
Abstract
Similar to nephrogenic adenomas in adults, those in children are rare benign lesions that often occur in the setting of previous surgery or chronic irritation of the urinary tract. These lesions often present with hematuria and/or as polypoid or papillary lesions on cystoscopy, which may indicate malignancy. We sought to evaluate the various patterns of nephrogenic adenoma occurring in the pediatric population and better characterize the immunophenotype of these lesions. We reviewed 21 cases of nephrogenic adenomas from urinary bladder biopsies of 16 patients. Most patients had a history of urinary bladder augmentation with recurrent urinary stones and urinary tract infections. Many cases presented as a papillary or polypoid mass on cystoscopy. The most common morphologic patterns are papillary, tubulocystic, and a mixed pattern of papillary and tubulocystic, followed by cystic and tubular. On immunostaining, PAX-2, PAX-8, CK7, and MUC-1 provided the most diffuse and intense positive reactivity for nephrogenic adenoma, whereas CD10 and P504S were focal and lesser in intensity when positive. p63 and PAX-5 were consistently negative. We conclude that, although rare in children, nephrogenic adenoma should be included in the differential diagnosis of papillary/polypoid lesions in the urinary tract, especially in the context of previous surgery, chronic irritation from recurrent urinary tract infections, or stones. The immunohistochemistry profile of nephrogenic adenomas in our study also provides evidence that these are derived from distal renal tubular cells. In difficult cases, an immunohistochemical panel consisting of cytokeratin 7, PAX-2, PAX-8, and MUC-1 may be useful.
INTRODUCTION
Nephrogenic adenomas are rare, benign, and proliferative lesions of the urinary tract that are most commonly found in the urinary bladder [1,2]. In adults, nephrogenic adenomas have been well studied and are often associated with renal transplantation and other chronic urinary tract conditions, including chronic irritation, previous surgery, and recurrent infections. Nephrogenic adenomas rarely occur in the pediatric population and are not as well studied. In children, patients can present with hematuria, irritative urinary symptoms, and/or a papillary/polypoid mass on cystoscopy. The recurrence rate of nephrogenic adenoma in children has been reported to be as high as 80% [3,4]. The exact pathogenesis of nephrogenic adenoma is unknown. One proposed histogenesis is a metaplastic process of the native urothelium in response to chronic injury, although there is recent convincing evidence that nephrogenic adenomas are derived from renal tubular cells that shed, migrate, reimplant, and then proliferate within urothelial mucosa [5–9]. We sought to evaluate the morphologic characteristics and immunophenotype of nephrogenic adenoma in a pediatric population.
METHODS
This study was approved by the Institutional Review Board of Indiana University Purdue University at Indianapolis. A computer-based text search of the surgical pathology files of Indiana University Health was conducted for the words “nephrogenic” and “adenoma” in the final diagnosis. A total of 21 cases of nephrogenic adenoma diagnosed from urinary bladder biopsies obtained between 2000 and 2011 were identified and confirmed by reviewing hematoxylin and eosin (H&E)-stained sections by all the authors. Of the 21 cases, 16 were 1st-time diagnoses and the remaining 5 were recurrences from 3 patients. A morphologic evaluation of the patterns of nephrogenic adenoma was performed on 4-μm-thick sections from formalin-fixed and paraffin-embedded tissue stained with H&E. All 21 cases had tissue blocks available for immunohistochemical staining directed against cytokeratin 7 (mouse monoclonal anti-body, ready-to-use [RTU]; Dako, Glostrup, Denmark), p63 (mouse monoclonal antibody, 1:400 dilution; Dako), MUC-1 (mouse monoclonal antibody, 1:500 dilution; Novocastra, Wetzlar, Germany), PAX-2 (rabbit polyclonal antibody, 1:100 dilution; Invitrogen, Carlsbad, CA, USA), PAX-5 (mouse monoclonal antibody, RTU; Dako), PAX-8 (rabbit polyclonal antibody, RTU; Cell Marque, Rocklin, CA, USA), CD10 (mouse monoclonal antibody, RTU; Dako), and P504S (rabbit monoclonal, RTU; Dako) performed on 4-μm-thick sections cut from formalin-fixed and paraffin-embedded tissue. A polymer-based method (EnVision FLEX or FLEX+; Dako, Carpinteria, CA, USA) and diaminobenzidine as the chromogen were utilized in a Dako automated immunostaining instrument. Negative and positive controls were performed for each immunohistochemical stain. The immunohistochemistry stains for each antibody were graded for extent and intensity of staining. Extent of staining was graded as 0 = negative, 1 = >1%–10%, 2 = >10%–50%, and 3 = >50%. Intensity of staining was graded as 0 = negative, 1+ = faint, 2+ = moderate, and 3+ = strong.
