
Abstract
Vitamin D is required for calcium absorption and normal bone mineralization; it has a key role in immune regulation against infections and is believed to be involved in immunomodulation in asthma. We did a retrospective analysis of 52 postmortem cases (aged 2 days to 10 years). Seventeen children had vitamin D deficiency (<25 nmol/L); 24 children had vitamin D insufficiency (25–49 nmol/L); 10 children had suboptimal vitamin D levels (50–79 nmol/L); and only 1 child had adequate levels (≥80 nmol/L). Three infants had fractures. Growth plate histology was abnormal in 10 cases with vitamin D deficiency (59%), but radiology was abnormal in only 3 of those cases. Eight infants (33%) with vitamin D insufficiency had abnormal histology, but radiology was normal in all cases. In 3 children hypocalcemia due to vitamin D deficiency was considered accountable for death; they all showed radiological and histological rickets: 2 babies had cardiomyopathy and a 3-year-old had hypocalcemic seizures. Children from all ethnic groups had a high proportion of low vitamin D levels. Vitamin D deficiency (the most common form of pediatric metabolic bone disease) is preventable and treatable. Profound hypocalcemia due to severe vitamin D deficiency can cause unexpected death in babies and young children. Measuring serum vitamin D levels postmortem may provide invaluable information on sudden unexplained death in ‘at-risk’ children. Vitamin D deficiency may be relevant in childhood asthma and in children with multiple infections and babies with bone fractures. Postmortem vitamin D levels are stable and easy to measure.
INTRODUCTION
Vitamin D deficiency has remained the most common form of metabolic bone disease that is entirely preventable yet is still on the rise in the United Kingdom and other western countries, especially among ethnic minority groups (dark skin, concealing clothing) [1]. Severe vitamin D deficiency, particularly with profound hypocalcemia, can cause substantial morbidity among ‘at-risk’ children, leading to life-threatening conditions and death if not diagnosed and treated in time. The pediatric population of Tower Hamlets in London, United Kingdom, has a low level of vitamin D in all ethnic groups, but these low levels are particularly widespread in children of Asian and African origin. In an internal audit conducted in our hospital in 2009 only 20% of white children, 4% of African and African-Caribbean children, and 3% of Asian children in whom total vitamin D was measured had levels of vitamin D measuring over 80 nmol/L. Total vitamin D includes vitamin 25–hydroxyvitamin D3 (naturally found in breast milk and fortified foods) and 25-hydroxyvitamin D2 (found in bottled milk and fortified foods).
As a consequence of our awareness of the low levels of vitamin D and the possible role of these low levels in terms of morbidity and mortality, we began to measure total vitamin D in our pediatric postmortem examinations as a diagnostic tool to help us understand why these children died [2].
Advice was sought from the East London Research Ethics Committee, which approved the nature of this case report series and the publications likely arising from it.
METHODS
A retrospective review of postmortems of infants and children in the pediatric autopsy files at The Royal London Hospital in North East London between July 2009 and April 2012 identified 183 cases. Of these, vitamin D status was known in 51 cases in children aged 2 days to 10 years. A single case with known vitamin D deficiency from 2002 was also included.
As part of the pediatric postmortem examination we take x-rays on children under 2 years of age and we sample the 6th rib in every case. We take blood for culture, toxicology, and biochemistry at the discretion of pathologist performing the postmortem. If in some cases there is not enough blood for all 3 tests, biochemistry is not done.
The growth plate is composed of a zone of resting cartilage with small individual scattered chondrocytes followed by a zone of proliferative cartilage in which the chondrocytes become aligned in the direction of growth as they enlarge and divide. This is followed by the hypertrophic zone, in which the chondrocytes become larger with more prominent nuclei but still maintain alignment in the direction of growth. The hypertrophic chondrocytes undergo apoptosis and cartilage then starts to become calcified and invaded by blood vessels to finally form the bony trabeculae. In a normal growth plate there is an orderly continuation of these zones, such that an imaginary slightly convex line may be traced on either side of the hypertrophic zone. In the case of rickets there is a lack of apoptosis of the hypertrophic zone, leading to a disorderly proliferation. The chondrocytes lose their columnar arrangement and the hypertrophic zone becomes thicker and disorganized. Tongue-like projections of cartilage extend into the spongiosa. The limit between the proliferative and hypertrophic zones also becomes irregular. Blood vessels are seen penetrating the hypertrophic cartilage zone [3].
In this study, abnormal histology was recorded when there was expansion of the hypertrophic zone with irregularity of the edges and loss of the columnar arrangement without tongues of chondrocytes or vascularization of the hypertrophic zone. The changes were considered mild when there was loss of columnar arrangement and mild expansion of the growth plate and moderate when there were obvious expansion and irregularities but when these features were short of the typical changes associated with rickets.
