
Abstract
This case report involved male infants of a size consistent with the estimated gestational age of 31 weeks. The mother of the twins was a 27-year-old, G4P3 woman with limited prenatal care who presented for cesarean delivery. Resuscitation efforts were initiated and continued until the infants became asystolic. Postmortem radiographs showed innumerable fractures of the limbs, ribs, and skull in various states of healing with callus formation; hence, the fractures were of prenatal origin. Despite the fractures, the growth of the long bones was not impaired. The radiographic findings were initially thought to represent osteogenesis imperfecta type IIC. However, there were also vascular anomalies not explained by this phenotype. Grossly, all arteries were elongated, thickened, and tortuous. The carotids, descending aorta, and iliac arteries were redundant to such an extent that they produced corkscrew patterns. There was also cutis laxa with loose, redundant skin over the entire body. Collagen genes did not show any mutations; however, when it was suggested Fibulin-4 be studied because of overlap with the condition described by Dasouki and colleagues in 2007, a homozygous premature stop codon mutation was found in that gene.
BACKGROUND AND CLINICAL HISTORY
The mother of the twins was a 27-year-old, G4P3 woman with limited prenatal care who presented for cesarean delivery of her twin fetuses at 31-2/7 weeks for oligohydramnios. Ultrasound examinations prior to delivery showed no fetal anomalies but were limited in utility as a result of the oligohydramnios. Immediately after delivery, Boy B required intubation, which was very difficult, resulting in air infiltration of the subcutaneous tissue of the anterior neck and chest. Pneumothoraces rapidly developed, requiring bilateral pigtail catheter placement. Subsequently, bilateral hemothoraces developed. Shortly thereafter, Boy B's cardiac rhythm degraded to ventricular fibrillation. Resuscitation efforts proceeded until Boy B became asystolic. Boy A was noted to have no respiratory effort. He was intubated and transfused with packed red blood cells. After 2 episodes of bradycardia Boy A no longer responded to resuscitation efforts.
Postmortem radiographs showed innumerable fractures of the limbs, thorax, and head (Figs. 1,2). These fractures were in various states of healing with callous formation. Despite the fractures, the growth of the long bones was not impaired. These radiographic findings were initially thought to represent osteogenesis imperfecta (OI) type II, group C, a lethal disorder. However, there were also significant vascular anomalies and cutis laxa, which are not explained by OI. The vascular pathology was characterized grossly by elongated, thickened, and tortuous arteries. All arteries appeared to be involved, with the carotids, descending aorta, and iliac arteries all redundant to such an extent that they produced corkscrew patterns.

Multiple fractures of limbs, thorax, and calvaria.

Multiple fractures of limbs, thorax, and calvaria.
GROSS FINDINGS
Because of the virtually identical findings in both infants they are described together. The skin over the entire body was loose and redundant. There were no scalp defects, but the parietal bones were fractured. There was slight hypertelorism and downward slant of the palpebral fissures. The external ears were apparently low-set and “crumpled.” The nose was narrow and pointed, the septum was midline, and choanae were patent but narrow. The chest was symmetrical and appropriate in size with multiple broken ribs bilaterally. The limbs had multiple fractures and healing fractures with palpable bony calluses. There was no subgaleal or subperiosteal hemorrhage. The skull was very thin, with multiple fractures of the calvarial bones. Wormian bones were present, and the cranial sutures were difficult to assess because of the fractures. The convolutions appeared consistent with a 30-week gestational age. All cranial nerves were present bilaterally. The cerebellum and brain stem were identified and were unremarkable. The cerebral vessels showed marked tortuosity and twisting. This was most notable in both inferior cerebellar arteries, the left junction of middle cerebral and anterior cerebral arteries, and the right middle cerebral artery. Organ situs in the thorax was normal; however, the coronary arteries, great vessels, and their tributaries were elongated and pursued a tortuous course, even forming “corkscrews” in the descending aorta and carotids (Figs. 3,4).