RESULTS
The results of the clinicopathologic data are summarized in Table 1. We examined 21 urinary bladder biopsies taken from 9 male and 7 female patients. Three of 16 (19%) patients had recurrences, and biopsies were taken from different procedures at different occasions. In our study, the patient age range was 2–18 years, with a mean age of 10 years and a median age of 9 years. Twelve patients had a history of previous urinary bladder surgery, 11 of which were due to structural anomalies requiring surgical repair. Seven of these patients had a history of bladder augmentation, 5 patients had a history of bladder stones, 3 cases occurred in patients with history of recurrent urinary tract infections, and 5 cases occurred in patients who had other types of urinary bladder surgeries. One case occurred in a patient with end-stage renal disease secondary to congenital urethral stricture with bilateral vesicoureteral reflux. Many cases were identified as polyps or papillary lesions during cystoscopy, 2 of which had appearances of papillary urothelial carcinomas and 1 of which appeared inflammatory in nature. Morphologic examination showed cuboidal, hobnail to low-columnar epithelium-lined tubules demonstrating variable histologic patterns, including papillary, tubular, cystic, tubulocystic, papillary, and mixed morphology (2 or more combinations of the aforementioned architectures). Nine cases had pure papillary architecture, 1 case had a pure tubular architecture, and 11 cases possessed mixed histologic patterns (Fig. 1). Of the 11 cases with mixed patterns, 9 cases were papillary and tubulocystic and 2 cases were papillary and cystic. Solid growth pattern, diffuse clear cell changes, and prominent cytologic atypia were not seen in any of the cases.
Clinicopathologic data of 21 cases of pediatric nephrogenic adenoma
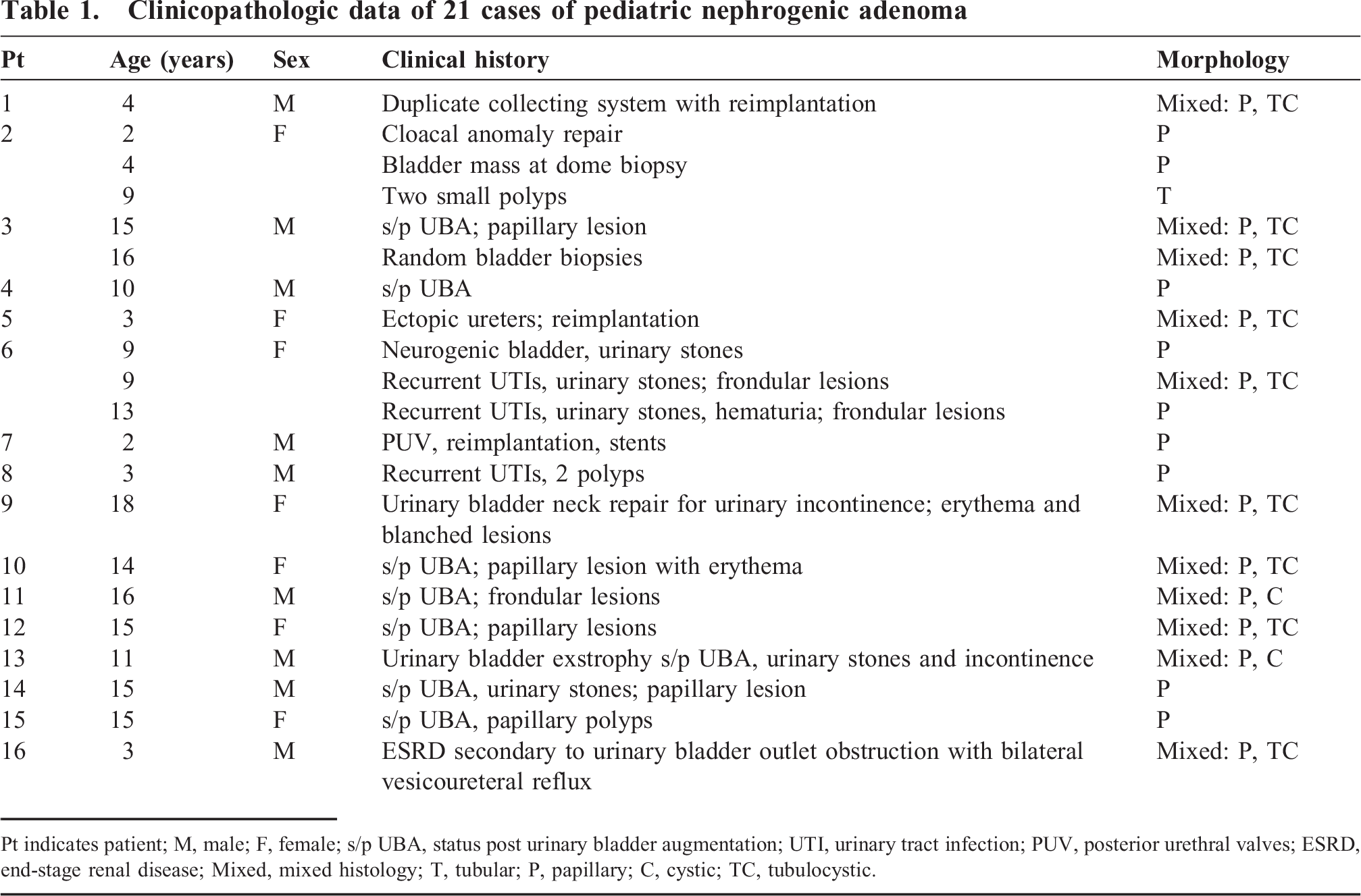
Pt indicates patient; M, male; F, female; s/p UBA, status post urinary bladder augmentation; UTI, urinary tract infection; PUV, posterior urethral valves; ESRD, end-stage renal disease; Mixed, mixed histology; T, tubular; P, papillary; C, cystic; TC, tubulocystic.