Vitamin D concentration is stable for several days after death, and in this study it was determined using a semiautomated solid-phase extraction tandem mass spectrometry 25-hydroxyvitamin D system. The method developed was able to measure 25-hydroxyvitamin D2 (25OHD2) and 25-hydroxyvitamin D3 (25OHD3) simultaneously in individual samples. Sample preparation (zinc sulfate protein crash) and solid-phase extraction steps (Waters Oasis elution plate) prior to LCMS analysis was performed with Tecan Freedom Evo 100 robotic instrumentation. Sample extracted in a microtiter plate was loaded into a tandem mass spectrometer and analyzed overnight. The assay used a 150-μL sample. Deuterated D3 + D3 was added to the patient sample prior to analysis to correct for procedural losses. The analytical range for both 25OHD2 and 25OHD3 was 5 to 250 nmol/L. Between-assay imprecision was <10% for the 4 IQC pools. The assay used NIST traceable calibrators and quality control material.
There is no strict definition of vitamin D “normal” and “abnormal” values. In our hospital, children with the combined levels of 25-OH vitamin D2 and vitamin D3 that were <30 nmol/L were considered vitamin D deficient and those with levels that were <80 nmol/L were considered vitamin D insufficient. However, the World Health Organization defines deficiency as <25 nmol/L and insufficiency as <50 nmol/L. For the purpose of this audit we considered vitamin D deficiency (VDD) to be <25 nmol/L, vitamin D insufficiency (VDI) to be 25–49 nmol/L, vitamin D suboptimal (VDS) to be 50–79 nmol/L, and vitamin D adequate or normal (VDN) to be >80 nmol/L. Calcium, phosphate, and parathyroid hormone were not measured as they are not stable after death.
RESULTS
Fifty-two children with known vitamin D status were identified (Table 1). We are not aware of whether or not any of the breast-feeding mothers or any of the children were on vitamin D supplementation. A summary of the findings is shown in Table 2.
Summary of all cases
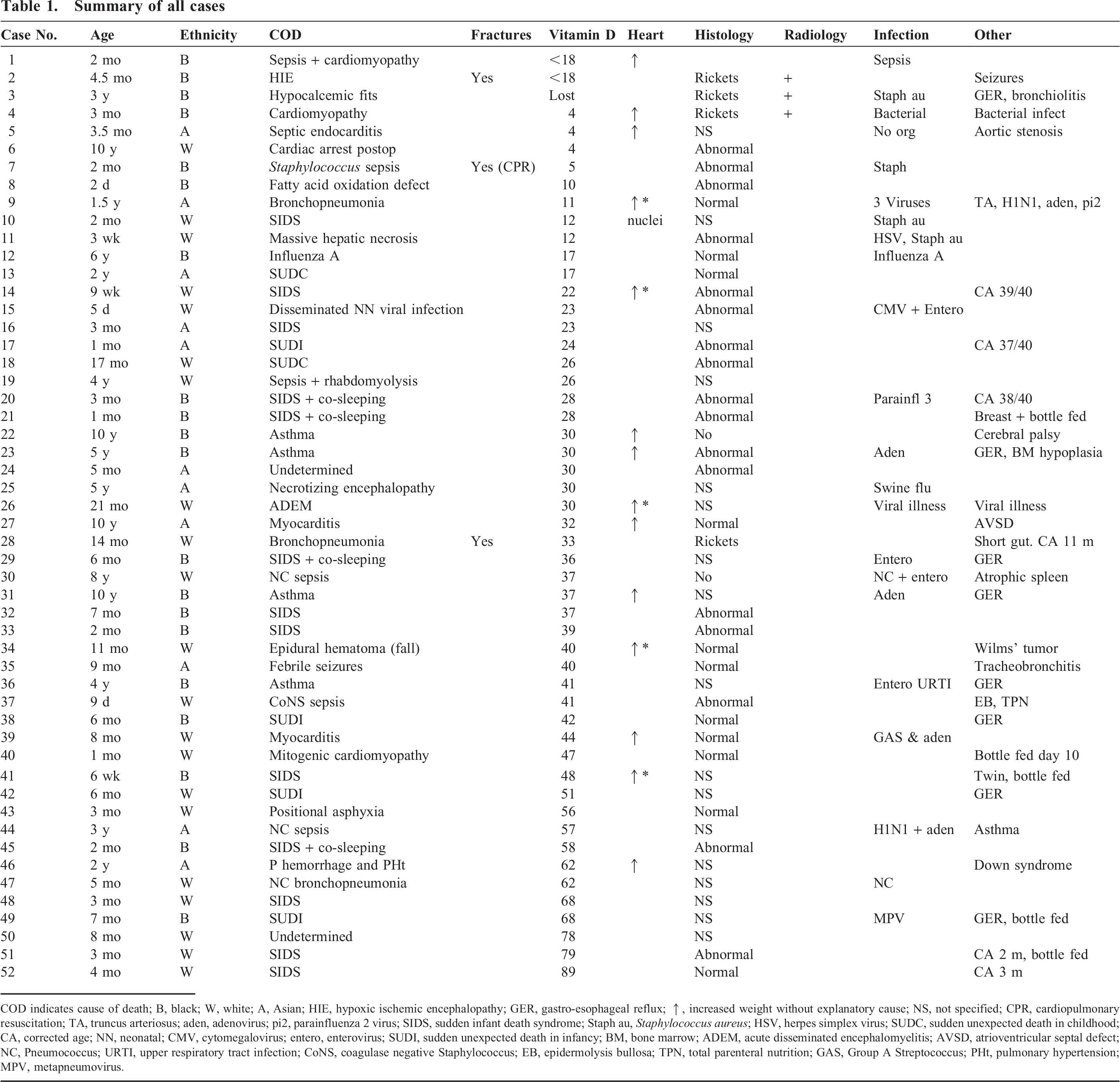
COD indicates cause of death; B, black; W, white; A, Asian; HIE, hypoxic ischemic encephalopathy; GER, gastro-esophageal reflux; ↑, increased weight without explanatory cause; NS, not specified; CPR, cardiopulmonary resuscitation; TA, truncus arteriosus; aden, adenovirus; pi2, parainfluenza 2 virus; SIDS, sudden infant death syndrome; Staph au, Staphylococcus aureus; HSV, herpes simplex virus; SUDC, sudden unexpected death in childhood; CA, corrected age; NN, neonatal; CMV, cytomegalovirus; entero, enterovirus; SUDI, sudden unexpected death in infancy; BM, bone marrow; ADEM, acute disseminated encephalomyelitis; AVSD, atrioventricular septal defect; NC, Pneumococcus; URTI, upper respiratory tract infection; CoNS, coagulase negative Staphylococcus; EB, epidermolysis bullosa; TPN, total parenteral nutrition; GAS, Group A Streptococcus; PHt, pulmonary hypertension; MPV, metapneumovirus.
