
Abstract
There is an increasing interest in the physiology and pathology of the umbilical cord because it is recognized as an important source of placental and, consequently, fetal problems. During the postmortem examination of a severely macerated 13-week-old fetus, a split umbilical cord was noted. This rare finding was seen in the middle segment of the cord, the fetal and placental ends both being normal. The pathogenesis of this lesion is not fully understood, and it is possible that it results through focal degeneration of previously formed Wharton's jelly or secondary loss of Wharton's jelly due to incomplete fusion or hypoplasia of the amniotic covering. Whatever the pathogenesis, it is assumed that an umbilical vessel devoid of its protective Wharton's jelly is more prone to compression and thrombosis with all its deleterious effects. Death in this case was probably associated with the congenital heart defect also presented by the fetus. The rarity of this lesion is probably explained by the fact that it represents the end of the spectrum of longitudinal deficiency of Wharton's jelly, a relatively common finding.
INTRODUCTION
The umbilical cord is the vital connection between the fetus and the mother, and therefore lesions involving it are regarded as potentially responsible for placental and fetal problems [1]. Transverse deficiency of Wharton's jelly is a common finding and is usually associated with umbilical cord hypercoiling. However, longitudinal deficiency leading to umbilical cord splitting is rare, with only a few cases reported in the English literature [2–5], to which we contribute another one seen in a severely macerated 13-week-old fetus.
CASE REPORT
The fetus was presented for postmortem examination with a history of delayed miscarriage at 13 weeks gestation. First trimester ultrasonography showed a cystic area in the cerebellum, but there was intrauterine fetal death before detailed examination could be performed. Unfortunately, there is no mention of the umbilical cord.
Postmortem examination revealed a severely macerated male fetus born at 13 weeks gestation. The attached umbilical cord measured 4.8 cm in length and showed a splitting starting at 0.3 cm from the fetal end. One segment of the split cord measured 1 mm in diameter and the other measured 0.6 mm (Fig. 1A).
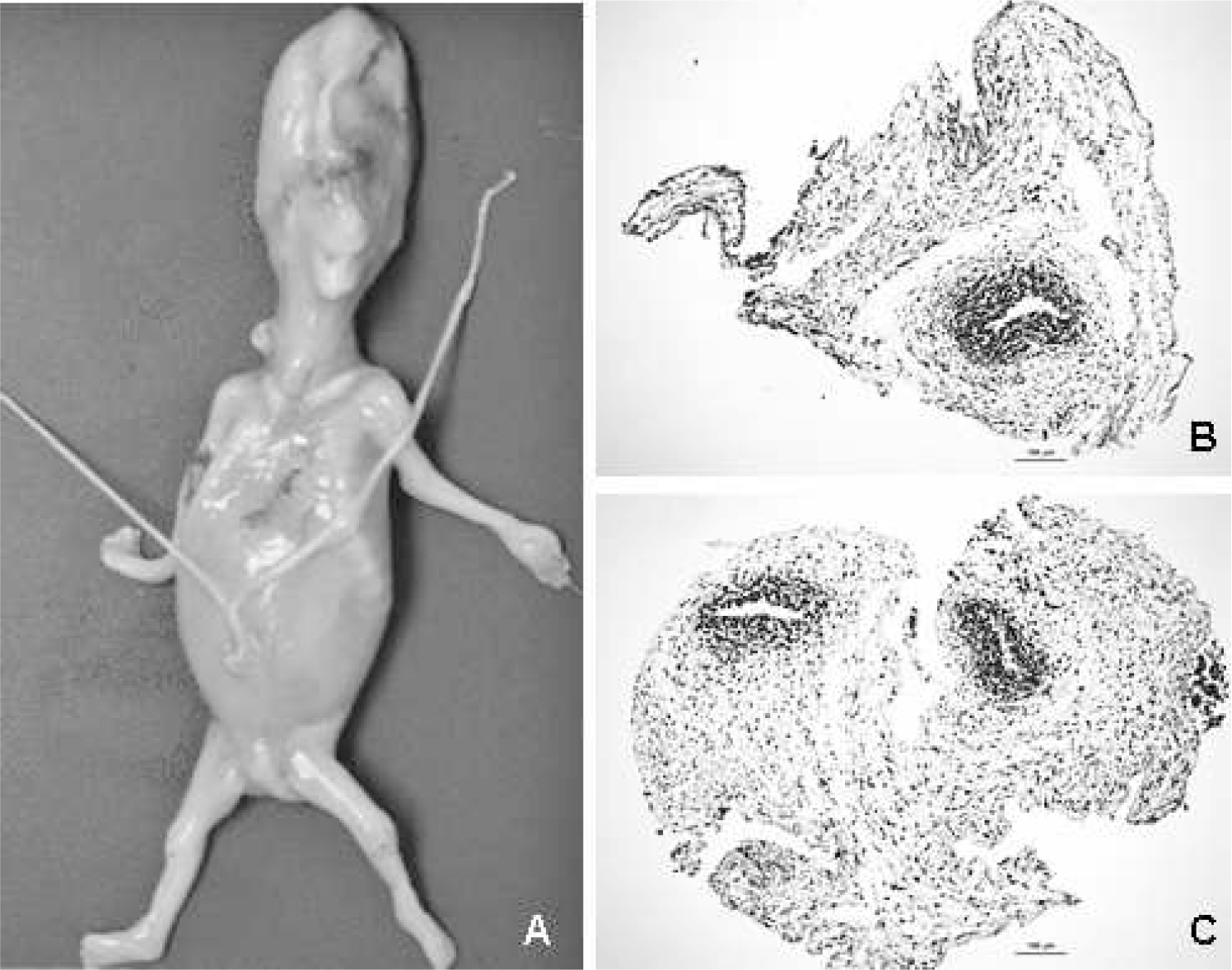
Macrophotography of a severely macerated 13-week-old fetus showing splitting of the umbilical cord. Note that the left segment is thinner and the right segment thicker (
Internal examination disclosed severely autolyzed organs, which prevented assessment of the brain, but a congenital heart defect, represented by pulmonary valve atresia and dextropositioning of the aorta, was noted. Solid-tissue karyotype obtained from the placenta was reported as 46,XY, normal male karyotype, and fluorescent in situ hybridization did not show rearrangements of the 22q11.2 region. Histologic examination of the internal organs showed advanced autolysis only.