Tortuous coronary arteries, elongated pulmonary artery.
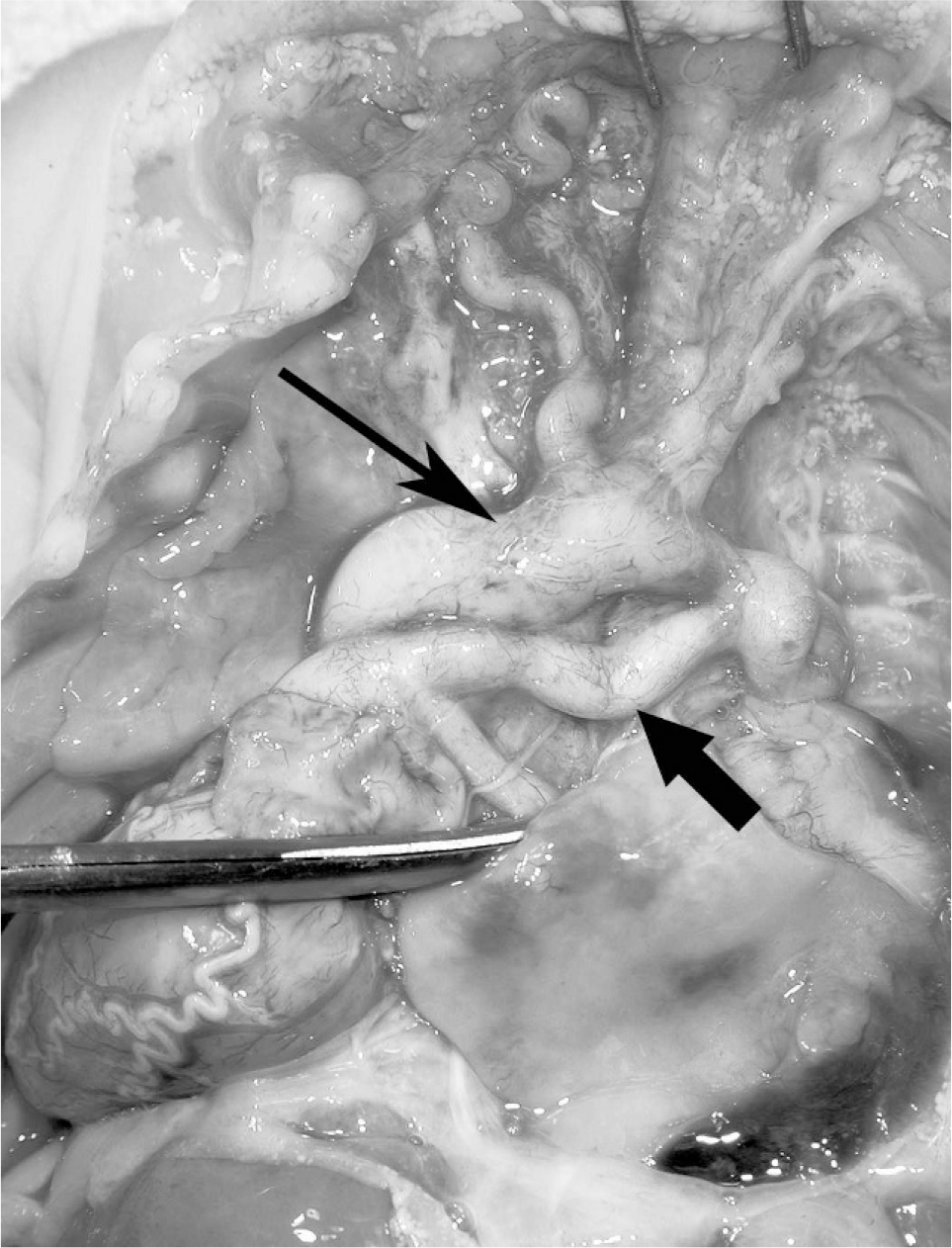
Elongated ductus arteriosus and tortuous carotids (thin arrow = aortic arch; thick arrow = ductus arteriosus).