Summary of findings

Histology indicates abnormal histology; Radiology, abnormal x-rays; W, white; A, Asian; B, black. Histology indicates all rib growth plate abnormalities, from mild to obvious rickets. Radiology indicates characteristic changes of rickets.
Abnormal heart without another explanation.
Vitamin D deficiency (<25 nmol/L)
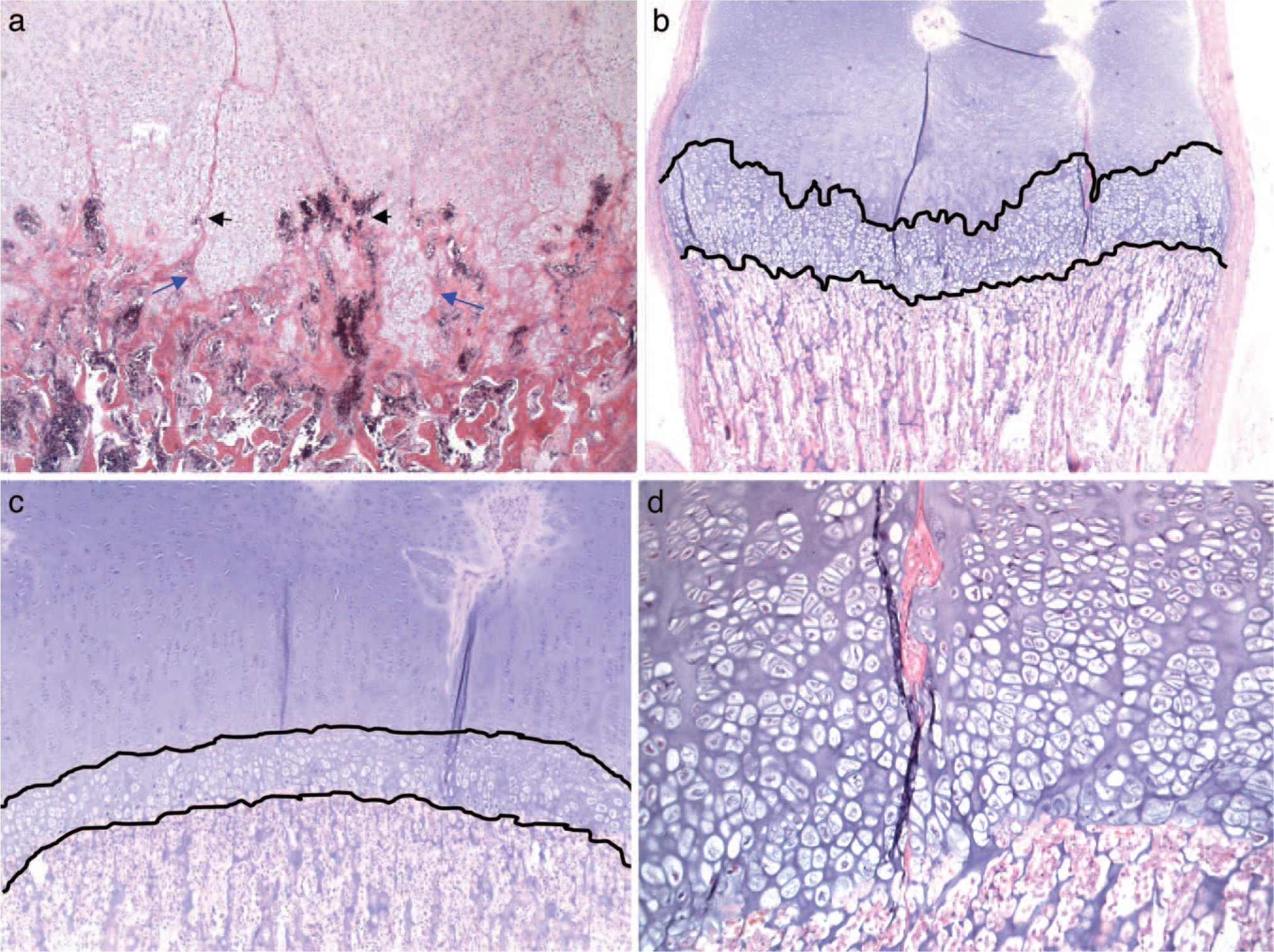
Seventeen children aged between 5 days and 10 years were VDD. Five children were white (30%), 6 were Asian (35%), and 6 were black (35%). Only 3 children had radiological evidence of rickets (18%), seen as metaphyseal flaring and cupping. However, histological examination of the rib growth plate independently conducted by 2 pediatric pathologists demonstrated abnormalities in another 7 cases, giving a total number of histological abnormalities (as described in Methods) as 10 (of 17) cases (59%). Three cases with radiological evidence of rickets showed typical rickets histology: irregular border between the growth plate and the primary spongiosa, invasion of the growth plate by blood vessels, widening of the growth plate, architecture cartilage disarray, and tongues of unmineralized cartilage extending into the metaphysis (Fig. 1a).
