
Abstract
Whole slide imaging (WSI) is rapidly transforming educational and diagnostic pathology services. Recently, the College of American Pathologists Pathology and Laboratory Quality Center (CAP-PLQC) published recommended guidelines for validating diagnostic WSI. We prospectively evaluated the guidelines to determine their utility in validating pediatric surgical pathology and cytopathology specimens. Our validation included varied pediatric specimen types, including complex or less common diagnoses, in accordance with the guidelines. We completed WSI review of 60 surgical pathology cases and attempted WSI review of 21 cytopathology cases. For surgical pathology cases, WSI diagnoses were highly concordant with glass slide diagnoses; a discordant diagnosis was observed in 1 of 60 cases (98.3% concordance). We found that nucleated red blood cells and eosinophilic granular bodies represented specific challenges to WSI review of pediatric specimens. Cytology specimens were more frequently discordant or failed for technical reasons, with overall concordance of 66.7%. Review of pediatric cytopathology specimens will likely require image capture in multiple focal planes. This study is the first to specifically evaluate WSI review for pediatric specimens and demonstrates that specimens representing the spectrum of pediatric surgical pathology practice can be reviewed using WSI. Our application of the proposed CAP-PLQC guidelines to pediatric surgical pathology specimens is, to our knowledge, the first prospective implementation of the CAP-PLQC guidelines.
Keywords
INTRODUCTION
Whole slide imaging (WSI) has been implemented with increasing frequency in research applications and in clinical practice, primarily outside of the United States [1–6]. The clinical utility of WSI has been limited in the United States, in part by the lack of regulatory approval for its use in primary diagnosis. The U.S. Food and Drug Administration has classified WSI as a class III medical device that requires validation and approval before use in primary diagnosis [7]. Based on a review of the literature and expert consensus, guidelines for validation of WSI were recently proposed by the College of American Pathologists Pathology and Laboratory Quality Center (CAP-PLQC) [8]. The CAP-PLQC guidelines comprise 12 statements that outline recommendations for when validation studies should be performed, the scope of what should be validated, and how validation studies should be conducted and documented. The CAP-PLQC guideline statements are noteworthy, both as a milestone in the development of WSI for diagnostic use and also for what is not included. The guidelines do not specify technical parameters for image capture or viewing workstations; rather, they focus on the goals of validation studies. This aspect of the guidelines offers laboratories flexibility in selecting and implementing WSI platforms. Validation studies can be attempted with existing systems, minimizing requirements for new capital investments in scanners and computer equipment, including monitors. Computer resources can also be minimized by customizing the captured image resolution for the intended use, and image compression and management systems can be employed to further manage large WSI files. Additionally, the CAP-PLQC statements leave specific judgments about the success or failure of the validation attempt to the medical judgment of individual laboratories. This aspect of the guidelines allows pathologists greater flexibility in customizing the evaluation of WSI systems to a specific intended use.
Many studies have compared the concordance of diagnostic reviews using glass slides and WSI for various specimen types and have demonstrated that WSI can show high concordance with glass slides, including the publications evaluated by CAP-PLQC as the basis for developing the validation guideline statements [1–3,9–31]. The CAP-PLQC meta-analysis of these studies further demonstrated that WSI review is capable of producing highly accurate diagnoses and high concordance with conclusions reached through examination of hematoxylin-eosin (H&E)–stained glass slides review [8]. In this first prospective evaluation of the practical implementation of the CAP-PLQC guidelines statements, we attempted to validate 2 specimen types: pediatric surgical pathology and pediatric cytopathology. This also represents the first dedicated study of WSI review for pediatric specimens. Herein, we detail our experience with the CAP-PLQC validation guidelines, highlighting technical challenges and differences in the microscopic features that pathologists were able to identify by glass slide or WSI review.
