
Abstract
Nevocytes (NC) and mastocytes (MC) have different progenitors but share stem cell factor as regulator/activator of NC and for differentiation/proliferation of MC. Both cell types express stem cell factor receptor CD117. We hypothesize that large/giant congenital melanocytic nevi (L/GCMN) may associate with MC hyperplasia. Forty-nine L/GCMN were examined, 12 samples from uninvolved skin of L/GCMN patients and 6 control skin samples studied with Giemsa and immunohistochemistry for CD117 and MC-tryptase. Picrosirius red (PR) was used to assess fibrosis. Digital images were used to count MC/mm2 using ImageJ software. Western blot (WB) for MC-tryptase in 12 GCMN and 12 non-nevus samples was performed. Analysis of variance (Tukey) and Pearson statistical tests were applied. Increased MCs were observed in nevus tissue (75.1 ± 35.3 MCs/mm2) and in uninvolved skin (53.74 ± 27.7 MC/ mm2). P = 0.109 from patients with L/GCMN, compared with controls from individuals without L/GCMN (28.74 ± 8.4 MC/mm2); P = 0.001 supported by results of WB analysis for tryptase. A positive trend toward correlation of MC numbers with fibrosis, assessed by PR staining fell short of statistical significance (r = 0.245; P = 0.086); no difference in fibrosis was found between nevus and non-nevus skin from patients with L/GCMN (P = 0.136). We found a higher density of MC, both in normal-appearing skin and nevus areas of L/GCMN patients, compared with control skin samples from individuals without nevi. Given the abnormal wound healing and allergic reactions described in L/GCMN patients, these findings suggest a potential role for MC in the biology of L/GCMN, making them a potential target for therapeutic intervention.
INTRODUCTION
Congenital melanocytic nevi (CMN) are present at birth or arise within the 1st few weeks of life [1]; they involve 1%–6% of newborns at birth [2]. These nevi are classified as large or giant (L/GCMN) if the maximum diameter expected in adulthood is larger than 20 cm. Large/giant CMN are much less common and has an estimated incidence of 1 in 20 000 to 500 000 live births [3]. Patients with L/GCMN have increased risk of malignant transformation [4,5]. Recently, this abnormality has been shown to be caused by somatic mutations in codon Q61 of NRAS [6].
It is well known that mastocytes (MC) participate in allergic and inflammatory processes. In this context, we have previously reported an increased number of MC in a “bulky perineal nevocytoma” (a form of L/GCMN) of a 3-year-old girl who presented with intractable pruritus [7]. Pruritus is a frequent symptom in patients with L/GCMN and could be intense and difficult to control with medication [7,8]. In addition, MC and melanocytes derive from different progenitors but share regulation by stem cell factor (SCF). This growth factor (also named “mast cell growth factor” or “kit-ligand”) is a cytokine fundamental for differentiation and proliferation of MC and for spatial distribution and activation of melanocytes [9]. Nevocytes (NC) from patients with CMN also express SCF receptor, CD117. Other clinical findings also support a relationship between MC and melanocytic lesions [10,11]; however, MC numbers have never been systematically assessed in L/GCMN.
The aim of this study was to investigate the number and distribution of the MC in nevi and unaffected skin from patients with L/GCMN compared with skin from patients without L/GCMN.
MATERIALS AND METHODS
This study was approved by the University of Pittsburgh Institutional Review Board with written exemption because it used only pre-existing de-identified materials and data.
Tissues
De-identified skin samples with the diagnosis of L/GCMN collected from 2000 to 2011 were obtained from the archive of the Department of Pathology, Children's Hospital of Pittsburgh of University of Pittsburgh Medical Center, and from the Congenital Nevi and Other Neurocristopathies-tissue bank (COND-Bank) housed at the Rangos Research Center, Children's Hospital of Pittsburgh, University of Pittsburgh Medical Center. Exclusion criteria were defined as inadequate or nonrepresentative samples for analysis or when other types of nevi were diagnosed on pathology review. Corresponding clinical information (age, gender, clinical diagnosis, number of nevi, body site, and size of the nevus) was recorded. As proposed by Krengel and colleagues [12], the projected adult size of the main nevi was used for clinical categorization of the CMN.