(
Seven cases without radiological evidence of rickets had obvious growth plate abnormalities ranging from mild to moderate (Fig. 1b,d).
Two infants, one of which was 4.5 months old with radiological rickets (case 2) and another that was 2 months old without radiological rickets (case 7), had multiple fractures. Case 2 had symptom-free healing fractures in life, and case 7, a 6-week-old infant, had 11 acute rib fractures (8 of them posterior), interpreted by a forensic pathologist and a pediatric pathologist to be due to cardiopulmonary resuscitation. Both infants were black and exclusively breastfed. The histology of the ribs in the 1st case showed typical changes of rickets, while the younger baby had less marked growth plate abnormalities.
In 3 (cases 1, 4, 14) of the 17 VDD (<25 nmol/L) cases without congenital heart disease the heart had an increased weight for age (including 2 who had dilated cardiomyopathy), while another case had myocardial cell hypertrophy (case 10) without heart weight increase, giving a total of 4 cases (24%) with heart abnormalities. There was no obvious correlation between the degree of vitamin D level and the increase in heart weight. Bone markers the day before death were available in case 6 and they were all normal.
The cause of death was heart disease (alone or combined with infection) in 4 children: postoperative cardiac arrest (case 6), septic endocarditis (case 5), 2 cardiomyopathies (cases 1 and 4), one of them with infection. Neurological causes (seizures) contributed to death in 2 children (cases 2 and 3), and infection was the cause of death in 5 children, as follows: staphylococcal sepsis (case 7), bronchopneumonia (case 9), massive hepatic necrosis due to herpes simplex virus (HSV) infection (case 11); influenza A (case 12), and disseminated neonatal cytomegalovirus and enteroviral infection (case 15). The death in 1 case was attributable to metabolic disease (case 8), and sudden infant death, sudden death in childhood, and/or sudden unexpected death in infancy (SIDS/SUDC/SUDI) was the cause of death in 5 children (cases 10, 13, 14, 16, 17).
Vitamin D insufficiency (25–49 nmol/L)
Twenty-four children with ages ranging between 9 days and 10 years were VDI. Nine children were white (37%), 4 were Asian (17%), and 11 were black (46%). None of these children had radiological evidence of rickets, as defined before. However, histological abnormalities in the rib growth plate were seen in 8 (33%) children: in 6 cases there was irregularity of the growth plate, with changes similar to those seen in the deficiency group. However, 1 case (case 28) with multiple healing fractures had histological rickets; this was a very premature child with short gut syndrome. Interestingly, despite the obvious histological metaphyseal irregularities, the x-rays did not show typical changes of rickets, although the bones were considered hypomineralized by 2 pediatric radiologists.
Three children without asthma or a cardiac cause of death (cases 26, 34, 41) had an enlarged heart (13%).
The cause of death was asthma in 4 cases (cases 22, 23, 31, 36), and it was infection in 4 cases, as follows: septic-induced rhabdomyolysis (case 19), 1 Streptococcus pneumonia sepsis (cases 30); 1 neonatal coagulase-negative Staphylococcus sepsis (case 37), and 1 bronchopneumonia (case 28). A cardiac condition with or without infection was the cause of death in 3 (cases 27, 39, 40), and a neurological issue was the cause of death in 4 cases, as follows: necrotizing encephalopathy (case 25), acute disseminated encephalomyelitis (case 26), epidural hematoma due to a short-distance fall (case 34), and febrile seizures (case 35). Nine deaths were attributed to SIDS/SUDI/undetermined (cases 18, 20, 21 24, 29, 32, 33, 38, 41).
