
Abstract
Infantile fibrosarcoma is a rare soft tissue tumor that usually presents either at birth or in the 1st year of life. Here we describe a case of a 4-month-old female who presented with a congenital right axillary mass. The initial clinical impression was benign vascular/lymphatic malformation. The core biopsy showed a spindle cell lesion with abundant vasculature represented by small vascular channels. However, immunohistochemical analysis did not support a diagnosis of vascular lesion/tumor. Polymerase chain reaction study for ETS Translocation Variant 6/neurotrophic tyrosine kinase receptor, type 3 fusion transcript was positive, and the diagnosis of infantile fibrosarcoma was established. The patient underwent resection of the axillary mass. Microscopic examination of the resection specimen showed numerous vascular channels. Intermixed there were also cellular areas composed of spindle cells similar to those seen in the biopsy material. Molecular studies were repeated and confirmed the diagnosis of infantile fibrosarcoma. Infantile fibrosarcoma has been previously reported in the literature to clinically masquerade as hemangioma. In addition, this case proves that infantile fibrosarcoma could also mimic vascular malformations on clinical, radiologic, and pathologic exams. In fact, the vascular component of the tumor is very unusual in our patient and represents a histologic feature that has not been described before. The case highlights the diagnostic challenges at clinical, radiologic, and pathologic levels in some cases of infantile fibrosarcoma and raises awareness among clinicians and pathologists related to another peculiar pattern that can be encountered in this disease.
INTRODUCTION
Infantile fibrosarcoma is a rare soft tissue tumor that is usually congenital or develops in the 1st year of life. Clinically it presents as a localized, well-delineated swelling after birth, with progressive growth. Sometimes a prominent vascular component is present within the tumor. In these cases, the mass could be clinically interpreted as a vascular lesion, in particular congenital hemangioma [1–11]. Herein we present a case of infantile fibrosarcoma misinterpreted clinically and radiologically as a vascular malformation. Even on histologic examination the vascular component was very prominent and unusual. The rarity of this tumor, as well as its potential to mimic other entities, may render a diagnostic challenge that can result in misdiagnosis and subsequent inappropriate patient management. This case raises awareness among clinicians and pathologists of another rare pattern that infantile fibrosarcoma can exhibit.
CASE REPORT
The patient was a 4-month-old female who came to medical attention for a right axillary mass. The lesion had been present since birth and had grown considerably since then. The patient had no significant medical history otherwise. No signs of infection were noted. At physical examination her neck was supple and she had no lymphadenopathy. There was a 2-cm, smooth, well-defined soft mass on the right lateral chest wall at the lower border of the axilla. There was no tenderness, redness, or drainage from the area. The ultrasound examination revealed a cyst in the subcutaneous fat layer, consistent with a lymphangioma.
A biopsy of the lesion was performed. During the procedure a large amount of blood was drained from the lesion, and, in fact, the mass decreased in size following biopsy. These findings were supportive again of a vascular/lymphatic process. The touch imprints showed blood and clusters of monotonous spindle cells with elongated nuclei with rounded ends, finely dispersed chromatin, and inconspicuous nucleoli (Fig. 1A). In correlation with the cytology, microscopic examination of the biopsy cores revealed a cellular lesion with abundant vasculature. The lesion was composed of spindle cells with few admixed inflammatory cells (lymphocytes and plasma cells) and mainly small-sized vessels (Fig. 1B). The spindle cells were mildly pleomorphic and did not show a particular architectural arrangement (Fig. 1C). Rare mitotic figures were seen. The vessels were lined by bland endothelial cells. The initial impression, based on light microscopy, was of kaposiform hemangioendothelioma. However, immunohistochemical stains did not support this diagnosis: CD31 and smooth muscle antigen (SMA) immunostains highlighted only the vascular spaces and were negative in the tumor cells; glucose transporter 1 (GLUT-1), D2-40 (podoplanin), desmin, and activin receptor-like kinase 1 immunostains were also negative. Given the clinical presentation, as well as prior reports of infantile fibrosarcoma mimicking hemangiomas, polymerase chain reaction studies for ETS Translocation Variant 6/neurotrophic tyrosine kinase receptor, type 3 (ETV6/NTRK3) fusion transcript were performed and were positive. These findings were consistent with the diagnosis of infantile (congenital) fibrosarcoma.