METHODS
Cases previously reviewed as glass slides for clinical purposes at Nationwide Children's Hospital, Columbus, OH, USA, were selected for digital capture and WSI review. Cases were chosen both randomly and nonrandomly to reflect the spectrum and complexity of our pediatric pathology practice. Randomly selected consecutive cases were identified first, and then nonrandomly selected cases were chosen to ensure the inclusion of additional important yet less common diagnoses not present among the randomly selected cases. The specimen types represented in the cases reviewed by WSI are listed in Table 1. At the time of WSI review, all cases were at least 3 months from previous glass slide review, and some nonrandomly selected cases were up to 6 years from clinical review. For the vast majority of cases, the time interval between glass slide review and WSI review (the “washout period”) was 4 to 5 months.
Selected specimen types
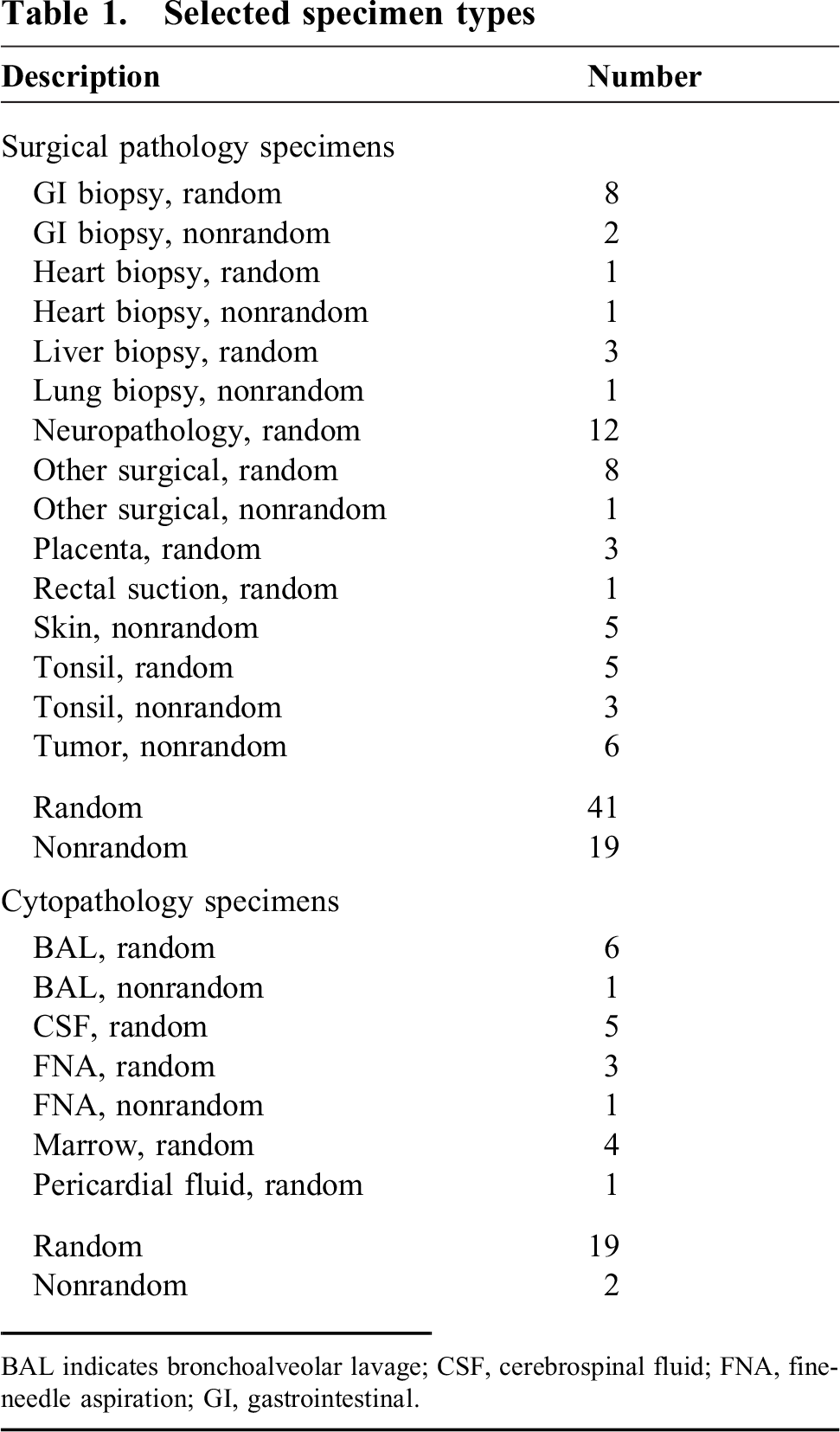
BAL indicates bronchoalveolar lavage; CSF, cerebrospinal fluid; FNA, fine-needle aspiration; GI, gastrointestinal.
