
Abstract
The length of the umbilical cord is an important data item, and little is known about the effects of time and fixation on measurement. Such a change has implications for the diagnosis of a long and short cord. This study was conducted to examine the effects of time and formalin fixation on cord length in a routine practice setting. We measured 90 cords from singleton term pregnancies within 5 minutes of delivery, again in the fresh state at 1 to 2 hours, and again after 24 to 48 hours of formalin fixation. The mean cord length was 536.7 mm at delivery. Mean cord shortening was 17.6 mm (3% reduction in length) between delivery and measurement at 1 to 2 hours, and 62.2 mm (12% reduction) between delivery and measurement after 24 to 48 hours fixation. Both values were statistically significant (P < 0.001). Studies on cord length should include data on time of measurement and fixation status.
INTRODUCTION
The umbilical cord is examined routinely in the course of laboratory assessment of a placenta, and length is one of the variables noted. Cord length is an important parameter, with 55 to 60 cm at term frequently taken as normal [1,2]. Long cords are associated with adverse outcomes, fetal abnormalities, and neonatal respiratory distress [3]. Short cords are associated with complications during labor and delivery for the mother and infant [4].
It has been suggested that the cord may contract by up to 7 cm after delivery because of tissue contraction, with a single abstract widely quoted [5]. Given the paucity of data in the literature, the aim of this study was to assess the effect of time and formalin fixation on the length of the umbilical cord in a routine clinical practice setting.
METHODS
This prospective observational study was conducted over a 2-month period at the National Maternity Hospital, Dublin, Ireland. We examined 93 placentas from singleton term pregnancies (37–41 completed weeks of gestation). Complete data were available on 90 cases. Delivery methods included vaginal and caesarean section. No change was made to routine obstetric practice, which is for delayed clamping (ie, approximately 2 minutes after delivery) in cases of uncomplicated delivery. Cord length was measured in millimeters from the insertion of the cord onto the placenta to its free (fetal) end. The first measurement was conducted within 5 minutes of delivery, and repeated 1 to 2 hours postdelivery while the placenta still was in the fresh state. Following 24 to 48 hours immersion in 10% neutral buffered formalin, the cord length was measured again. Paper measuring tapes were used. To obviate any potential bias to “round-off” to the nearest centimeter, the blank side of the tape was used until the measurement was complete, and the length in millimeters then read from the printed side. For each of the three observations, the length was measured three times and the mean of the three values was taken as the final length. Statistical analysis of results was by the post hoc test analysis using Bonferroni correction to estimate the mean shortening between lengths. A P value of 0.05 was regarded as significant.
RESULTS
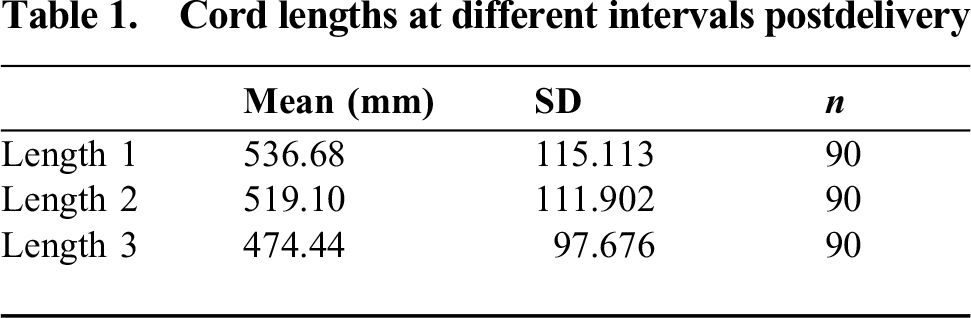
Of 90 cases evaluated, 63 (70%) were noninstrumental vaginal deliveries, 8 (9%) were instrumental vaginal deliveries, and 19 (21%) were delivered by cesarean section. The maternal age range was 21 to 41 years, with a mean of 32.5 years. Of the women 30 (33.3%) were primiparous and 60 (66.6%) were multiparous. Mean cord lengths were 536.68 ± 115.11 mm at delivery (time 1), 519.10 ± 111.9 mm at 1 to 2 hours post-delivery (time 2), and 474.44 ± 97.68 mm 24 to 48 hours after formalin fixation (time 3, Table 1). Applying the Bonferroni correction, the mean length differences were 17.58 mm between times 1 and 2, and 62.24 mm between times 1 and 3. Both results were statistically significant (P < 0.001).
