in the placenta, or fetal hypoxia.
For several years, the present author has been using three terms to make a placental diagnosis: the preuterine (PR), uterine (UH), and postuterine (PU) patterns of chronic hypoxic placental injury [19–21]. However, the clinical correlations of the diagnoses have never been summarized. The aim of this analysis is to study this in a large placental material.
MATERIALS AND METHODS
This is a retrospective analysis of 5097 placentas (≥20 weeks and < 43 weeks) consecutively examined by the author over the period of 14 years. The placentas were submitted for examination because of a high-risk pregnancy, fetal distress, poor condition of the neonate, operative delivery, or gross placental abnormalities. Placental examination was performed according to generally accepted criteria [1,2,12,13,16,22]. Specifically, two sections of placental membrane roll, umbilical cord, and at least two paracentral full-thickness chorionic disc sections were routinely obtained as a part of the placental examination if no gross lesions were identified. All grossly seen lesions were also sampled. The samples were fixed in buffered formalin, followed by routine paraffin embedding, cutting, and staining with hematoxylin and eosin. Definitions of clinical conditions and placental lesions conformed to those described elsewhere and the author's previous publications [1,2,4,6,8,9–13,16,22,23]. In addition to standard terminology for placental lesions, diagnoses of PR, UH, and PU were rendered on histological grounds, based on the examination of paracentral sections of grossly unremarkable placental tissue according to the algorithm presented in Figure 1. The type of placental maturation (homogeneous vs heterogeneous), its consistency with gestational age (hypomature or hypermature), and villous vascularity are the keystones of this approach, but such histological features as density and proliferation of villous cytotrophoblastic cells, excessive syncytial knotting (Tenney-Parker change), amount of villous extracellular matrix, and number of Hofbauer cells are also helpful [17]. Examples of the three patterns of chronic placental hypoxic injury and comparisons with a normal same-gestational-age placenta are illustrated in Figure 2. Selected maternal, fetal and neonatal, and gross and microscopic placental features were statistically compared between the diffuse chronic hypoxia group (study group, SG) and the rest of the material (comparative group, CG), as well as separately among the PR, UH, and PU subgroups of the SG using descriptive statistics. Yates χ2 or analysis of variance, single factor with the Holm-Bonferroni correction for multiple comparisons, was employed for this purpose.
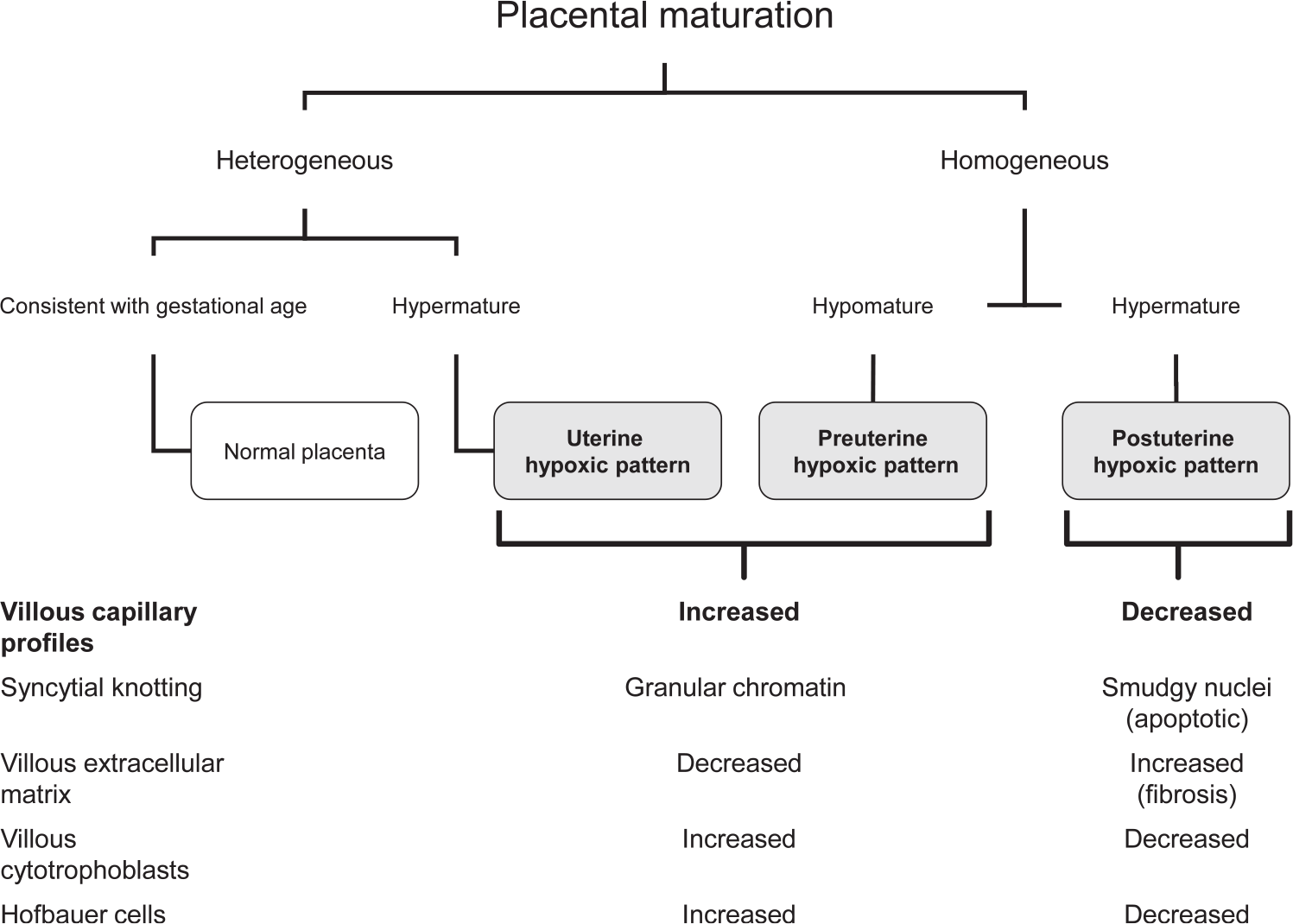