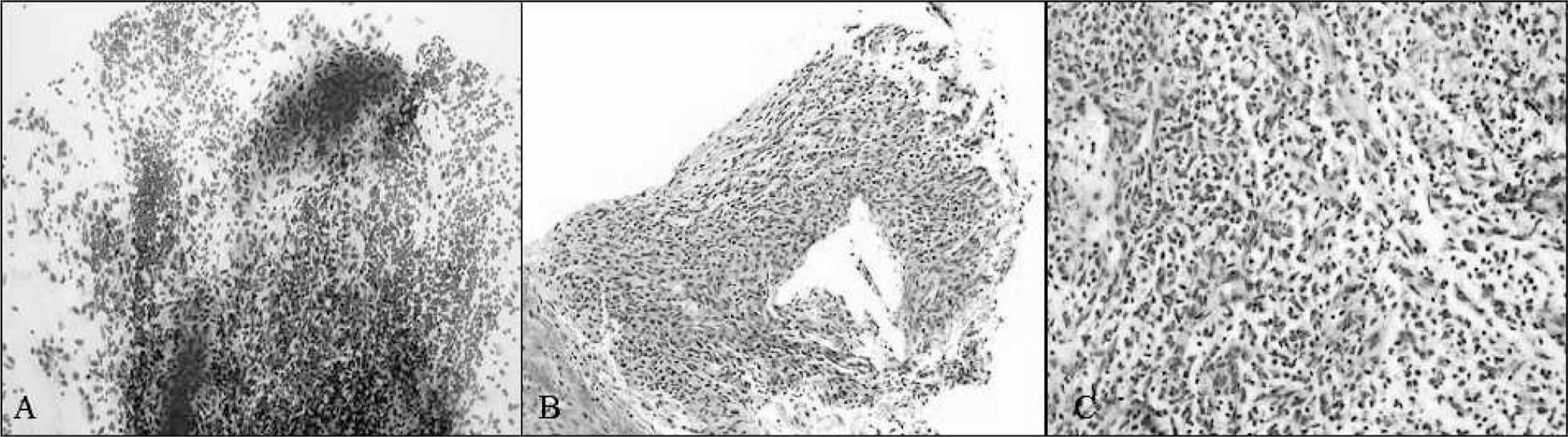
Microscopic examination of the biopsy. (
Two weeks later, the patient underwent excision of the axillary lesion. Gross examination of the resection specimen showed a 4.4 × 4.0 × 3.0–cm, well-delineated mass with a variegated aspect, composed predominantly (∼70%) of cystic spaces filled with blood alternating with solid soft, dark red areas occupying about one third of the mass (Fig. 2A). Microscopic examination revealed a well-demarcated, deep-seated lesion with a predominant vascular component, different from the one observed on the biopsy material. This time the vessels were medium to large in size, ectatic, and creating anastomosing channels, mostly with a thin wall (Fig. 2B) showing occasional SMA-positive bundles of smooth muscle (Fig. 2C,D). Within the walls of the vascular channels there were plump spindled cells with elongated nuclei and a fair amount of eosinophilic cytoplasm, similar to the lesional cells present in the biopsy. The cells showed low-grade nuclear pleomorphism and low mitotic activity. The solid component resembled the biopsy sample and consisted of similar lesional cells (Fig. 2E). Repeated immunohistochemical studies revealed a pattern of staining analogous to that seen on the biopsy material, with CD31 and SMA stains highlighting the vascular spaces and being negative in the tumor cells (Fig. 2F,G). Molecular studies (reverse transcriptase–polymerase chain reaction) for ETV6/NTRK3 fusion product were repeated and again were positive. Based on these findings a final diagnosis of infantile fibrosarcoma with a prominent vascular component was rendered.