All slides were imaged in a single plane using an Aperio Model XT digital slide scanner. The captured area of the slide was customized to include only the area containing tissue, and digital images were reviewed to confirm that the digital image contained the entire specimen. Cytology cases were not screened by a cytotechnologist prior to glass or virtual slide review. Digital capture of cytospin slides and small biopsy samples (such as gastrointestinal or endomyocardial biopsy specimens) was performed at the equivalent of ×40 objective magnification, using an Olympus ×20 objective (UPlan SApo ×20/0.75 ∞/0.17/FN26.5) in combination with a ×2 optical magnification changer. To limit large digital files, slides other than cytospin slides and small biopsy specimens were captured at ×20 magnification using only the ×20 objective. The resolutions of WSI images captured at ×20 and ×40 were 0.5 μm/pixel and 0.25 μm/pixel, respectively. The digital slide images generated by the slide scanner were 24-bit color and employed JPEG compression with a quality factor of 30 (on a scale of 1 to 100, a higher number indicates higher quality). This quality factor results in a compression ratio of approximately 23 to 1.
Captured cases were de-identified by relabeling them with consecutive numbers and registered in the laboratory information system with only the patient age, gross description of the specimen, and clinical history as it appeared in the final pathology report; all patient-specific information and any references to previous specimens were redacted. The resulting de-identified WSI cases were reviewed by the same pediatric pathologist who had previously completed clinical evaluation of the corresponding glass slides at Nationwide Children's Hospital. In the spirit of providing the case to the pathologist in a similar environment to the anticipated clinical application, pathologists were provided with the de-identified information from the laboratory information system and initially only given access to H&E-stained WSI, frozen sections, and intraoperative touch preparations for each case.
WSI were reviewed using ImageScope software (Leica Biosystems, Buffalo Grove, IL, USA) on desktop computers equipped with 1280- × 1024-pixel resolution Dell monitors (Dell Corporation, Austin, TX, USA). WSI corresponding to additional stains ordered by the pathologist (special stains and immunohistochemical stains) as well as ancillary test results were available to the pathologist on request after initial WSI review of the H&E-stained slides.
We used stringent criteria to score differences observed in WSI review; we chose to score differences in the diagnosis or diagnostic category as discordant, irrespective of the impact on patient care by current treatment protocols. The results of WSI review were compared with the original glass slide diagnoses and were scored as (1) essentially identical (differences with minimal impact on the interpretation of the report); (2) minor difference (variations in the microscopic features identified, but without a change in the diagnosis); (3) major difference (a different diagnosis or different diagnostic category); or (4) unsatisfactory for evaluation (resulting from either failure to capture the digital image or image quality that was not acceptable to the reviewing pathologist). Diagnoses were considered concordant when scored as either “essentially identical” or “minor difference.” Diagnoses were considered discordant when WSI review resulted in either a major difference or WSI review was unsatisfactory to render a diagnosis for any reason.
RESULTS
Successful WSI review of pediatric surgical pathology
WSI evaluation of 60 surgical pathology cases (130 specimen parts represented in 473 slides) resulted in high concordance with the diagnoses rendered by prior glass slide review. A discordant diagnosis was seen in only 1 case (1.7% of cases, 98.3% concordance), with 3 parts each resulting in the same discordant diagnosis (2.3% of parts, 97.7% concordance) (Table 2). The discordant case was a brain tumor originally classified on glass slide review as a pilocytic astrocytoma and diagnosed as a glioneuronal tumor after review by WSI. This difference would not have influenced the clinical management of the patient according to current treatment protocols. The difference in this diagnosis was primarily attributable to eosinophilic granular bodies (EGBs) that were not detected by WSI review. Retrospective review of the WSI images showed that this histologic feature appeared differently in the WSI image when compared to the glass slide (Fig. 1). Minor differences in the diagnoses rendered were seen in 25 parts from 15 cases and are categorized in Table 3. Minor differences occurred primarily in small biopsies (14 cases, 24 parts) and in many instances represented differences in the evaluation of inflammation (10 cases, 15 parts).