The specimens had been fixed in 10% formalin and processed by routine paraffin-embedding technique. To select the paraffin blocks with representative nevus tissue and to confirm the diagnosis, a review of all hematoxylin and eosin-stained slides was performed. One block was selected from each patient and recut to provide 5 μsections.
Stains
Slides were stained with Giemsa to detect the metachromatic granules of MC and with Picrosirus red (PR) (data not shown) using an established technique employed to assess the amount of fibrosis [13]. Immunohistochemistry (IHC) was performed on the Ventana Benchmark XT IHC automated staining platform (with controlled and standardized conditions) (Tucson, AZ, USA) following the manufacturer's instructions, with positive and negative controls. Primary anti-tryptase (monoclonal, clone AA1, Dako Cytomation, Carpinteria, CA, USA) diluted at 1∶200 and anti-CD117 (polyclonal, Dako) diluted at 1∶250 were used. All slides were visualized using the Ventana uvRed alkaline phosphatase detection kit to avoid confusing melanin with 3,3′-diaminobenzidine deposition.
Image capture and morphometric analysis
Whole-slide images were obtained scanning slides with an Aperio Scanscope at ×20 (scan resolution at 0.499 μm/pixels) (Sausalito, CA, USA). After scanning, images at ×20 magnification were captured (image dimension 1024 × 768 pixels), and both epidermis and areas with technical artifacts (section folds, knife marks, etc.) were excluded. Nine images in different dermal layers were analyzed for each slide: 3 photographs from the papillary dermis, 3 from mid-reticular dermis, and 3 from the deep reticular dermis. Morphometric analysis was carried out using the ImageJ software and the technique described at the National Institutes of Health (NIH) website http://rsbweb.nih.gov/ij/docs/.
Tryptase immunohistochemistry was used to measure the number of MC based on the morphometric point-counting technique, and the size of overlaying fields was fitted to the size of 1 MC [14]. The results were expressed as number of MC per mm2. Quantification of fibrosis using PR was assessed by determining the percentage of the total tissue occupied by collagen [13].
Western blotting
Approximately 30 mg MC nevus tissue samples containing lesions were finely minced using scalpel and proteins extracted using 120 μl of lysis buffer (50 mM HEPES pH 7.4, 150 mM NaCl, 100 mM NaF, 1 mM MgCl2, 1.5 mM EGTA, 10% glycerol, 1% Triton ×100, 1 μg/ml leupeptin, 1 mM phenyl-methyl-sulfonyl-fluoride). Protein concentration was measured using a Bradford protein assay kit (Bio Rad Laboratories, CA, USA). Equivalent amount of protein was separated through 4%–15% sodium dodecyl sulfate polyacrylamide gel electrophoresis and blotted on a polyvinylidene difluoride membrane. Membranes were incubated in blocking buffer containing 5% milk in TBST (Tris-buffered saline with Tween 20) followed by incubation overnight with anti-tryptase and anti-CD117 primary antibodies, diluted 1∶1000 in blocking buffer; for control, we used a monoclonal anti-β-actin antibody 1∶5000 (Sigma Aldrich, St Louis, MO, USA). The secondary antibody used was peroxidase-conjugated goat anti rabbit and/or anti-mouse IgG from Jackson Immunoresearch Laboratories Inc. (West Grove, PA, USA). After wash and incubation with appropriate secondary antibodies, blots were developed using chemiluminescent horseradish peroxidase substrate (EMD Millipore, MA, USA). Tryptase and CD117 blots were re-probed for house-keeping protein beta actin to verify equal loading. Densitometric analysis was performed using ImageJ software from the NIH. Quantification was performed by comparing the relative ratios of C/β-actin to N/β-actin for each patient and calculating the mean changes. Graphically the differences are expressed on the ordinate as relative protein expression of tryptase (CD117)/β-actin. A total of 12 patients/24 samples (nevus and non-nevus skin) was analyzed.