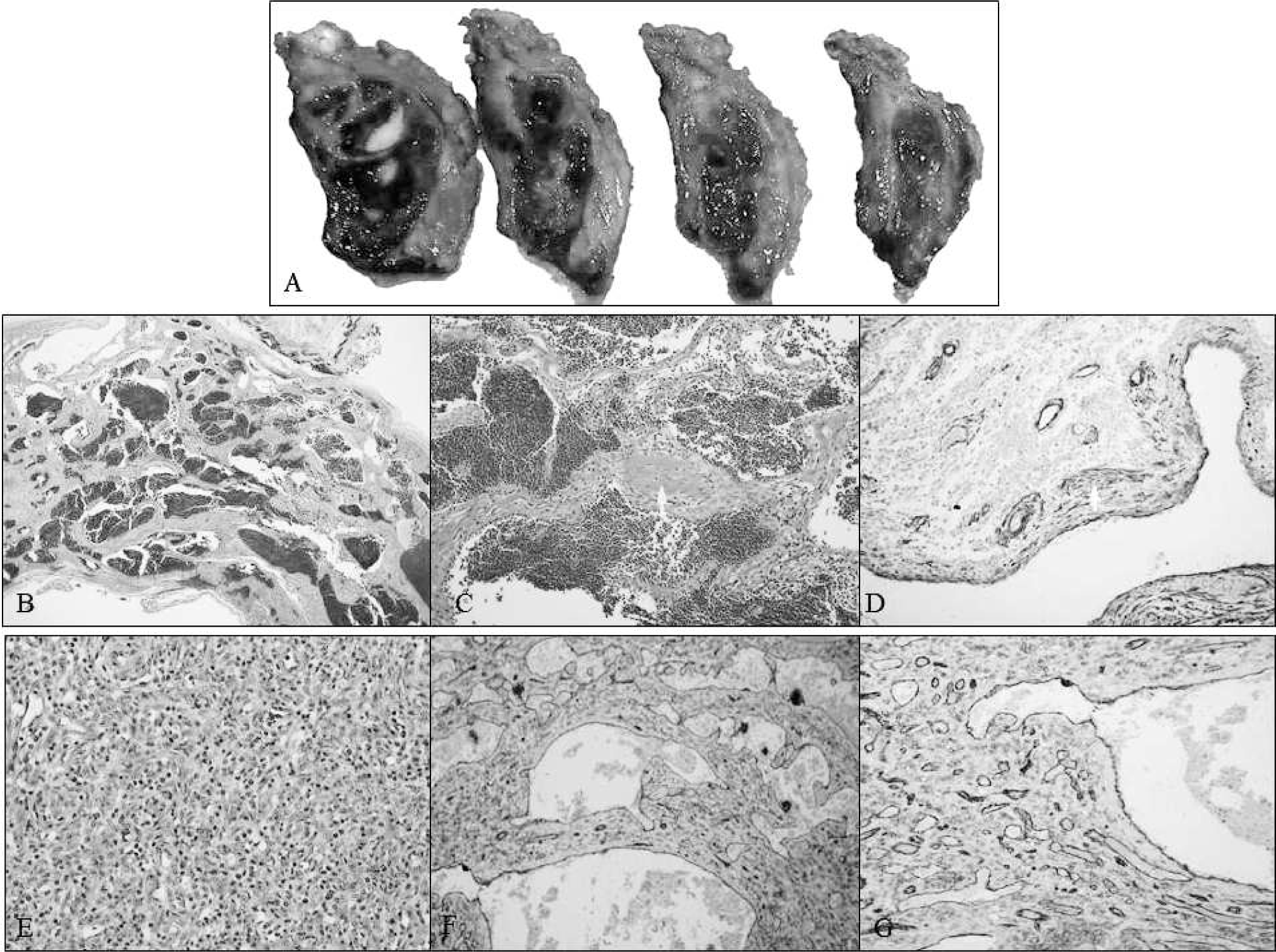
Gross and microscopic findings of the resection specimen. (
DISCUSSION AND LITERATURE REVIEW
Congenital infantile fibrosarcoma is an indolent, slow-growing, malignant spindle cell tumor that is present at birth or occurs in the infancy period. It presents as a well-defined lesion that is usually located on the extremities, but head/neck area and trunk are also common locations.