Suboptimal vitamin D (50–79 nmol/L)
Ten children ranging in age between 3 months and 3 years had vitamin D levels between 50 and 79 nmol/L. Radiology was normal in all. However, 2 cases (45 and 51) had an abnormal growth plate. These were babies (2 and 3 months old, respectively) that were bottle-fed and may have had lower levels at birth. Increased heart weight was found in 1 case, but this was attributed to pulmonary hypertension, which was the cause of death (case 46). The cause of death in the other cases was infectious in 2 cases (both by Streptococcus pneumonia, cases 44 and 47); positional asphyxia was the cause of death in 1 case (case 43), and SIDS/SUDI or undetermined causes were involved in 6 (cases 42, 45, 48–51).
Normal vitamin D (>80 nmol/L)
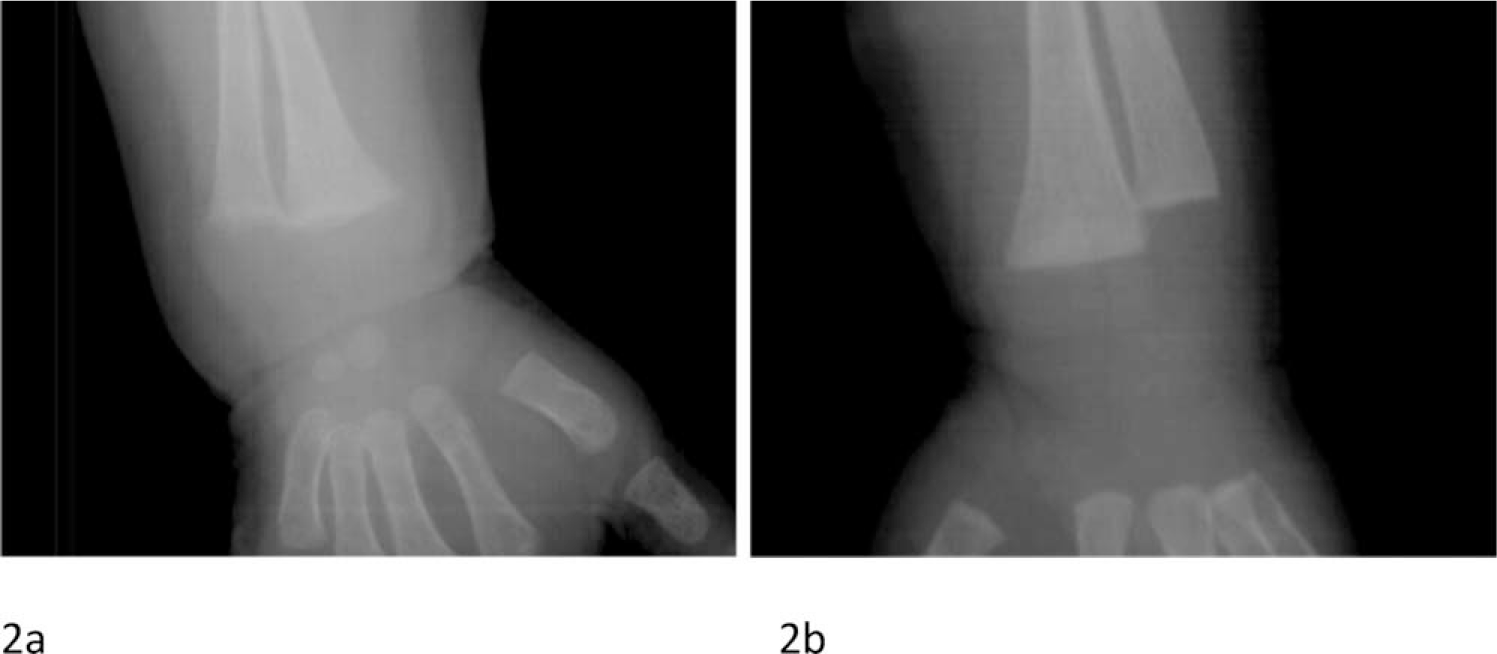
Only 1 case (case 52), a 4-month-old white baby (corrected age 3 months) who died of SIDS had normal levels of vitamin D; histology (Fig. 1c) and radiology were normal (Fig. 2b) in this case.
(
Many of the infections in all groups with less than 80 nmol/L of vitamin D were attributable to more than 1 microorganism or coexisted with another cause of death: a child with dilated cardiomyopathy and sepsis (case 1), aortic stenosis complicated by endocarditis (case 5), and a myocarditis with adenovirus and group A streptococcal infection (case 39). Three cases from the asthma patient group had viral infections (cases 23, 31, 36), 2 of the neurological deaths were related to a previous infection (cases 3 and 26), and another case was secondary to swine flu (case 25). Three SIDS case patients had viral infections (cases 20, 29, 49), and 1 had Staphylococcus aureus of unknown significance (case 10). In addition, there were 2 pneumococcal infections associated with a viral infection (case 30 with enterovirus and case 44 with swine flu and adenovirus), 1 case of bronchopneumonia associated with 3 viruses (case 9), 1 neonate with a double viral infection (case 15), and another (case 11) involving HSV and staphylococcal infection.
According to the children's ethnicity, 24% of white children, 32% of black children, and 50% of Asian children had VDD; 43% of white children, 58% of black children, and 33% of Asian children had VDI; and 28% of white children, 10% of black children, and 17% of Asian children had VDS. Only 5% of white children, but no black or Asian children, had normal levels.