Statistical analysis
Statistical analysis was performed using SPSS 20.0 (SPSS, Chicago, IL, USA). The results were expressed as mean ± SD or total number and percentage. One-way analysis of variance with Tukey for post hoc multiple comparisons was used to compare MC numbers between the groups, and Pearson's test was used to study the correlation between MC number and fibrosis in nevus tissue. The significance level was set as P ≤ 0.05.
RESULTS
Sample characteristics
We studied 49 nevus tissue samples; 12 uninvolved skin samples from patients with L/GCMN taken from areas adjacent to the nevus (perilesional) but without macro- or microscopic presence of nevus, and 6 were normal skin controls. Thirty-one patients (63.2%) were female; the patient ages ranged from 3 months to 16 years (mean 4.4 years); and 33 (67%) were classified as giant CMN. All lesions were excised for cosmetic reasons, and none of the children had a diagnosis of melanoma. Clinical features of the children and adolescents and the location of the tissue used in this research are presented in Table 1.
Clinical features and the location of the melanocytic nevus
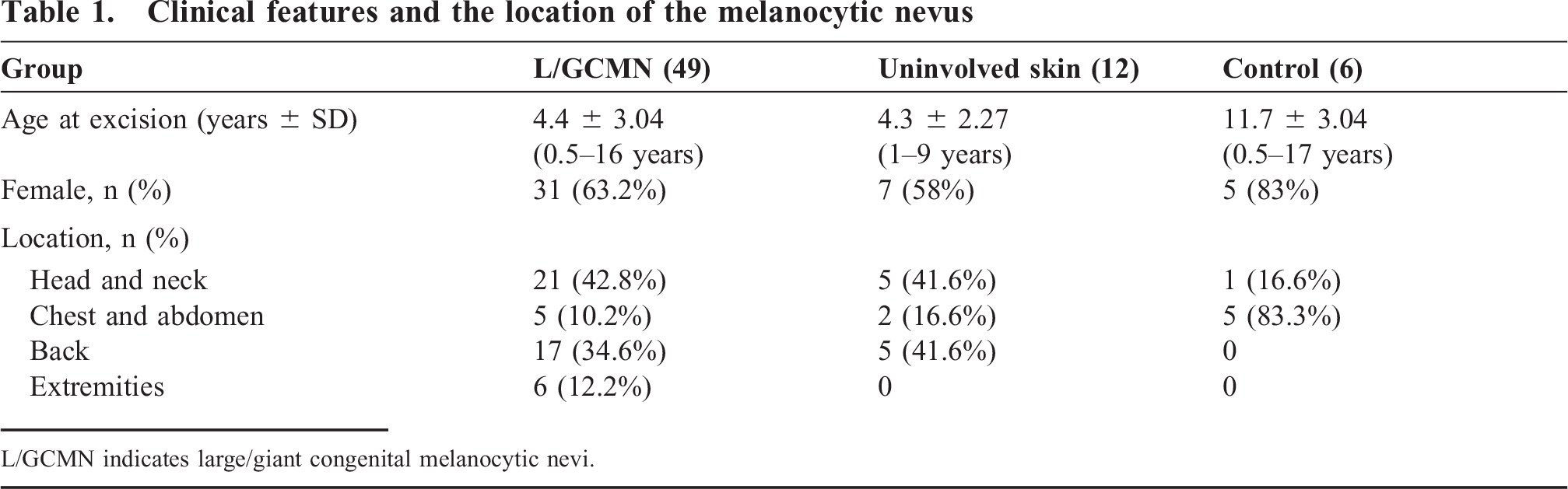
L/GCMN indicates large/giant congenital melanocytic nevi.
Mast cells number and distribution
The mean MC counts in L/GCMN tissues was higher (75.1 ± 35.3 MCs/mm2) than that found in control skin from individuals without L/GCMN (28.74 ± 8.4 MC/mm2); P = 0.001, but similar to the uninvolved skin tissues from patients with GCMN (53.74 ± 27.7 MC/ mm2), P = 0.109 (Fig. 1B,C). Figure 2 compares the MC number per mm2 in L/GCMN, uninvolved skin from patients with L/GCMN, and control skin.