Clinically, infantile fibrosarcoma can mimic other entities. It has been reported [12] to be misdiagnosed as teratoma. However, the most frequently reported clinical masquerader of infantile fibrosarcoma is a vascular proliferation, in particular hemangioma [1–11], with only one other case being clinically misinterpreted as vascular malformation [7]. Moreover, infantile fibrosarcoma can present with massive bleeding from the tumor and a clinical picture of Kasabach-Merrit syndrome [1,4,8], creating confusion with a kaposiform hemangioendothelioma [8].
Our present case shows that infantile fibrosarcoma can mimic vascular/lymphatic malformations in addition to hemangiomas not only on physical and radiologic exam but also histologically. The patient presented clinically with what appeared to be a vascular proliferation. The differential diagnosis for a congenital enlarging vascular lesion usually includes a number of common entities, such as hemangiomas or vascular malformations; malignancies are less likely to be considered. Radiology studies have shown poor discrimination between highly vascularized malignant soft tissue lesions and benign vascular proliferations [13]. This fact is also illustrated by our case as well as by prior reports [1–10,Table 1], in which the radiologic techniques commonly detected a mass with prominent vessels, sometimes with a cystic, hemorrhagic appearance similar to that seen in our case [1,8] and could not establish the correct diagnosis, misinterpreting the tumor as being a benign vascular proliferation. The upper extremities (including the shoulder/axillary region) seemed to be the most common location in these cases. There appears to be an equal distribution between male and female patients in this case study. With the exception of 2 cases [3,9], all of the other lesions were present at birth.
A review of prior infantile fibrosarcoma cases mimicking vascular lesions
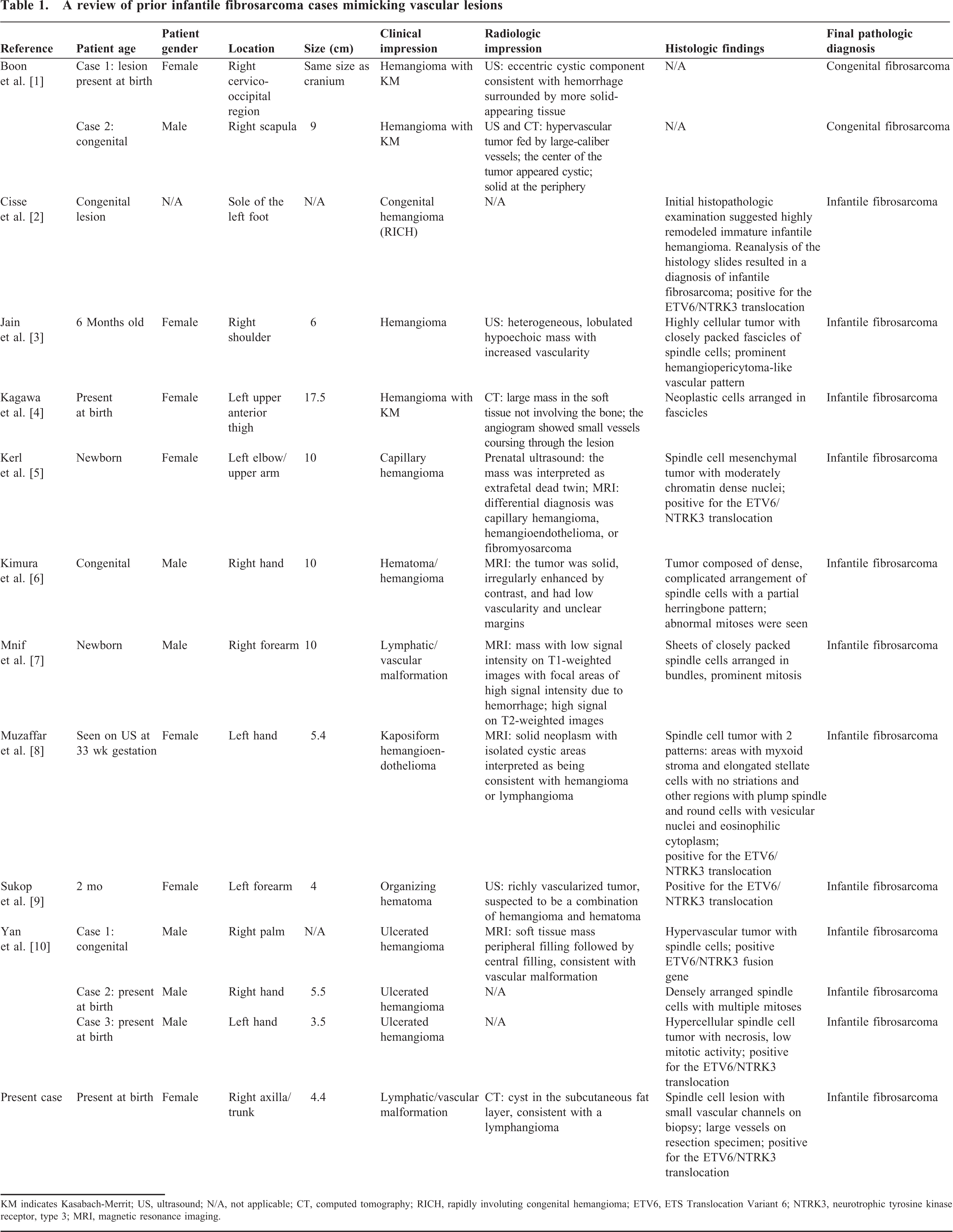
KM indicates Kasabach-Merrit; US, ultrasound; N/A, not applicable; CT, computed tomography; RICH, rapidly involuting congenital hemangioma; ETV6, ETS Translocation Variant 6; NTRK3, neurotrophic tyrosine kinase receptor, type 3; MRI, magnetic resonance imaging.