Surgical pathology diagnostic differences and concordance

Surgical pathology differences by WSI review
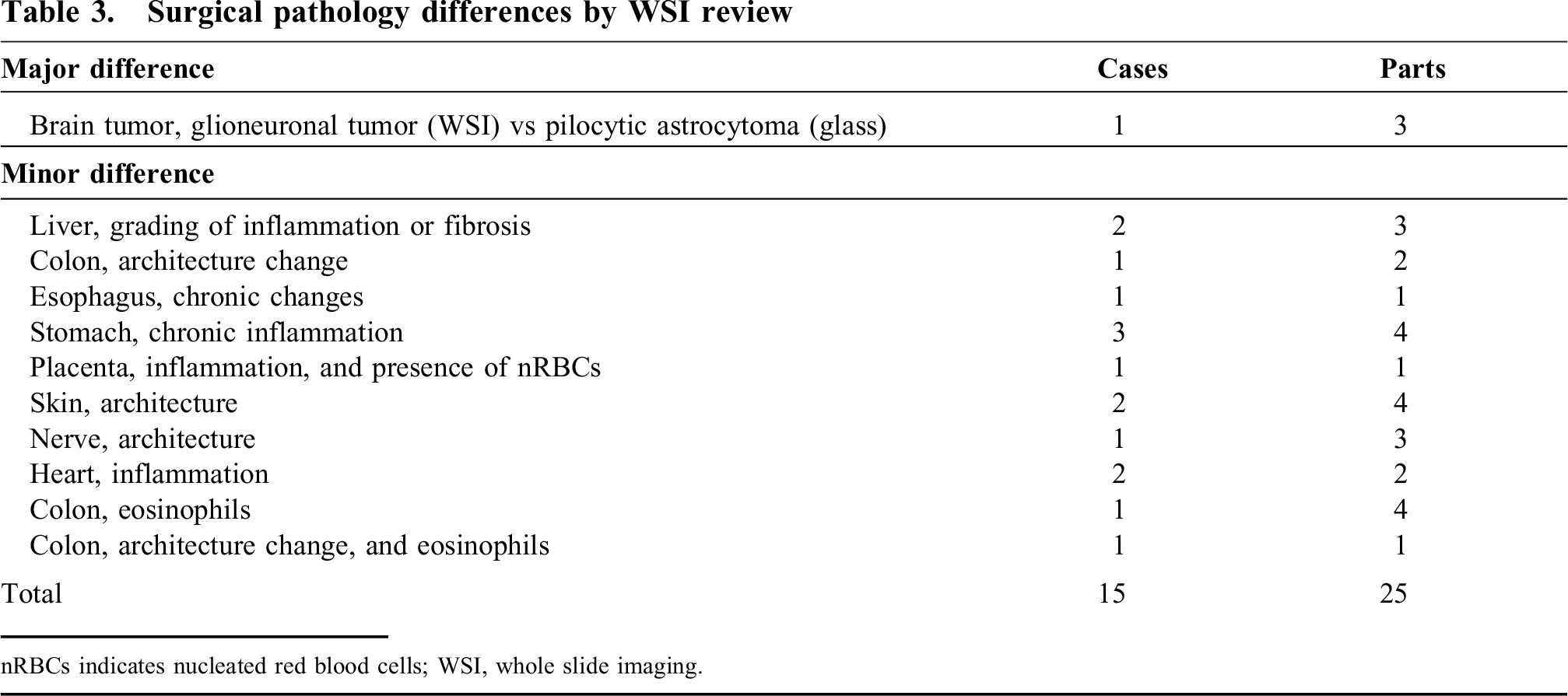
nRBCs indicates nucleated red blood cells; WSI, whole slide imaging.