Composite photomicrograph of immunohistochemical staining for tryptase showing an increased number of mast cells: (
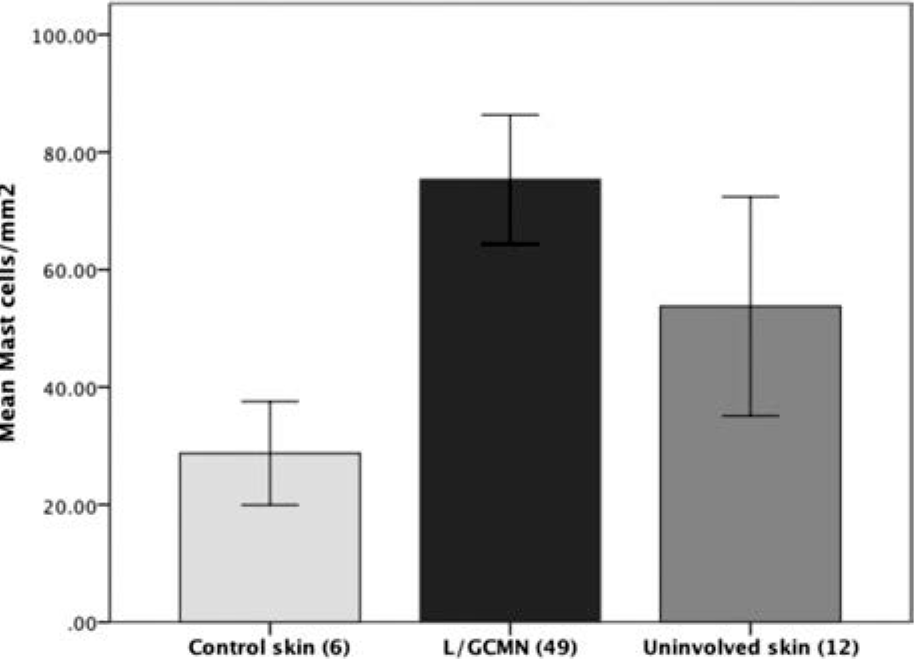
Bar diagram showing mean number of mast cells in three different skin tissue samples, using anti-tryptase antibody staining and expressed as mast cells/mm2. Nevus tissue from patients with large/giant congenital melanocytic nevi (L/GCMN) have increased number of anti-tryptase staining cells compared with skin from control (P = 0.001), but no differences were found between nevus and uninvolved skin from patients with L/GCMN (P = 0.119). One-way analysis of variance; Tukey for post-hoc multiple comparisons.
The similarity in MC counts between the L/GCMN and uninvolved skin tissues from patients with GCMN is supported by Western blot (WB) analysis of paired tissue samples from 12 patients, which showed similar tryptase amounts in nevus tissue (N) compared to uninvolved skin from the same patient (C) (Fig. 3).