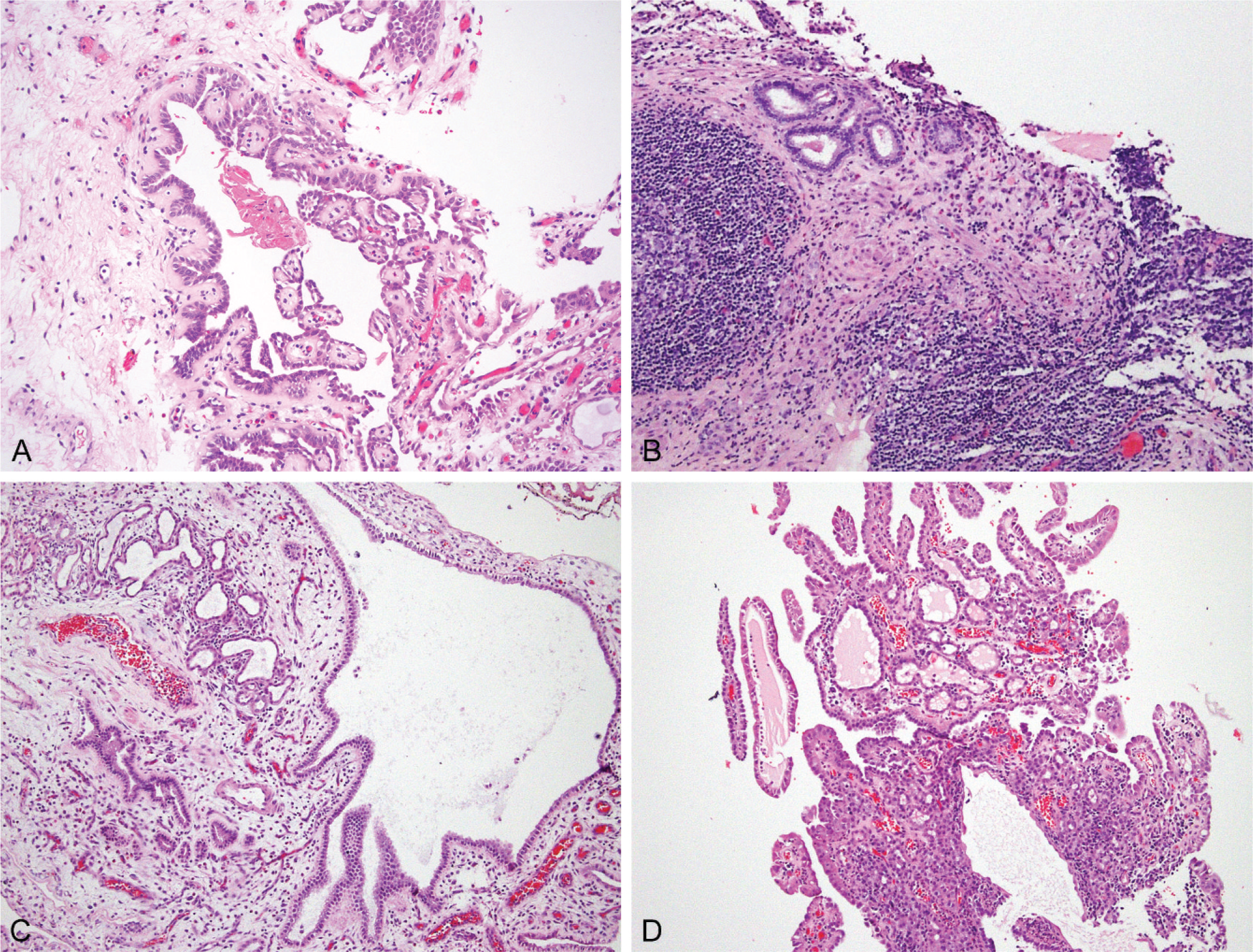
Nephrogenic adenoma exhibiting papillary (
The detailed immunohistochemical staining results for each case are summarized in Table 2, and the total percentage of cases positive for each stain is provided in Table 3. Cytokeratin 7 (cytoplasmic) and MUC-1 (luminal) both showed >50% staining with strong intensity (3+) in all cases (100%). All but 1 case had >50% extent of positive staining for PAX-8 (nuclear), 18 of which showed strong intensity. PAX-2 (nuclear) showed similar staining, with 17 of 21 cases (81%) demonstrating >50% staining with either moderate (2+) or strong (3+) intensity. p63 and PAX-5 were uniformly negative in all 21 cases. Variable positive reactivity was observed with P504S and CD10 and ranged from negative to >50% for extent of staining; intensity ranged from weak to strong. The adjacent normal urothelium showed consistent positive immunostaining for cytokeratin 7 and p63 but was negative for P504S, PAX-2, PAX-5, CD10, and MUC-1 (Fig. 2).