Abdomen organ situs was normal, except for a partial defect of the dorsal mesenteric root. The right diaphragm was particularly thin and membranous. The heart and great vessels were normally situated and configured; however, the vessels and their branches were elongated and tortuous. Atrial situs was normal. The pulmonary artery exited the right ventricle and branched into the right and left pulmonary arteries in the usual fashion. The coronary ostia and arteries were normally connected. The ascending aorta was tortuous. The arch of the aorta was normally formed. The major branches of the aorta arose in the usual fashion, were long and tortuous, and patent. The trachea and bronchi branched normally. The pleural surfaces of the lungs appeared normal. The right and left lungs were small but normal in lobation. The gastrointestinal tract, pancreas, hepatobiliary system, spleen, lymphatic system, urinary tract, male genital system, and endocrine organs all appeared grossly normal. The placenta was discoid, dichorionic, and diamniotic.
MICROSCOPIC FINDINGS
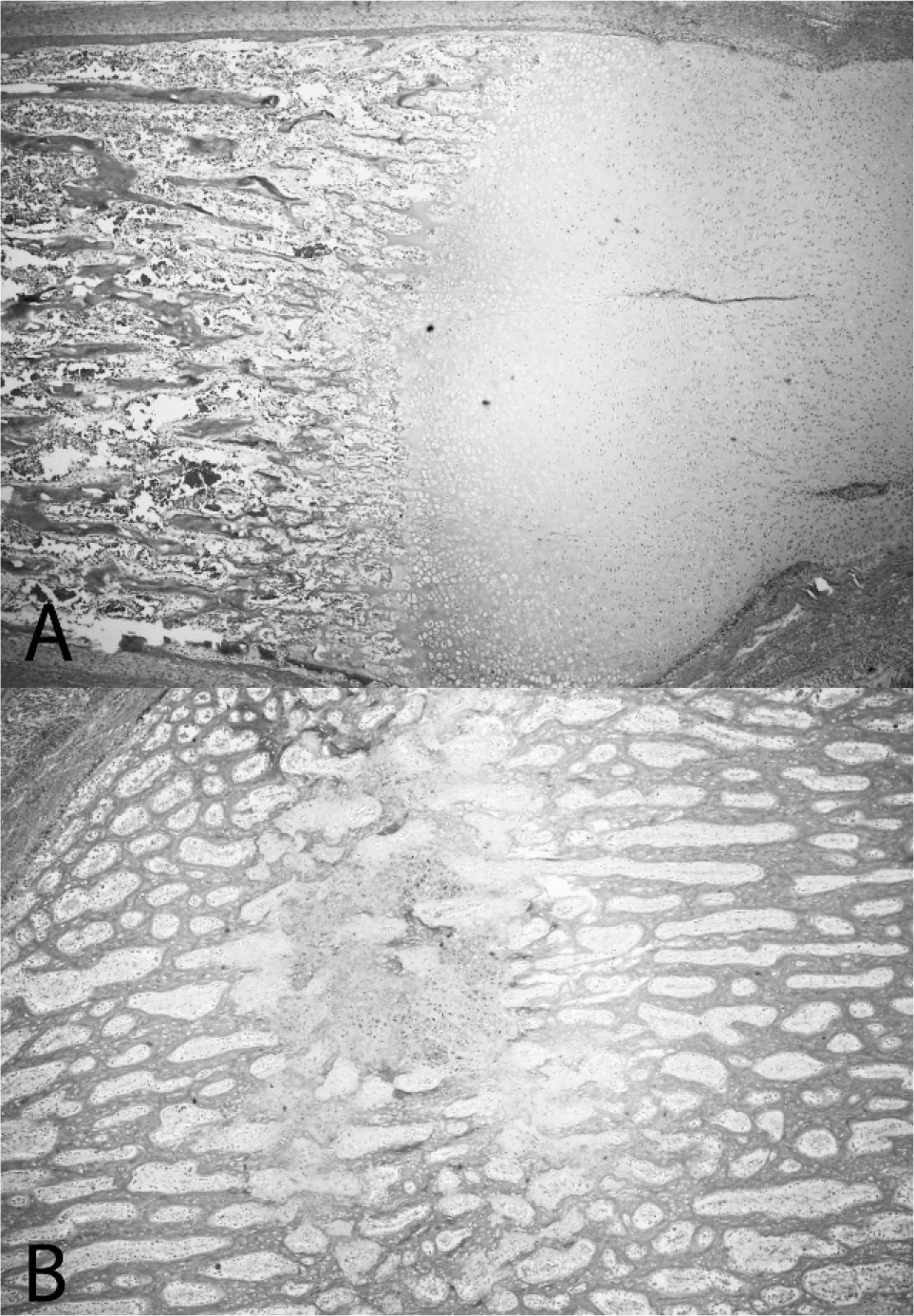
The lung was in the early alveolar phase of development. There was extensive dysplasia of the pulmonary arteries, with hypertrophy of the tunica media, intima, and adventitia. There was absence of the elastic lamina (Fig. 5). The pulmonary arteries weaved in and out of the plane of section multiple times. The