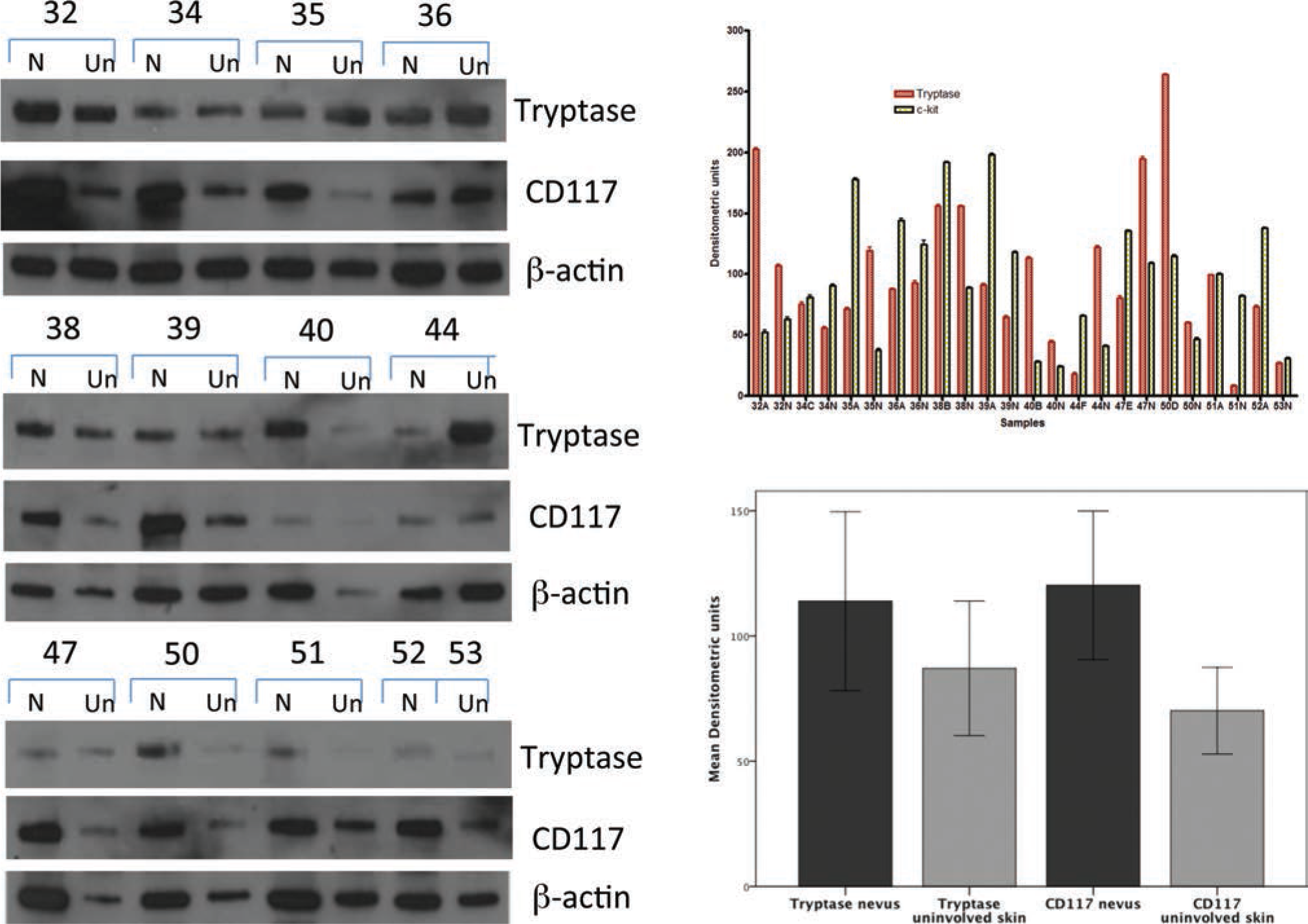
The receptor for SCF, CD117, showed cytoplasmic immunoreactivity and strong staining in MC (Fig. 1E), but melanocytes at the dermoepidermal junction and NC were also positive (Fig. 1F). CD117 WB analysis also supported this immunophenotype (Fig. 3C). It is interesting to note the CD117 immunoreactivity in NC increases in intensity in more superficial nevus layers.
We also found a trend toward a positive correlation of MC numbers and fibrosis, assessed by PR staining on the nevus samples, but this fell short of statistical significance (r = 0.245; P = 0.086); no difference in fibrosis was found between nevus and non-nevus skin from patients with L/GCMN (P = 0.136).
DISCUSSION
Our results confirm that L/GCMN associate with MC hyperplasia. We found an increased number of MC in nevi from L/GCMN patients compared with normal skin controls. It could be difficult to count with precision the number of MC on routine stains. The traditional metachromatic method using Giemsa staining showed increased numbers of MC in skin from patients with L/GCMN, but their granules were sometimes difficult to discriminate from melanin. For this reason, we chose to use IHC with anti-tryptase, which offers a more reliable method to count MC, yielding more sensitivity and specificity for the visual identification of MC in histologic sections. Furthermore, tryptase is expressed in all stages of MC development [15]. Immunohistochemistry for CD117 (c-kit) marks MC and also melanocytes and NC; all 3 cell types are CD117 positive.