DISCUSSION
Vitamin D is a pro-hormone essential for normal calcium absorption from the gut, and vitamin D deficiency is associated with rickets in growing children and osteomalacia in adults. Rickets is the failure of mineralization of growing bone and cartilage [4].
Vitamin D is crucial in calcium and phosphorus homeostasis. In addition to bone mineral metabolism, adequate levels of 25(OH)D are needed for regulation of physiological functions, and vitamin D receptors (VDRs) are found in most tissues.
The major endogenous, synthetic source of vitamin D for humans is the epidermis. Vitamin D3 is produced in the skin by a ultraviolet B–mediated reaction that converts 7-dehydrocholesterol to previtamin D3. This in turn undergoes a subsequent conversion to vitamin D3, also in the skin. From the skin, vitamin D3 finds its way into the general circulation. In the hepatic parenchyma, vitamin D3 is converted to 25-hydroxy-vitamin D3 [5].
Severe chronic vitamin D deficiency leads to overt skeletal abnormalities in children, typically defined as rickets. However, there are large number of infants, children, and adolescents who are vitamin D insufficient but who have no apparent skeletal or calcium metabolism abnormalities [6].
In response to the decline in blood calcium levels, parathyroid hormone (PTH) is produced in order to maintain calcium within the range required for normal nerve and muscle function. At the renal level, there is calcium retention and phosphate excretion. An initial increase in the production of 1,25-dihydroxy-vitamin D [1,25(OH)2D] together with PTH releases both calcium and phosphate from bone through an increase in osteoclastic bone resorption. 1,25(OH)D also acts at the level of the small intestine to increase calcium uptake. If there is continuing poor supply of vitamin D, 1,25(OH)2D production in the proximal tubules diminishes gradually, and this may also contribute to the rise in PTH through lack of feedback at the level of PTH gene transcription [1].
In young children vitamin D deficiency results in rickets and skeletal growth retardation, and in some cases this will be accompanied by hypocalcemia. In over 70% of children with rickets and over 90% of children with hypocalcemia vitamin D concentrations are <12.5 nmol/L [4].
Lack of sun exposure is the main cause of vitamin D deficiency. Factors contributing to vitamin D deficiency include indoor activities during daylight hours, industrial pollution, inadequate skin exposure (either as a result of darker skin, which requires longer exposure, or dress codes that limit skin exposure), and the use of strong sunscreen protection [1].
Despite adequate sunlight exposure, nutritional rickets due to low calcium consumption develops in some children beyond the 1st year of life. Evidence from several tropical countries indicates that many children with nutritional rickets have adequate vitamin D status. Calcium-deficiency rickets likely occurs in many tropical countries but may be misdiagnosed as vitamin D deficiency in the absence of laboratory measurement of 25-hydroxyvitamin D. Calcium-deficiency rickets was first reported and is still occasionally described among American and European children whose milk intake is restricted [7].
All causes of malabsorption may contribute to vitamin D deficiency, including short gut syndrome, Crohn's disease, celiac disease, cystic fibrosis, and primary biliary fibrosis. Rickets is well known in children's conditions such as biliary atresia [8].
Phosphate plays a critical role in skeletal integrity and mineral metabolism. Phosphate homeostasis is largely regulated by proximal renal tubular absorption. Abnormalities of phosphate transport are seen in 3 forms of hereditary hypophosphatemic rickets [9].
There is variable presentation of rickets depending on age at onset and individual genetic polymorphisms [10]. Vitamin D deficiency may cause apnea, hypocalcemic seizures, tetany, delayed motor milestones, skeletal deformities, and fractures. It has also been reported to lead to an increased risk of other childhood disorders, such as type I diabetes and bronchial asthma, frequent lower respiratory infections, and tuberculosis [11–13].
Two of the children who presented with seizures had low calcium: one was borderline and the other had severe hypocalcemia. Both had radiological and histological rickets. Hypocalcemic symptoms occur in patients with rapid growth rates (children <1 year of age and adolescents). Symptoms generally occur when the ionized calcium level is less than 1 mmol/L, and they mainly depend on how quickly the serum calcium falls. Hypocalcemia increases neuronal excitability, causing tetany, muscle spasms, and seizures; in infants it may present as upper airway obstruction (laryngospasm, stridor, and apnea).
Two children had severe dilated cardiomyopathy. One had been diagnosed with rickets-related cardiomyopathy in life (case 1) and the other was diagnosed postmortem (case 4). In addition, in 4 other children (in whom there was no other apparent reason for the increase in weight) the heart weight was increased for age, and 1 child with a normal-sized heart had histological cardiomyocyte hypertrophy. Overt cardiomyopathy is a very rare but life-threatening complication of rickets. Cardiomyocytes have VDRs, and calcium has long been known as an inotropic substance essential for cardiac muscle function. While cardiomyopathy develops in the context of chronic hypocalcemia, other forms of cardiac dysfunction occur during acute reduction in serum calcium levels; cardiac contractility may be reduced and the QT interval prolonged. Cardiac manifestations are reversible with vitamin D and calcium treatment, and the survivors have a good prognosis.