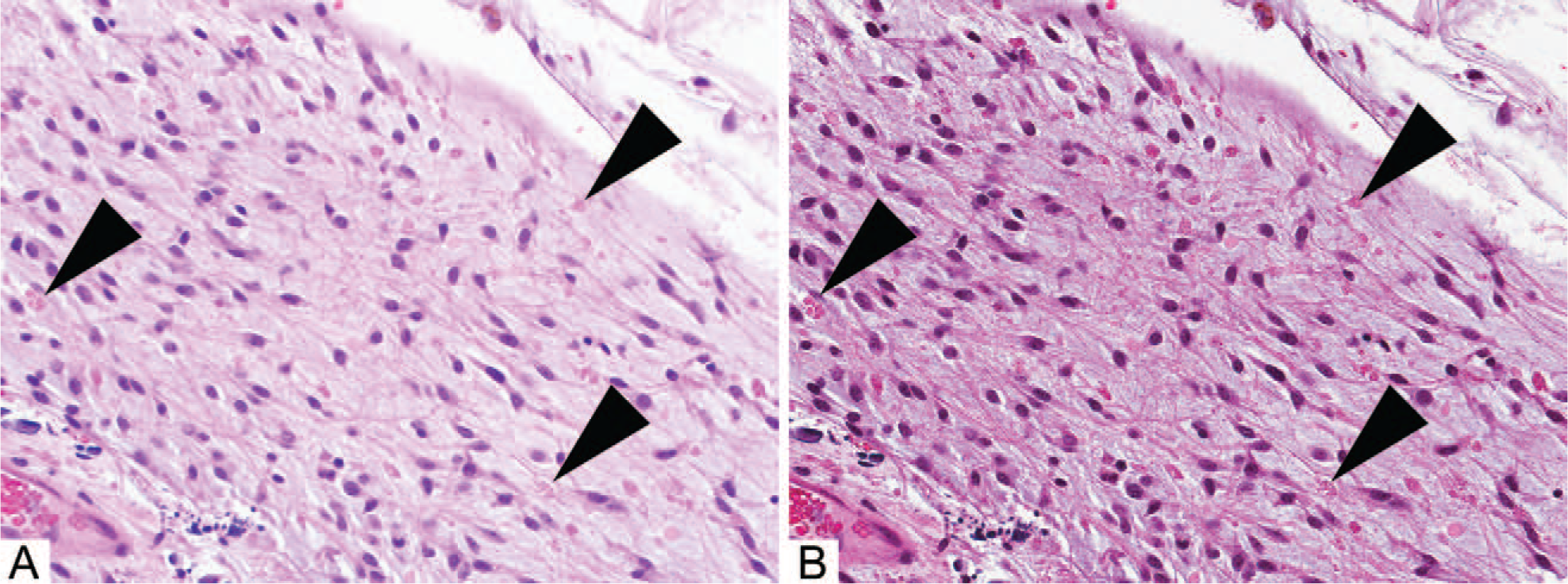
Differing glass slide and whole slide imaging (WSI) appearances of eosinophilic granular bodies. Eosinophilic granular bodies in this pilocytic astrocytoma (arrowheads) demonstrate a refractile quality when viewed by conventional microscopy (
Despite reaching a concordant diagnosis in nearly all surgical pathology cases, the identification of several features varied when reviewing WSI compared with glass slides. In addition to eosinophilic granular bodies (Fig. 1), identification of eosinophils and nucleated red blood cells varied between glass slide and WSI reviews (Fig. 2). These features each demonstrate refractile eosinophilic cytoplasm, with subtle differences in their appearance on glass slides compared with WSI.