lungs were incompletely aerated, with large areas of atelectasis. The coronary arteries showed a dysplasia similar to that noted in the pulmonary vessels, with thickening of the intima and media and multiple planes of section to each artery. The liver had poorly defined portal triads, with moderate degenerative swelling of hepatocytes. A segment of multiple ribs from each newborn was submitted for histologic evaluation. The epiphyseal growth zone appeared normal. There was a sharp demarcation between bone and cartilage at the junction (Fig. 6). The cellularity of the bony trabeculae appeared normal. Extramedullary hematopoiesis was present. The bones showed healing fractures, with woven bone and central cartilaginous islands. There was a lack of subperiosteal ossification and decreased formation of trabeculae (Fig. 6). Sections of brain showed a normally developing fetal parenchyma, with cellular differentiation and migration patterns appropriate for the gestational age. An elastin stain of cerebral vessels showed the presence of a normal internal elastic lamina in some vessels. The placenta was appropriately developed for the 3rd trimester. It was dichorionic and diamniotic. The remaining submitted tissues showed normal architecture and development.
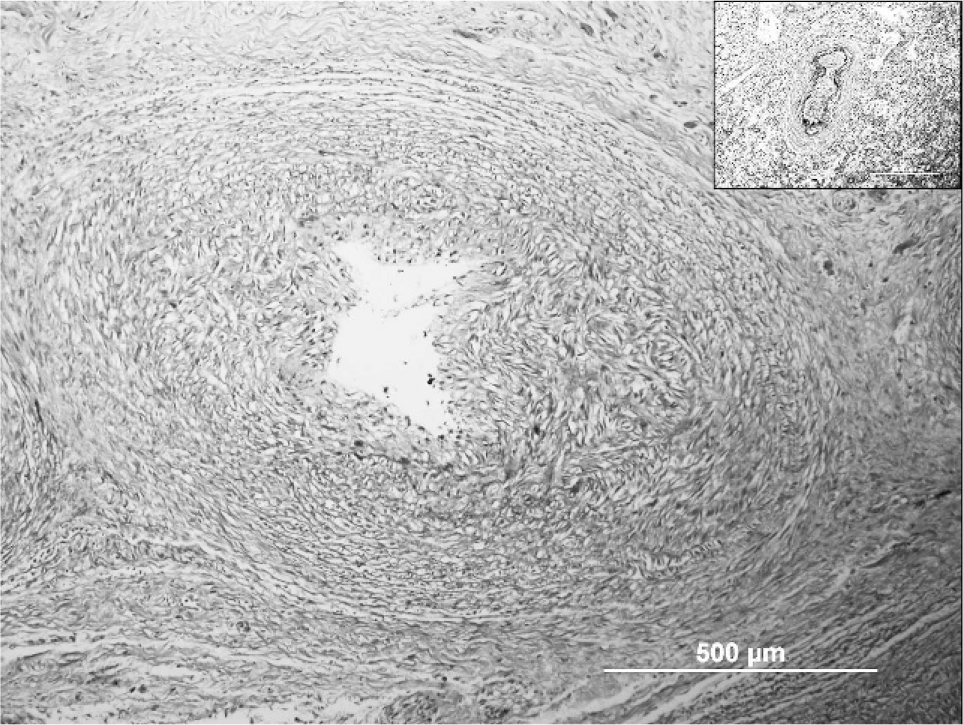
Absent elastic fiber staining in pulmonary arterioles, intimal hypertrophy (inset: age-matched control).