Immunohistochemical staining results for each of the 21 cases of nephrogenic adenoma
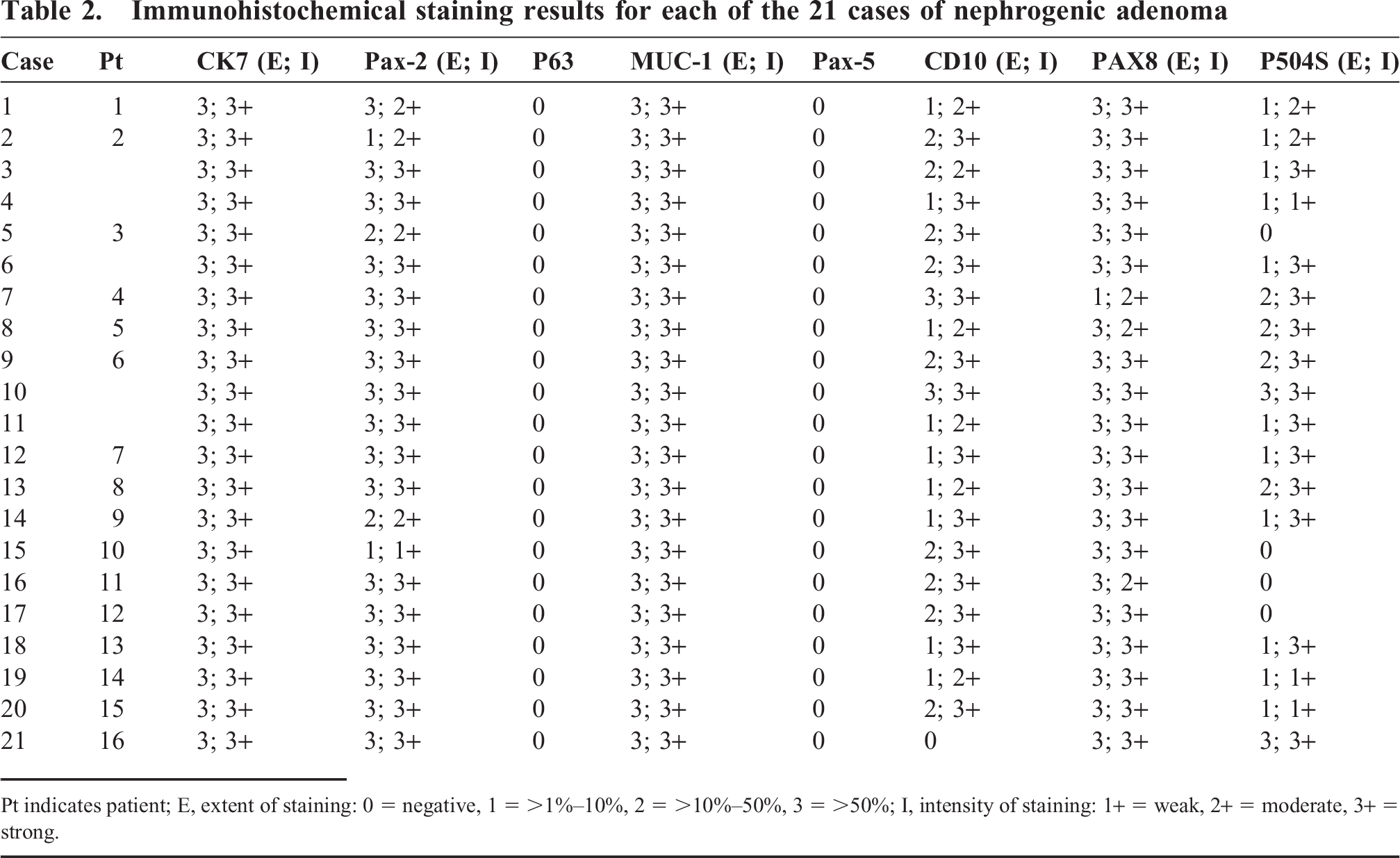
Pt indicates patient; E, extent of staining: 0 = negative, 1 = > 1%–10%, 2 = >10%–50%, 3 = >50%; I, intensity of staining: 1+ = weak, 2+ = moderate, 3+ = strong.