Flow sheet for diagnosis of diffuse patterns of chronic hypoxic placental injury. Knowledge of gestational age, type of villous maturation (heterogeneous vs homogeneous), and villous vascularity are the most important discriminating criteria. The preuterine and uterine hypoxic patterns are distinguished mainly on the basis of homogeneous placental maturation in the former and heterogeneous maturation in the latter. Other histological features (syncytial knotting, amount and proliferation of villous trophoblasts, amount of Hofbauer cells, and amount of extracellular matrix of chorionic villi) are also helpful. Their configurations are opposite in the postuterine pattern vs the preuterine and uterine patterns.
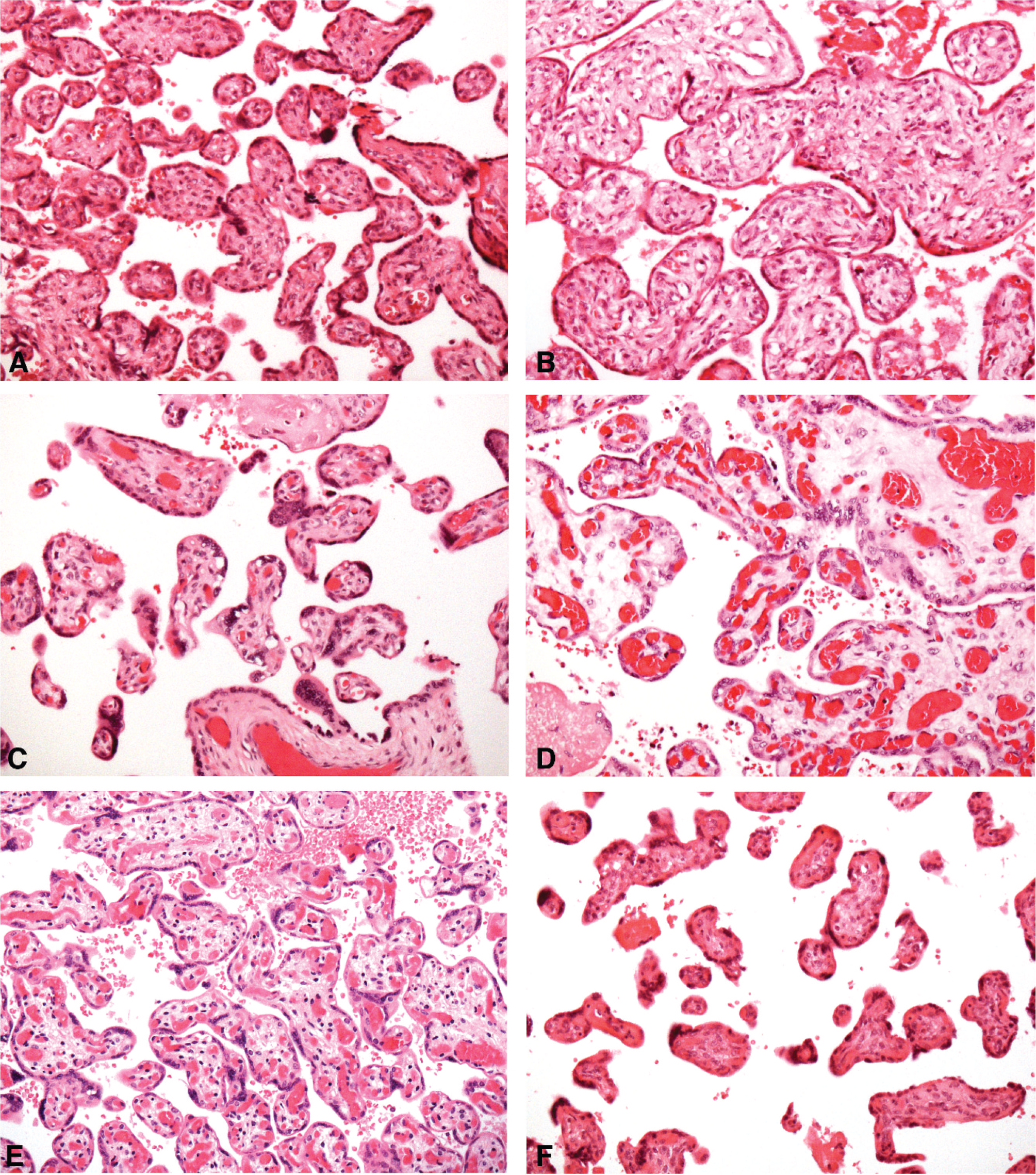
Normal placental histology vs global hypoxic patterns of placental injury.
RESULTS
Of the 5097 placentas examined, 4413 (CG) featured no histological patterns of global hypoxia (86.6%), while 684 did (15.4%) (SG); of these, 289 placentas showed PR (42.2%), 237 placentas showed UH (34.6%), and 158 placentas showed PU (23.1%).
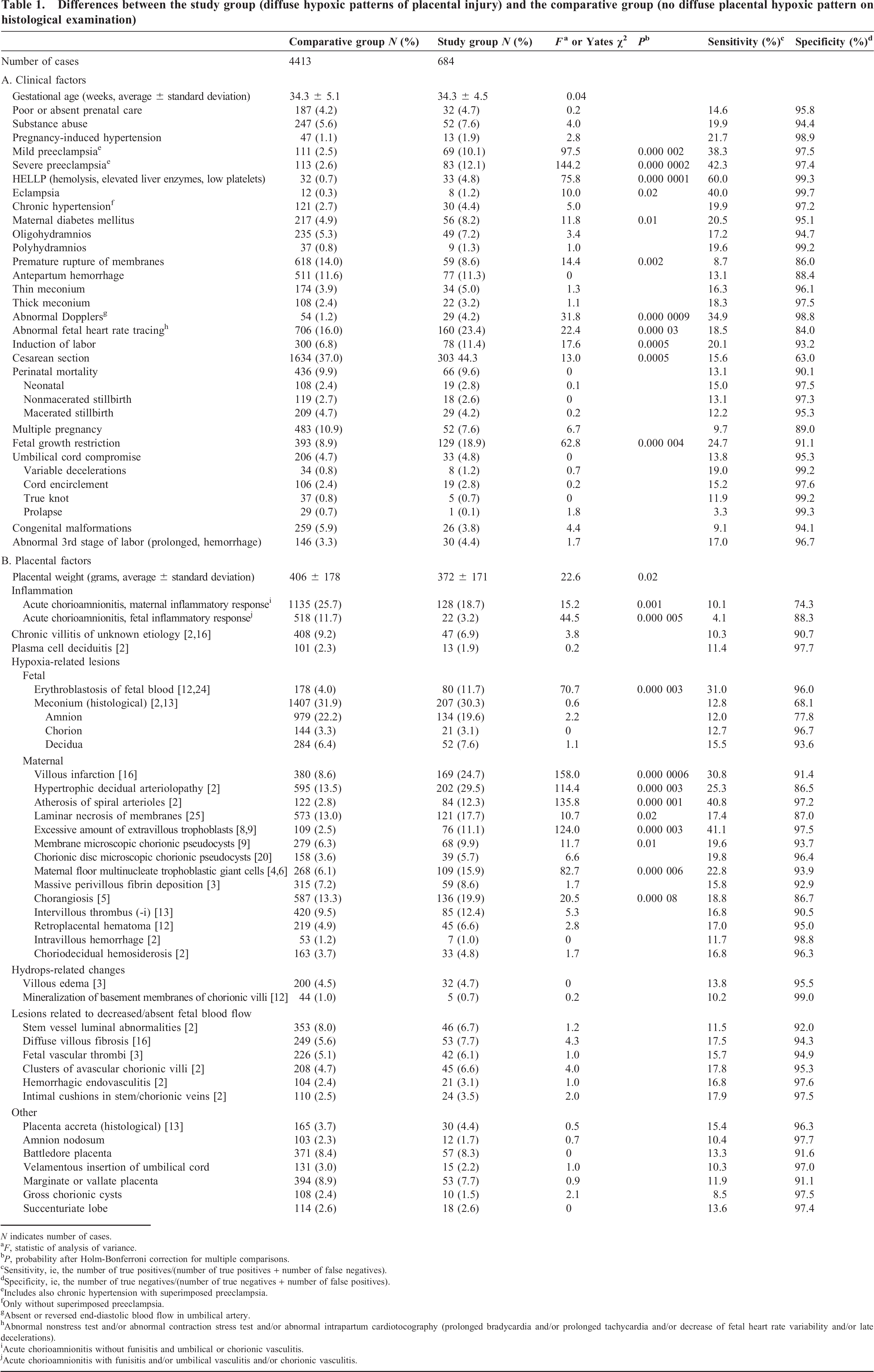
Average gestational age was identical in the SG and CG. Cases of the SG were characterized by highly statistically significant associations with known pregnancy risk factors such as preeclampsia, diabetes mellitus, abnormal cardiotocography, absent or reversed end-diastolic blood flow in umbilical arteries, and higher rates of induction of labor, cesarean sections, and fetal growth restriction. There were no statistically significant differences in umbilical cord compromise or perinatal mortality between the SG and CG. Placentas of the SG were lighter (despite the identical average gestational age). They also had statistically significantly more frequent mild erythroblastosis of fetal blood; features of acute placental hypoxia (villous infarction and/or membrane laminar necrosis); and other features of chronic placental hypoxia, such as increased amount of membrane (>7 rows of extravillous trophoblastic cells) and chorionic disc extravillous trophoblasts (>5 cell islands/placental septa per paracentral section of grossly unremarkable chorionic disc, not associated with fibrinoid material such as in massive perivillous fibrin deposition [9]), microscopic chorionic pseudocysts, clusters of multinucleated trophoblastic giant cells in the decidua, and intervillous thrombi). Decidual arteriolopathy (hypertrophic arteriolopathy and atherosis) were also seen statistically significantly more frequently in the SG. Also, some signs of diffuse (diffuse fibrosis) and focal (clusters of avascular chorionic villi) villous underperfusion were slightly more frequent in the SG (Table 1). There were no significant differences in meconium staining or hydrops-related changes. Premature rupture of membranes and acute chorioamnionitis were significantly more common in the CG. However, the specificity of the diffuse chronic hypoxic patterns of placental injury was much higher (mostly >90%) than the sensitivity, with the latter exceeding 40% for preeclampsia.