Infection, either as a cause of death or as an additional finding, was present in 9 children with VDD and 9 children with VDI, as well as in 3 children with VDS. Vitamin D plays an important role in both innate and adaptive immunity. Vitamin D is considered to be a necessary intermediate in the generation of antimicrobial peptides by monocytes-macrophages. Activated inflammatory cells have VDRs. Rickets during infancy has been associated with a higher prevalence of lower respiratory tract infections. Vitamin D may also promote antiviral activities [13].
Four children died as a consequence of asthma. Correlations between lower vitamin D levels and markers of allergy have been described in childhood asthma. Vitamin D enhances the anti-inflammatory effects of glucocorticoids. Lower vitamin D levels contribute to increasing asthma severity, and when these levels are low there is a need for higher doses of glucocorticoids to achieve treatment effect [14].
In established rickets, there is expansion of the late chondrocyte layer secondary to impaired apoptosis of hypertrophic chondrocytes. Maturation of the growth plate depends on phosphate-regulated apoptosis of hypertrophic chondrocytes via activation of the caspase 9–mediated mitochondrial pathway [15,16]. However, as shown in our observations, earlier changes, which are easily distinguished from normal growth plate (Fig. 1b–d), can be seen in a large percentage of infants with vitamin D levels <25 nmol/L (59%) and a smaller percentage of infants with vitamin D levels ranging between 25 and 49 nmol/L (33%) before the radiological manifestations of rickets are evident (Fig. 2a). This was well described in the old literature. Wimberger [17] compared radiological pictures and histological sections from the same bone at postmortem and found that the interval between the 1st histological rachitic changes and the 1st radiological change was as long as several weeks. As this is an observational study based on postmortem reports of the growth plate histology, more detailed analysis of the morphological changes is outside the scope of this article.
Histological changes were reported in 10 cases with VDD, 8 cases with VDI, and 2 cases with VDS. Histological abnormalities were identified in 59% of infants under 6 months of age and in 27% of those aged 6 to 12 months. A single case with histological and radiological rickets was in the >1-year-old group. Four cases (cases 2, 3, 4, 28) had marked rickets changes in the growth plate, but only 3 of those (cases 2, 3, 4) had radiological evidence of rickets. Perez-Rosello and colleagues [18] report a single case in which all radiologists agreed that there was demineralization and that child had severe vitamin D deficiency. As all children were alive, no histological studies of the bones were done [18]. Schilling and colleagues [19] describe 9 patients with vitamin D deficiency (considered to be <50 nmol/L) among a group of 118 children with fractures aged 6 days to 22 months. The age of the children with vitamin D deficiency was not specified. They did not see radiographic demineralization in any of these children. These were also cases in which the bone histology was not completed [19]. Several other authors [20–22] have described fractures as the 1st presentation in rickets.
Twelve of the 17 children with VDD (<25 nmol/L) and 5 of the 24 children with VDI (25–49 nmol/L) were under 6 months of age (Fig. 3). In many of these deficient babies there was a recorded history of being exclusively breastfed. In the only instance in which the mother's vitamin D level was tested, she also had vitamin D deficiency (24 nmol/L). A 3.5-month-old baby with a corrected age of 2 months who had normal vitamin D levels and some abnormalities in the growth plate had been fed by endotracheal tube and formula milk since birth.
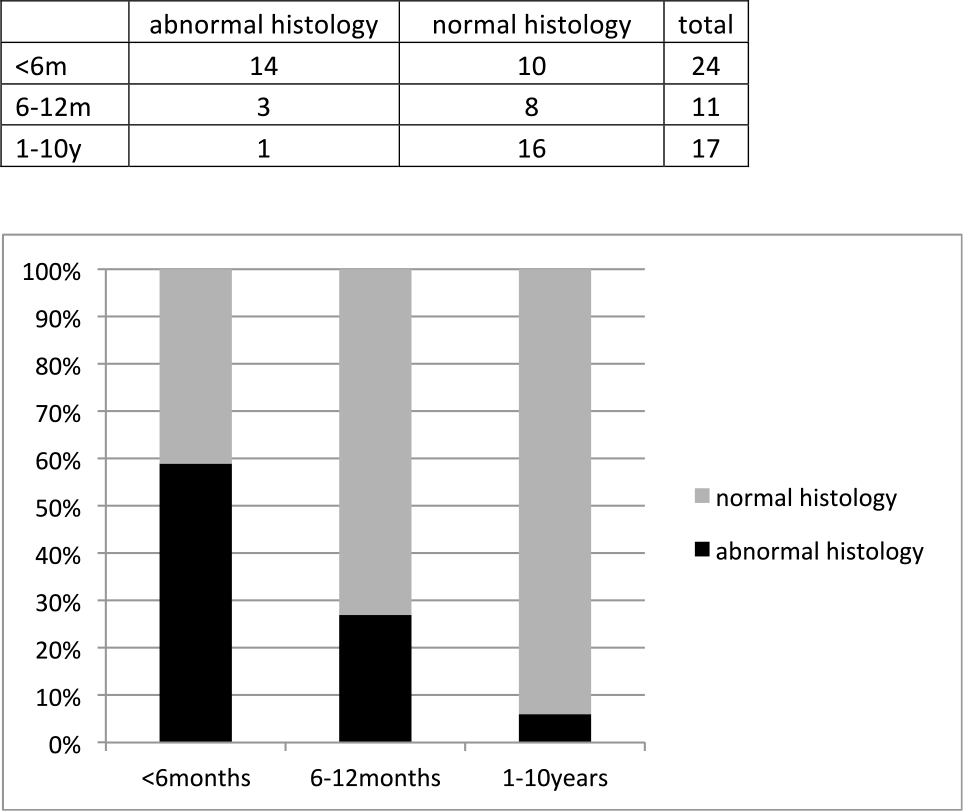
Rib growth plate histology according to age. Total numbers in table and percentages in graphic.