An unexpected finding in this study was the presence of a significantly higher number of MC in uninvolved skin from these patients with L/GCMN compared to skin from controls. This was seen in normal appearing skin with no NC but adjacent to the resected nevus (perilesional). The association between melanocytic lesions and MC had been demonstrated in typical melanocytic nevi, dysplastic nevi, in situ, and invasive melanomas. However, the number of MC in L/GCMN has never been systematically studied. The size of our study group and the opportunity to compare nevus tissue with uninvolved skin from the same patients and with normal skin from children and adolescents without nevi provide statistical power and significance to our results.
The WB data on paired skin samples from L/GCMN patients were consistent with the histologic findings demonstrating that the relative abundance of mast cell tryptase was similar in nevus and uninvolved skin, indicating similar numbers of MC. Although CD117 was increased in the nevus sample compared to the uninvolved skin, the increased CD117 would be expected due to the greater presence of NC in the involved skin samples compared to the uninvolved areas of skin. We speculate that our findings could be due to genetic factors leading to proliferation of NC and MC. Mastocytes produce SCF, creating an autocrine loop for their own stimulation/growth as well as a potential paracrine loop for activating CD117 on neighboring nevus cells. Additionally, fibroblasts and keratinocytes can also produce SCF and may affect MC and NC proliferation. Other factors, including local substances produced by the nevus or its surrounding stroma, such as interleukin 3 (IL-3), may also have a role in increasing MC [16]. Our results are in agreement with the description by Biswas and colleagues [17], who report higher numbers of MC within and surrounding nevi compared with melanomas, and also with those of Carr and colleagues [10], who showed significant increase of MC densities in “neural nevi” compared with both neurofibromas and control nevi. However, neither of these studies [10,15] compared the nevus with normal skin from controls.
Our results are in keeping with what we previously described in a patient with a GCMN (“bulky perineal nevocytoma” variant) and pruritus of such intensity, that the patient presented with anemia secondary to bleeding due to scratching of her nevus [7]. Pruritus of CMNs may be difficult to control clinically, and our results support the notion that this finding may be observed in many patients with L/GCMN. As a matter of fact, severe pruritus in the nevus area is a frequent clinical complaint in patients with L/GCMN. Because MC are a source of histamine, their abundance in L/GCMN may be contributing to the severe pruritus.
Some authors have suggested that MC may have a role in the development of cutaneous tumors [18]. However, the clinical significance and role of MC in the development and progression of melanocytic tumors remains controversial. Mastocytes can contribute to both promotion and inhibition of tumor growth. This may be due to their heterogenous phenotype dictated by signals from the local milieu [19]. Participation of MC in tumor progression and in neoangiogenesis has been shown in skin tumors, including melanocytic nevi and melanomas [10,20–24]. Tryptase also has proangiogenic action with its ability to degrade connective tissue matrix and to activate PAR-2 receptors expressed by endothelial cells [25,26]. The PAR-2 receptor is expressed by nevi and melanomas [27], and an analogous mechanism could be operating in melanocytic lesions; however, this hypothesis requires further study. On the other hand, other MC tumor effects have also been documented because mediators released by them show an inhibitory effect on tumor growth and angiogenesis. Specifically tumor necrosis factor α, IL-1, and IL-6 have been reported to suppress melanoma growth. Activation of toll-like receptor 2 on MC and subsequent release of IL-6 results in the inhibition of tumor growth both in vitro and in vivo. Recruitment of natural killer cells and CD3+ T cells by MC has also been observed [28].
In conclusion, our results show that patients with L/GCMN have an increased number of MC in their skin within the nevus area and also in the uninvolved skin, compared to control skin samples from patients without nevi. These findings support the notion that patients with L/GCMN may carry generalized defects that result in the increase of 2 populations linked by their common response to the c-kit–SCF pathway. Analysis of their genetic features in regard to this pathway may shed light onto potential mechanisms explaining these findings. Furthermore, clinical manifestations of patients with L/GCMN, such as increased pruritus and hypertrophic scarring, may also be related to the larger numbers of MC observed in these patients.