Differences between the study group (diffuse hypoxic patterns of placental injury) and the comparative group (no diffuse placental hypoxic pattern on histological examination)
N indicates number of cases.
f , statistic of analysis of variance.
P, probability after Holm-Bonferroni correction for multiple comparisons.
Sensitivity, ie, the number of true positives/(number of true positives + number of false negatives).
Specificity, ie, the number of true negatives/(number of true negatives + number of false positives).
Includes also chronic hypertension with superimposed preeclampsia.
Only without superimposed preeclampsia.
Absent or reversed end-diastolic blood flow in umbilical artery.
Abnormal nonstress test and/or abnormal contraction stress test and/or abnormal intrapartum cardiotocography (prolonged bradycardia and/or prolonged tachycardia and/or decrease of fetal heart rate variability and/or late decelerations).
Acute chorioamnionitis without funisitis and umbilical or chorionic vasculitis.
Acute chorioamnionitis with funisitis and/or umbilical vasculitis and/or chorionic vasculitis.
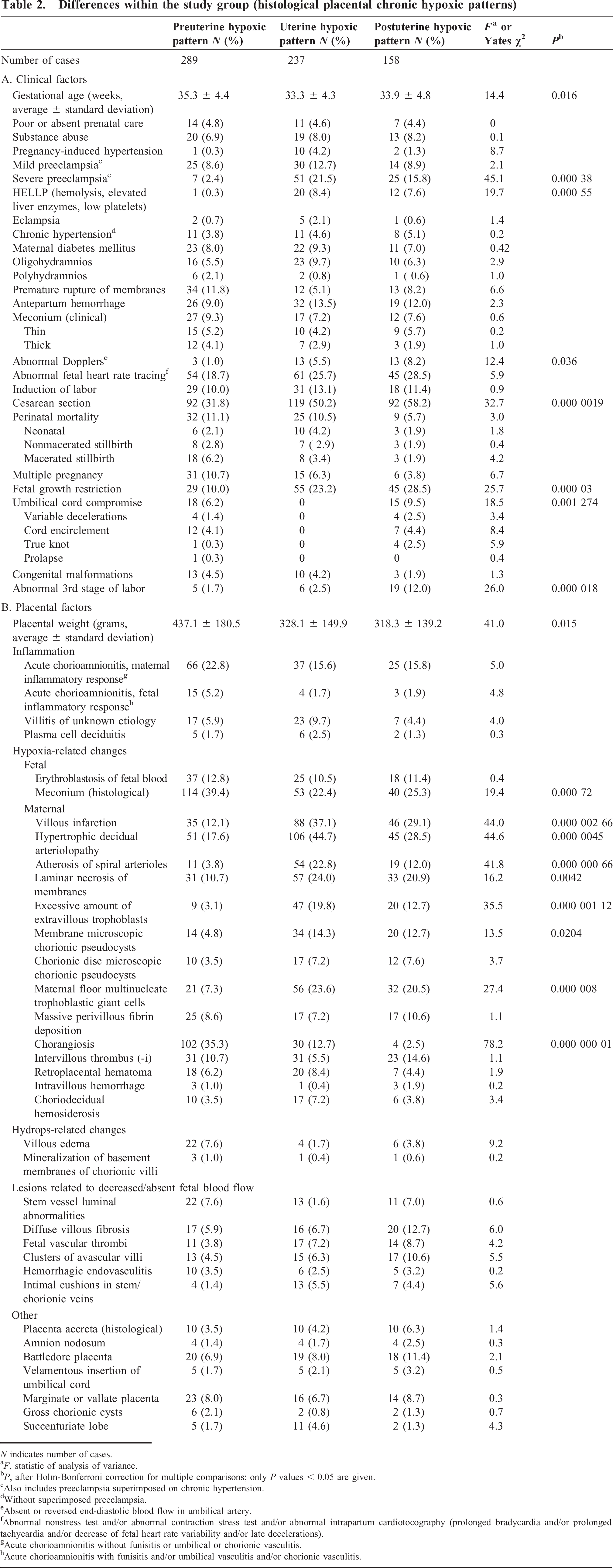
Within the SG itself (Table 2), the PR subgroup featured the highest percentages of histological meconium staining, chorangiosis, and villous edema. In the UH subgroup, the gestational age was the shortest, and preeclampsia, placental infarction, hypertrophic decidual arteriolopathy, decidual atherosis, membrane laminar necrosis, excessive extravillous trophoblasts, membrane microscopic chorionic pseudocysts, and multinucleated trophoblastic giant cells in decidua basalis were most prevalent. In the PU subgroup, abnormal antepartum Dopplers, clinical umbilical cord compromise, cesarean section delivery, fetal growth restriction, abnormalities of 3rd stage of labor, and the lowest placental weight were most commonly observed.