RESULTS OF MOLECULAR ANALYSIS
Fibroblasts from these twins were cultured and analyzed in the Collagen Diagnostic Laboratory of Dr Peter Byers (Department of Pathology, University of Washington, Seattle, WA, USA). No abnormalities of collagen structure or function were identified. After reading Dasouki and colleagues [1] we suggested that the Fibulin-4 gene be studied. This was carried out in the Byers Laboratory by Dr Ulrike Schwarze, who found a “homozygous deletion of a single G in exon1 (c.85delG), which creates a premature termination codon (PTC) in exon 2. FBLN4 has 10 coding exons, and a PTC in exon 2 is predicted to lead to efficient nonsense-mediated mRNA decay (homozygous ‘null‘) so that no fibulin-4 protein is produced” (Ulrike Schwarze, personal communication).
DISCUSSION
These vascular findings have been described previously as part of the arterial tortuosity syndrome (ATS) [2]. This “syndrome” is characterized by tortuous arteries with disorganized elastic fibers in the vessel walls. Individuals with ATS have been known to survive into early adulthood without symptoms [3]. Death can occur in ATS patients as a result of stroke or, in one case, kinking and compression of the pulmonary artery. The gene defect that was recently identified as a cause of ATS is on chromosome 20 and involves the synthesis of the GLUT10 glucose transporter [4–6].
The multiple fractures producing discontinuous beading and varying thickness to the ribs is characteristic of OI type II, class C. The slender long bones of these twins shared these same characteristics but lacked the malformed scapulae and os ischiae, as originally described in the lethal form of OI [7]. A possible mechanism for the involvement of FBLN4 (also known as EFEMP2) in bony development has recently been described [8,9]. FBLN4 interacts with lysyl-oxidase, and this enzyme interacts with the formation of collagen 1. Proper elastogenesis and collagen framework of the subperiosteal tissues through interaction of FBLN4 may have a key role in producing a similar phenotype to that seen in OI type II, class C.
The 1st report of a patient with a FBLN4 mutation [10] noted findings very similar to those of the present infants, including multiple fractures, and detected a homozygous missense mutation (p. E57K). A 2nd case was reported with compound heterozygosity and a “null” mutation [1].
It seems clear that the main cause for the phenotype is the absence of FBLN4 in the extracellular matrix, which is observed with homozygous missense mutations as well. One of the major consequences is the underdevelopment of elastic fibers, which was a prominent finding in the present cases. A question that will require further investigation is how the absence of FBLN4 and underdevelopment of elastic tissue leads to bone maldevelopment and multiple fractures.
Footnotes
ACKNOWLEDGMENTS
We are grateful to Drs Peter Byers and Ulrike Schwarze (University of Washington, Seattle, WA, USA) for collagen and FBLN4 analyses and especially to Emily Sorensen for expert manuscript preparation.