Vitamin D deficiency during pregnancy has significant implications for fetal development: calcium is essential for many biological pathways, including muscle contraction, 2nd messenger formation, secretion of neurotransmitters and hormones, and blood coagulation, and it is an important component of the skeleton. At birth the body contains approximately 30 g of calcium; this amount increases to approximately 1000 g in adults; 99% of the body calcium is in the skeleton. Skeletal growth is a dynamic process that requires 25 to 30 g of calcium to be transferred from the mother to the fetus during pregnancy [23]. This is achieved mainly through increased intestinal calcium absorption facilitated by vitamin D. The pregnant woman will leach nutrients from her bones and tissues in order for the pregnancy to survive, but the net amount of vitamin D transferred to the fetus will be reduced, which may affect fetal bone mineralization and growth. It has been shown that low maternal vitamin D status during pregnancy is associated with splaying of the distal metaphysis of the fetal femur [24], and intrauterine fractures due to congenital rickets have been described in the literature [25]. During the last trimester approximately 80% of fetal skeletal mineral is deposited: more than 150 mg calcium/kg body weight and 70 mg phosphate/kg body weight are provided every day to the growing fetus through active transplacental transport. A fetus that was vitamin D deficient during pregnancy will likely be born with near-normal serum calcium concentrations and normal skeletal morphology but risks developing rickets within the 1st weeks or months of life, especially if exclusively breastfed [26]. In most women the amount of vitamin D in breast milk is too small to prevent vitamin D deficiency in the breastfed infant. Thus, in early infancy, the vitamin D status of breastfed infants depends on the vitamin D transferred across the placenta during fetal life. From then on, because of the short half-life of vitamin D (2–3 weeks) and of the active form of vitamin D (4 hours) [4], an external supply of vitamin D through breast milk (unlikely in a vitamin D–deficient mother) or infant supplementation or the endogenous production through sunlight exposure is necessary to maintain vitamin D sufficiency.
Our results are similar to those reported in a recent audit of postmortem-measured vitamin D; the authors [27] found abnormal radiology in 19% of cases, but there was abnormal histology in 69% of cases.
CONCLUSIONS
Vitamin D deficiency, which is the most common cause of rickets, has made an unfortunate comeback in the United Kingdom, especially, but not exclusively, in ‘at-risk’ ethnic minority groups. Rickets can manifest at many levels, from mild biochemical abnormalities to growth delay and skeletal deformities, from dilated cardiomyopathy to acute and sudden events (such as seizures and tetany). Rickets may also present as fractures and may initially raise suspicion of abuse. Biochemical and histological abnormalities appear earlier than radiological abnormalities. Vitamin D levels, together with other markers of bone disease, should be measured in all infants presenting with single or multiple fractures, regardless of the radiological appearance of the metaphyses, and rickets-related fractures should be considered in cases with biochemical abnormalities; however, it is worth noting that bone markers may be normal, even with positive histological changes. In addition, severe rickets can be life threatening, and if not recognized early on, it can cause unexpected death from seizures or cardiomyopathy in babies and young children.
While vitamin D deficiency (mostly through low blood calcium) was directly responsible for a small number of deaths (dilated cardiomyopathy and fatal seizures), its role in morbidity appears to be more widespread. Postmortem vitamin D results may be helpful in understanding the pathophysiological mechanisms of the disease that caused the death and in directing further investigations into the cause of death since radiological evidence is not a reliable indicator.
The main limitation of this study is that this is a retrospective descriptive observation. The aim of the study is to raise awareness of the importance of measuring vitamin D and of examining the rib growth plate in pediatric postmortems. An additional properly designed research study needs to be done in order to address the reproducibility by different pathologists of the changes observed, to perform morphometrical analysis to quantify these changes, and to determine the clinico-pathological correlations.
In our experience, measuring serum vitamin D levels postmortem may provide invaluable information on sudden unexplained death in children, in children dying from asthma, and in babies with fractures. Vitamin D levels are easy and inexpensive to measure, and the information obtained may assist in establishing the cause of death. Low vitamin D may prove to be a significant risk factor in various morbidities.
Footnotes
ACKNOWLEDGMENTS
Thanks to Dr Liina Kiho for recording growth plate histology in her cases and to Dr Benjamin Jacobs and Dr Esin Kotiloglu-Karaa for helpful comments.