Differences within the study group (histological placental chronic hypoxic patterns)
N indicates number of cases.
f , statistic of analysis of variance.
P, after Holm-Bonferroni correction for multiple comparisons; only P values < 0.05 are given.
Also includes preeclampsia superimposed on chronic hypertension.
Without superimposed preeclampsia.
Absent or reversed end-diastolic blood flow in umbilical artery.
Abnormal nonstress test and/or abnormal contraction stress test and/or abnormal intrapartum cardiotocography (prolonged bradycardia and/or prolonged tachycardia and/or decrease of fetal heart rate variability and/or late decelerations).
Acute chorioamnionitis without funisitis or umbilical or chorionic vasculitis.
Acute chorioamnionitis with funisitis and/or umbilical vasculitis and/or chorionic vasculitis.
DISCUSSION
The placental response to chronic hypoxia does not follow a single pathway. Chronic hypoxia exerts an effect on placental villous development, modifying mainly placental maturity and vascularity. Less oxygen provided to the uterus as a whole imparts a PR (“preplacental,” hypoxemic) pattern of diffuse hypoxic placental injury/type of development and is associated with pregnancies at high altitudes, maternal anemia, air pollution and maternal smoking, maternal diabetes mellitus, or increased distension of the uterus (ie, multiple pregnancy) [17,19,26–29]. Multifocal prolonged restriction of blood supply to the placenta (underperfusion) induces the UH (“uteroplacental,” ischemic) pattern of chronic placental injury, typically occurring in preeclampsia at term and in late-onset fetal growth restriction [17,19], whereas the more acute restriction causes placental infarction [1,12,13]. Chronic hypoxia originating in the placenta itself results in the histological PU (“postplacental,” developmental) pattern of chronic hypoxic injury, which typically develops in retained stillbirth, early onset fetal growth restriction and preeclampsia, and fetal thrombotic vasculopathy, the latter only focally [17,19].
Whereas both the PR hypoxia and the UH hypoxia are associated with intervillous hypoxemia, the PU hypoxia features the intervillous hyperoxemia caused by decreased extraction of oxygen from the intervillous space [15,17]. Only the The UH hypoxia is caused by maternal vascular underperfusion, while the PR and PU hypoxia are not. The UH hypoxia, indicative of poor uteroplacental perfusion, is not even the most common type (Table 2).
The true practical value of using the diagnostic histological terms “preuterine,” “uterine,” and “postuterine” lies in keeping pathologists aware that there is no single pattern of chronic hypoxic placental injury, thereby expanding the pathologists’ armamentarium in this respect. Apart from the undisputed role of the type of placental maturation (Fig. 1), the villous vascularity is the keystone of diagnosis.
The PR features, unlike normal placenta, include a homogeneous villous maturation (ie, all microscopic fields look similar) and diffuse villous hypervascularity encompassing not only all cases of diffuse chorangiosis but also other diffusely hypervascular placentas with more than 5 capillary profiles per chorionic villus [16]; thus, the condition does not always meet the Altshuler rule of tens [5]. The villous hypervascularity is therefore not equivalent to chorangiosis, as the threshold for villous hypervascularity is lower. The increased proportion of vascular profiles in hypervascular villi results in a relative enlargement thereof, imparting a hypomature look to the placenta (Figs. 1,2E). The author does not share the opinion that chorangiosis is “an ominous indicator” of chronic fetal hypoxia [30], as the outcome of pregnancy in PR was the most favorable of all three hypoxic subgroups (Table 2A). In addition to hypervascularity, the PR, as in maternal anemia [31], is associated with deeper trophoblastic myometrial invasion, which results in less common clusters of multinucleated giant cells in the decidua basalis and a less frequent incidence of excessive numbers of extravillous trophoblasts (Table 2B).