In all cases, the definitive diagnosis relied on histopathological characteristics. Typically the microscopic appearance of infantile fibrosarcoma is that of a cellular tumor composed of uniform spindle cells arranged in fascicles, sometimes with a herringbone arrangement. Hemangiopericytoma-like vessels could be seen within the lesion. However, there is an impressive histologic diversity of these tumors: some can show a poorly organized pattern of immature and even primitive mesenchymal cells; others can have a variable number of admixed inflammatory cells. Our case also exhibited an unusual histologic pattern and represented a diagnostic challenge. After reviewing the biopsy material, the 1st impression was of kaposiform hemangioendothelioma, given the small elongated vascular spaces and slightly atypical spindle cells, with rare mitosis admixed with occasional plasma cells, although other soft features seen in kaposiform hemagioendothelioma (cytoplasmic hyaline globules, fragmented red blood cells, and platelet thrombi) were not detected in our case. Another consideration was an infantile hemangioma in the proliferative phase, but the lobular architecture of this lesion was not apparent in our patient. However, the diagnosis of a vascular tumor was not supported by the immunohistochemistry studies (negative CD31, podoplanin, GLUT-1 stains). Only the patient's age, clinical presentation, and previous reports of infantile fibrosarcoma misdiagnosed as vascular lesions prompted us to perform molecular studies, which confirmed the diagnosis. The resection specimen was very puzzling as well: it also had a prominent vascular component representing about 70% of the lesion, characterized this time by large, thin-walled vascular channels, some with smooth muscle within the walls. No hemangiopericytoma-like vessels were present. Lymphatics were also absent, as D2-40 immunostain was negative. In the absence of a previous diagnosis (such as in our case, in which infantile fibrosarcoma had already been diagnosed by molecular studies performed on the biopsy material), one can easily misinterpret this type of lesion as a vascular (in particular, a venous/arterio-venous) malformation. The morphologic appearance of this vascular component is very unusual in infantile fibrosarcoma; commonly, the vessels seen within this tumor have a hemangiopericytomatous appearance. Microscopy in 2 of the prior cases [2,10: case 1] also revealed a hypervascular lesion, but in contrast to our case, the histologic exam resembled more closely a hemangioma [2]. In fact, both of these cases required reevaluation of the pathology slides for a correct diagnosis. The morphology in the remaining cases was straightforward, and a final diagnosis of congenital/infantile fibrosarcoma was rendered.