Immunoreactivity of nephrogenic adenomas
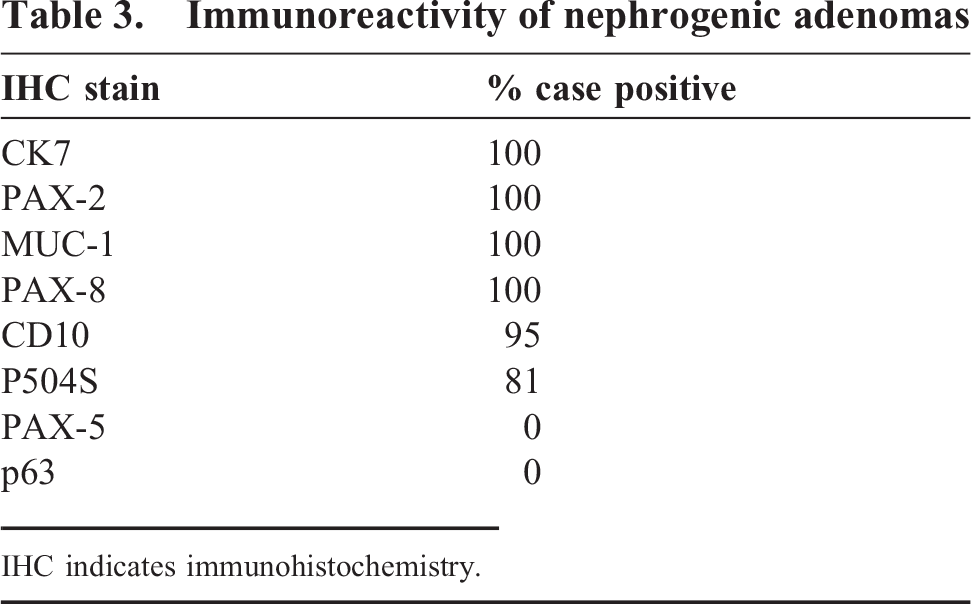
IHC indicates immunohistochemistry.

immunohistochemical characteristics of nephrogenic adenoma demonstrating intense cytoplasmic staining for cytokeratin 7 (
DISCUSSION
In pediatric patients, nephrogenic adenomas, although rare, should be included in the differential diagnosis of polypoid or papillary lesions in the urinary tract, especially in the context of previous surgery or chronic irritation from recurrent urinary tract infections or stones.
A study done by Franke and colleagues reported a 3% occurrence rate of nephrogenic adenomas within a pediatric augmented bladder population [10], indicating an overall rare occurrence (rare, but not uncommon in such a population), and this is in accordance with our data, given 7 of 16 (44%) patients in our study had undergone urinary bladder augmentation for neurogenic bladders.
At least 12 of the 21 total cases of urinary bladder biopsies grossly presented with polyps, nodular lesions, papillary lesions, and/or erythema on cystoscopy, some of which appeared especially malignant per clinical notes. Pathologic examination revealed no cytologic atypia, diffuse clear cell change, or solid growth pattern, and various patterns were observed, with the most common being mixed morphology consisting of papillary and tubulocystic patterns. The 2nd most common was a “pure” papillary morphology. We did not encounter other patterns previously reported in the adult population: thyroid like, microcystic, vascular hobnail, signet ring cell like, or fibromyxoid [11–13].
The immunohistochemistry profile of nephrogenic adenomas in our study shows a strong and diffuse positive reactivity with cytokeratin 7, PAX-2, PAX-8, and MUC-1 with variable, usually less intense, and more focal reactivity to CD10 and P504S. These immunohistochemical results are all in accordance with those previously reported in adult nephrogenic adenomas [13–16]. A study by Fromont and colleagues reported nonspecific positive staining for P504S and CD10 in nephrogenic adenomas as a result of the use of avidin–biotin detection procedure reacting with the high level of endogenous biotin [14]. The P504S and CD10 antibodies utilized in our study were also detected utilizing an avidin–biotin system and may account for the focal positive reactivity. The positive immunostaining for PAX-2 and PAX-8, both of which are renal transcription factors, provides support that nephrogenic adenomas in pediatric patients are derived from distal renal tubular cells [5–9].