Histological diagnosis of the UH hinges mainly on the heterogeneous placental hypermaturity with only focal hypervascularity, which can—but need not—meet the quantitative criteria of chorangiosis (“focal chorangiosis,” “incipient or emerging chorangiosis”) [30] (Figs. 1,2C,D). These hypervascular areas feature enlarged chorionic villi, decreased villous stromal extracellular matrix, increased Hofbauer cells, villous cytotrophoblasts, and nonapoptotic syncytial knotting, with all the features being focal (Fig. 2C,D). In addition, the presence of decidual arteriolopathy, increased extravillous trophoblasts [7,8], microscopic chorionic cysts [20], and clusters of multinucleate trophoblastic giant cells in decidua [6] (Table 2) would favor UH over PR.
The PU, like the PR, features homogeneous (therefore abnormal) placental maturation [17]; otherwise, the histological features are completely the opposite of those for PR (Fig. 1): increased smudgy (apoptotic) syncytial knotting, increased extracellular matrix of chorionic villi, and decreased villous cytotrophoblastic cells, Hofbauer cells, and villous vascularity [1,12,17,18,21,32]. By definition, all features are diffuse, as opposed to UH.
The results of the current analysis show that most cases of preeclampsia, pregnancy-induced hypertension, diabetes mellitus, nonreassuring fetal heart rate tracing, abnormal Dopplers (absent or reversed end-diastolic umbilical artery flow), and fetal growth restriction were found in the CG (without diffuse placental hypoxic patterns), ie, reflecting a sensitivity of < 50% (Table 1A). This is not unexpected for several reasons. First, although the sensitivity of the discussed patterns of chronic placental injury would seem low and unsatisfactory, the ≥40% sensitivity of the patterns for preeclampsia (Table 1) is still higher than the sensitivity of such time-honored hypoxic placental lesion as placental infarction (≤40%). In addition, various abnormal laboratory findings of preeclampsia show not only that the disorder is present before it is clinically apparent (such cases may have been present in the CG), but also that the poor placental perfusion can be operative in other medical complications of pregnancy, such as collagen vascular diseases, microvascular disease, or excessive placental size [33]. Second, the placenta is not only a large organ with substantial functional reserve; additionally, not all cases of disease and complications during pregnancy are associated with pathologic placentas and hypoxic fetuses and/or neonates. Next, therapeutic interventions such as cesarean sections or induction of labor may have had an effect on the results by preventing the development of placental or fetal hypoxia diagnosed after the mandated premature delivery. Fourth, placental oxygen consumption is four times higher than fetal oxygen consumption; therefore, the placenta is affected by hypoxic conditions first, followed only later by fetal compromise in some cases, as has been proven for at least midgestation in experimental studies [32] and confirmed by this study through the finding of less frequent fetal erythroblastosis vs purely placental hypoxic lesions (Table 1B). Next, fetal hypoxia can occur acutely (eg, after a cord compromise or abruption) and thus may not be associated with even acute histological placental hypoxic lesions, which develop 2 to 4 hours to 4 days after a hypoxic event [2]. It takes even more time for chronic lesions to develop, eg, weeks for chorangiosis [30]. Not surprisingly, clinical umbilical cord compromise and/or focal placental lesions of decreased fetal blood flow (Table 1), because they are frequently random pregnancy accidents, did not correlate with diffuse placental hypoxia, although they can produce a focal PU, so-called stasis-induced thrombotic vasculopathy, with clusters of avascular and fibrotic chorionic villi [34–37]. Congenital malformations, notorious for the frequent absence of abnormal placental findings [16,24], were understandably more common in the CG. Only severe congenital malformations forming mass lesions that interfered with blood return from the placenta can produce placental stasis-induced thrombotic vasculopathy, but not diffuse PU [25], which was, however, not a topic of this analysis. Sixth and finally, the high specificity of the discussed patterns means that positive identification of one of the patterns is significant and unlikely to occur by mere chance.