The placenta, which presented an irregular shape, had a weight of 30 g and measured 7.5 × 4.5 × 1.3 cm. The umbilical cord insertion was central, and it measured 4 cm in length and 0.2 cm in diameter. There was a distal splitting of the umbilical cord beginning at 3 cm from the placenta end. The membranes were incomplete and translucent, and the fetal surface showed normal vascular arborization. The maternal surface was intact and normal in color, with a recent attached blood clot measuring 2 × 2 cm. The cut surface showed no focal lesions.
Histologic examination of the thinner split segment of the umbilical cord showed a single artery only (Fig. 1B), whereas the thicker split segment showed 1 artery and 1 vein (Fig. 1C), which were better visualized with AE1-AE3 immunostain (Dako, Carpinteria, CA, USA). This immunostain highlights both umbilical vessel smooth muscle cells and amniotic epithelium, revealing that the latter was partially absent in the split area. Sections of the fetal and placental ends revealed a single umbilical cord profile with 3 vessels. There was no inflammation or any other identifiable lesion.
The placenta exhibited chorionic villi with central stromal fibrosis and fine basement membrane calcification, consistent with changes that occur after fetal death. No sclerotic villi were noted. The membranes were unremarkable.
DISCUSSION
The umbilical cord is vital and yet has an apparently simple structure: 2 arteries and occasionally 1 artery and 1 vein immersed in Wharton's jelly, which are made up of ground substance of open-chain polysaccharides with a fine network of microfibrils and mesenchymal cells that present myofibroblastic differentiation towards the vessel walls all surrounded by amniotic epithelium with its supporting mesenchymal cells [6]. The umbilical vessels do not have an adventitia, and therefore Wharton's jelly is an integral part of the structure [3]. In fact, Wharton's jelly is regarded as essential for blood vessel support [7]. If deficient, adequate maintenance of the vascular lumen is impaired, allowing vascular occlusion and/or thrombosis [3].
Focal transverse Wharton's jelly deficiency is noted in umbilical cord strictures, usually associated with hypercoiled cords, but longitudinal linear deficiency is probably a primary developmental defect. Its pathogenesis is not fully understood, but apparently it occurs after degeneration or loss of pre-existent Wharton's jelly, based on the notion that normal umbilical cord development is not possible in the absence of embryonal mesenchyme [2].
Mucoid or cystic degeneration of Wharton's jelly has been proposed, although not demonstrated, as a possible pathogenetic mechanism [2].
Another hypothesis is incomplete fusion of the amniotic covering and the extraembryonic mesenchyme, future Wharton's jelly, in early fetal development, or due to hypoplasia of this amniotic covering with a secondary loss of the Wharton's jelly [3]. Fox [8] proposed a similar explanation for furcate umbilical cord insertion.
Whatever the cause, longitudinal deficiency of Wharton's jelly is a rare event, with only a few cases reported in the English literature [2–5]. Previous reported cases linked it with late fetal death [2,3], but other babies were born alive, although presenting different conditions, such as neurodevelopmental deficit [4] and patent omphalomesenteric duct [5]. In the present case, it was observed in a 1st-trimester fetus who also presented congenital heart defect, the latter being frequently associated with intrauterine death. Histology of the placenta did not disclose completely sclerotic villi or chorionic or stem vessel thrombosis, lesions frequently associated with umbilical cord accidents, but only regressive changes, which normally develop after fetal death.
Linear deficiency of Wharton's jelly has also been described in a case in which the separate blood vessel was a vein and not an artery, and this was interpreted as persistence of the right umbilical vein because the cord showed 2 veins and 2 arteries in the nonsplit areas [9].
The rarity of this lesion is probably due to its representing the end of the spectrum of longitudinal deficiency of the Wharton's jelly. Pathologists who are used to examining many placentas know that some umbilical cords show focal longitudinal grooves, which on cross-section make a Figure 8, and that on histology there is a variable amount of jelly around the vessels. There are still other cases in which Wharton's jelly deficiency is more pronounced, with variable separation of 1 artery, although keeping a single complete amniotic covering all around the cord. Finally, there are cases in which this amniotic covering is missing [3–5], as in the present case, resulting in isolated blood vessels with absent or minimal Wharton's jelly. The absence of amniotic epithelium around the split umbilical cord in placentas from living babies or fresh late fetal death [3–5] lends support to the assumption that both splitting and absent amniotic epithelium in the present case are not the result of maceration.
Whatever the cause and presentation of linear Wharton's jelly deficiency, the umbilical vessels devoid of its usual surrounding of jelly are more prone to compression and kinking, predisposing thrombosis and its deleterious effects on the chorionic villi and, more importantly, in the fetus [4].