Recurrence is common and may be asymptomatic. In our study, 3 of 16 (19%) patients had recurrences of nephrogenic adenoma, and the recurrence rate is similar to that reported by Simo and colleagues [4]. The treatment of choice remains complete surgical resection and close clinical follow up.
The gross appearance and morphologic features of nephrogenic adenoma may mimic other entities that occur in the urinary tract. It is important to distinguish benign nephrogenic adenoma from other mimickers that commonly occur in the pediatric population, such as embryonal rhabdomyosarcoma, fibroepithelial polyp, papillary/polypoid cystitis, and urothelial neoplasms, in order of frequency [17]. It may be especially difficult given that some of these differential diagnoses can present with similar clinical histories of prior surgeries and chronic irritation in the urinary tract. Fortunately, most of these previously mentioned entities are distinctly different from nephrogenic adenoma on morphologic examination. A polypoid botryoid variant of embryonal rhabdomyosarcoma typically consists of spindled tumor cells and classically displays a cambium layer compared to the bland, single layer of hobnail to cuboidal cells of nephrogenic adenoma. A fibroepithelial polyp is composed of a dense polypoid to papillary fibrous stroma without inflammation, lined by a multilayered bland urothelium. There is no risk of recurrence with a fibroepithelial polyp and no clinical follow up is needed, unlike with a nephrogenic adenoma. Urothelial neoplasms are lined by urothelium, instead of the single cuboidal- or hobnail-lined epithelium of nephrogenic adenoma.
Urinary tract malignancies, including prostatic and urothelial carcinomas, are rare in the pediatric population and will not pose a diagnostic challenge in the differential diagnosis of pediatric nephrogenic adenoma. However, should a rare situation arise in which these lesions are within the differential diagnosis, principles used in the adult population to distinguish these entities are also applicable in the pediatric population. Prostatic adenocarcinoma frequently expresses P504S, and it may have an atrophic appearance that resembles the tubular pattern of nephrogenic adenoma; however, the typical association with other patterns of nephrogenic adenoma and positive reactivity with PAX-2 and PAX-8 are helpful in making the correct diagnosis. Clear cell adenocarcinoma of the bladder also expresses P504S and CD10, but a lack of prominent clear cells, bland cytology, and absence of mitoses all point toward a diagnosis of nephrogenic adenoma. Urothelial carcinoma, papillary type or nested variant, may exhibit bland cytology and have a similar growth pattern to nephrogenic adenoma. It can be accurately diagnosed by occasional positive p63 reactivity and lack of PAX-2 and PAX-8 staining, together with the commonly associated, more typical patterns of high-grade urothelial carcinoma.
In conclusion, this study compares the nephrogenic adenoma morphologic spectrum and immunohistochemical similarities between the pediatric and the adult populations, in addition to providing credence to the implantation theory of renal tubular cells in urinary bladder as the primary source of nephrogenic differentiation. Nephrogenic adenoma is a benign lesion that may cystoscopically and microscopically mimic malignant neoplasms in the urinary tract. It is important to include nephrogenic adenoma in the differential diagnosis, especially if there is a clinical history of prior bladder surgery, such as urinary bladder augmentation or presence of chronic irritation or inflammation. In difficult cases, careful morphologic examination and an immunohistochemistry panel including cytokeratin 7, PAX-2, PAX-8, MUC-1, and p63 are recommended.
Footnotes
ACKNOWLEDGMENTS
We thank Tracey Bender of our department for her careful editing and manuscript preparation and Connie Temm for her expedient immunohistochemical preparations.