The statistical analysis further revealed that other hypoxic placental lesions showed significant correlation with the diffuse hypoxic patterns of placental injury (Table 1B). The placentas were smaller in the SG, despite the fact that the gestational age was identical in the SG and the CG. Chronic hypoxic lesions, such as an increased number of cell islands/placental septa, microscopic chorionic cysts, multinucleated trophoblastic giant cells in the decidua basalis, chorangiosis, and acute placental lesions such as placental infarctions and membrane laminar necrosis, were much more common in the SG than in the CG, as were maternal vascular lesions (hypertrophic decidual arteriolopathy and atherosis of spiral arterioles). Also, mild erythroblastosis of fetal blood, the only (and therefore the most definitive) placental evidence of fetal hypoxia [38], was three times more common in the SG than in the CG but less common than other hypoxic lesions, as mentioned earlier. Interestingly, the frequency of histological evidence of meconium release did not differ between the SG and CG, confirming the poor predictability of the sign in retrospective diagnosis of placental hypoxia [38]. Also, as expected, other nonhypoxic placental lesions were either more common in the CG or showed no statistically significant differences in prevalence between the two groups (eg, gross placental abnormalities, villous edema and ferrugination of basement membranes of chorionic villi, and lesions related to a decreased or absent fetal blood flow).
Within the SG itself, despite significant overlap among various clinical conditions and complications of pregnancy (Table 2A), a general trend toward the known associations of different types of chronic placental hypoxia was observed: pregnancy-induced hypertension and severe types of preeclampsia (but not chronic hypertension) in UH [17], multiple pregnancies in PR [28], and abnormal Dopplers and clinical umbilical cord compromise in PU [14,32,39–41]. Fetal growth restriction was more than twice as common in association with UH and PU than in PR, which is consistent with the two known and different etiologies of the conditions: late-onset and early onset fetal growth restriction, respectively [20]. Interestingly, the gestational age was, on average, 2 weeks more advanced in PR despite the fact that the prevalence of multiple gestation was the highest in this group. This subtype of chronic hypoxic pattern of placental injury was more likely to be associated with other abnormal histological features than with specific clinical conditions, thereby pointing to the polyetiological nature of the PR. This, and perhaps the higher cesarean section rates in UH and PU, resulted in an absence of statistically significant differences in perinatal mortality among the groups. Overall, PU was the most and PR the least ominous histological subtype of diffuse placental hypoxia.
With respect to placental factors (Table 2B), not only were decidual arteriolopathy, infarctions, and laminar necrosis most common in UH, which is understandable and consistent with the literature data [12,17,19]; in addition, chronic hypoxic lesions associated with an increased amount of extravillous trophoblasts (increased number of cell islands/placental septa and microscopic chorionic cysts) were more common in the UH group. It appears that they may be regarded as the complementary criteria of this type of chronic placental hypoxia in histologically borderline cases. Diffuse villous fibrosis (or increased extracellular matrix of chorionic villi) was more frequent in the PU group, possibly as evidence of a nonacute umbilical cord compromise [34,35], as occult cord compromise is notoriously difficult to exclude clinically. Therefore, only clinically positive cases (variable decelerations, encirclements, prolapse, and true knots) were statistically analyzed in this material.
In summary, examination of the placenta provides a chance to retrospectively diagnose in utero chronic hypoxia in the second half of pregnancy. Since the placenta is a large organ with a large reserve capacity, one cannot expect an absolute correlation with maternal and fetal conditions, particularly because many complications of pregnancy occur either acutely or are not caused primarily by placental pathology. Because a multiplicity of placental lesions increases the risk of fetal complications [42], in addition to naming various focal placental hypoxic lesions, recognition of various chronic hypoxic patterns should help to identify more cases of placental hypoxic injury, not just those limited to poor uteroplacental perfusion, and to clarify the etiopathogenesis of a significant proportion of complications of pregnancy and abnormal fetal or neonatal outcomes. Because the placenta does not respond in a single way to hypoxia, the histological changes should be explained in the context of clinical complications of pregnancy and gross placental and umbilical cord findings. The author believes that such an approach can contribute to a better explanation of perinatal morbidity/mortality and the mechanism of fetal injury, which potentially could be beneficial for management of future pregnancies.