As is shown by the present case, molecular studies are very helpful in those instances with peculiar morphologic appearance. Infantile fibrosarcoma has a distinctive reciprocal translocation, t(12;15)(p13;q25), resulting in ETV6/NTRK3 gene fusion. This rearrangement, described by Knezevich and colleagues [14], fuses the ETV6 (also known as the TEL) gene from 12p13 with the NTRK3 gene (also known as TrkC) on 15q25. ETS Translocation Variant 6 is a member of the E 26 family of transcription factors and is essential for developmental processes such as hematopoiesis and yolk-sac angiogenesis; NTRK3 is a transmembrane surface receptor for neurotrophin-3, has protein tyrosine kinase activity, and is primarily expressed in the central nervous system, where it is involved in growth, development, and cell survival. The ETV6/NTRK3 chimeric protein has been linked to multiple signaling cascades, including Ras-MAP kinase and PI3K-AKT, through the IRS-1 adaptor protein [15]. It has been shown to have potent in vivo and in vitro transforming activity in several cell lineages, including fibroblasts [16], hematopoietic cells [17], and breast epithelial cells [18]. As such, it is not surprising to find this translocation as a recurrent phenomenon in infantile fibrosarcoma. In one review [19], the chimeric gene was observed in 10 of 11 cases and helped distinguish congenital fibrosarcoma from other spindle cell lesions encountered in children. The same translocation has also been detected in other tumors, some of which are seen in childhood, namely, congenital mesoblastic nephroma [20] and acute myelogenous leukemia [21], as well as in secretory carcinoma of the breast [18].
Interestingly, neurotrophin-3 (the NTRK3 ligand) has recently has been demonstrated [22] to be a novel angiogenic factor capable of neovascularization in a mouse model of limb ischemia. This finding might explain the prominent vasculature in some cases of infantile fibrosarcoma: it is possible that constitutive activation of the NTRK3 tyrosine kinase function due to ETV6/NTRK3 fusion leads to development of numerous vascular channels within the tumor. The relationship between the neoplastic cells of infantile fibrosarcoma and the vascular component of the lesion is probably even more intriguing: in a case report by Miura and colleagues [23], congenital fibrosarcoma showed regression during the course of the disease and transformation to hemagiopericytomatous tissue that lost expression of the ETV6/NTRK3 fusion gene. Based on these findings, one might wonder if infantile fibrosarcoma has a vascular origin. In fact, the histogenesis of this disease is not well understood, but morphologic similarities between congenital fibrosarcoma, infantile myofibromatosis, and congenital hemangiopericytoma point to the fact that these entities are histogenetically related [24,25]. In a study by Blizniukov and colleagues [26], ultrastructural analysis revealed well-differentiated collagen-forming neoplastic fibroblasts in about half of the infantile fibrosarcoma cases; immature embryonic-like fibroblasts closely resembling perichondrial fibroblasts of the embryonic limb at 6 weeks of development were also identified.
Generally, infantile fibrosarcoma has an excellent prognosis and a very low metastatic rate. Initial optimal treatment is complete surgical excision, which is associated with a survival rate of about 90% in long-term studies [27]. The role of preoperative chemotherapy hasn't been well defined, but this therapy can be used when the tumor is located in a difficult surgical area to decrease tumor size and facilitate the surgery. Postoperative chemotherapy can be used when the microscopic surgical margins are positive for tumor. Radiation therapy is usually avoided as a result of its associated growth disturbances.
The findings presented here highlight the importance of considering less-likely entities when an infant presents with what appears to be clinically and radiologically a vascular lesion. In fact, many conditions that can masquerade as infantile hemangioma were reported [28], some of which are malignant and require immediate and appropriate management. Infantile fibrosarcoma is one of them and should be considered in the differential diagnosis of congenital tumors with a prominent vascular component. This challenging case also points to a peculiar, novel histologic appearance of infantile fibrosarcoma with prominent larger caliber vascular channels without a hemangiopericytomatous look. This pattern can impose diagnostic challenges to the unaware pathologist and proves that congenital fibrosarcoma can be mistaken for a vascular lesion even on morphologic exam.