Cord lengths at different intervals postdelivery
DISCUSSION
Mean cord length differs in different published studies. The population mean from a study of over 30,000 placentas assessed in a pathology laboratory was 37.38 cm [3]. Mean cord length in a population of 1082 consecutive low-risk women was 43 cm [6]. The mean cord length in 11,029 singleton Japanese placentas of 34 to 41 weeks' gestational age was 56.2 cm [7]. In none of the above studies was time to measurement or fixation status specified.
Not surprisingly, the definitions of long and short cords vary. Berg and Rayburn [8] reported on 3019 cords of consecutive deliveries >34 weeks of gestation, measured by different observers within minutes of delivery. They defined a long cord as >80 cm (3.7% of cases), and a short cord as <35 cm (2% of cases). In data from the Collaborative Perinatal Project, the 10th centile for cord length was 43 cm and the 90th centile was 77 cm at 40 weeks' gestation [2]. Baergen and colleagues [3] defined an extremely long cord as 2 standard deviations above their population mean; that is, ≥70 cm. Others have taken ± 1.5 standard deviations (SD) from their mean giving definitions of a long cord as ≥74 cm and a short cord as ≤38 cm [7].
Problems in assessment include variables outside the pathologist's control, such as the length of cord segment that remains attached to the neonate, the length of cord (if any) removed for clinical purposes, rupture of the cord during the third stage of labor, the interval from delivery to laboratory assessment of the cord, and the effect of fixation. Many pathologists will be cautious in diagnosing abnormal cord length, and a short cord in particular, due to these factors. A large study on the implications of diagnosis of a short cord did not, in fact, give a specific measurement [4]. Similarly, because the evidence base for shortening is scanty, cord pathology may be underestimated and the possibility of a long cord dismissed, despite possible clinical relevance. Therefore, the current study was designed to examine the effects of time and fixation on cord length in the context of routine practice. We have shown that the normal cord shortens by 3% in the first 1 to 2 hours following delivery, and shortens by 12% between delivery and assessment 24 to 48 hours after fixation. The mean cord shortening in this study was 62 mm and a cord that measures 35 cm when fixed is likely to have measured 40 cm in vivo.
Short umbilical cords may result from reduced tension on the cord during early pregnancy. Associated factors include early intrauterine fetal constraint, such as oligohydramnios, skeletal dysplasia, or fetal limb dysfunction. Risk factors include increased maternal body mass index, nulliparity, and fetal congenital malformation, such as trisomy 21[4]. Shorts cords are associated with increased maternal and fetal complications, with a higher rate of operative vaginal delivery and have more complications in labor [4]. The difference of 10 cm between investigators in diagnosis of a short cord has implications for studies examining these associations. While this study did not examine long and short cords specifically, it is reasonable to assume the same percentage shortening applies to both.
The effect of formalin fixation on tissue varies, depending on the organ involved. Goldstein and colleagues [9] evaluated a 5 cm margin in colorectal excision specimens and showed a 57% reduction in length, 70% of which occurred in the 10 to 20 minutes following surgical excision, and 30% post fixation. In a separate study of skin excisions a difference of 16% to 18% was found, but this was not attributed to formalin fixation [10]. The larger volume of smooth muscle in the bowel compared to the skin may account for the different percentages. We have shown that most of the observed shortening of the cord occurs following formalin fixation, although as we did not compare a fresh to a formalin-fixed cohort over a similar time period, this cannot be attributed exclusively to the effect of formalin with certainty. However, fixation following a period in the fresh state parallels the practice in many laboratories.
In conclusion, our data suggested that studies should state whether the measurement is of the fresh or fixed cord. While measurement of the cord immediately after delivery is optimal [3], this may not be achievable in all maternity units. Noting the time at which the cord length was measured will permit identification of cords of abnormal length.
Footnotes
ACKNOWLEDGMENTS
We thank the delivery ward staff of the National Maternity Hospital and Mr John Long, Senior Anatomic Pathology Technician.