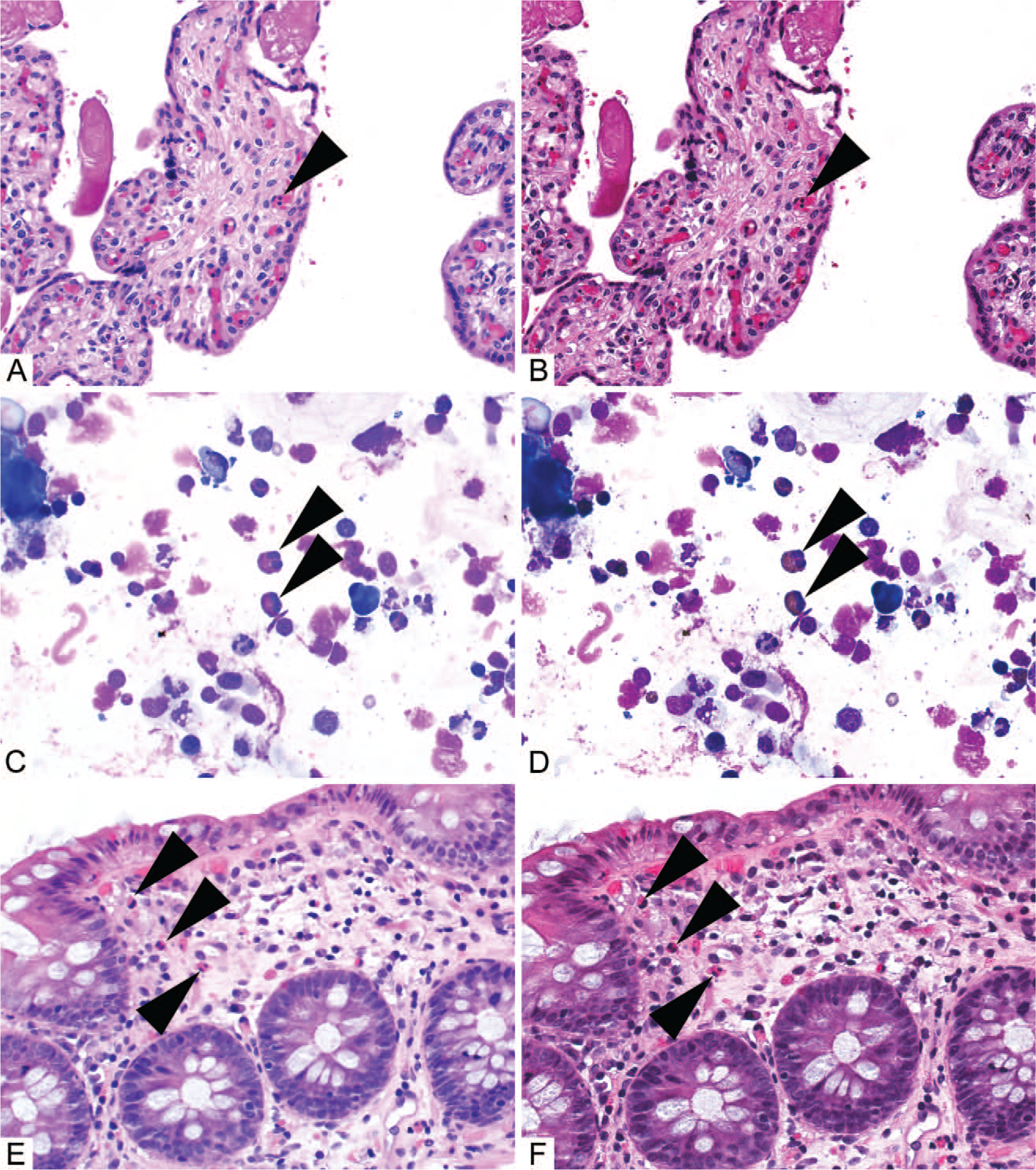
Differing glass slide and whole slide imaging (WSI) appearances of nucleated red blood cells and eosinophils. Nucleated red blood cells were challenging to identify in WSI with ×20 objective magnification image capture. Additionally, the refractile quality of the cytoplasm of nucleated red blood cells (arrowheads) appears differently in glass slides (
Low cellularity can limit digital capture of cytology specimens
Digital slide capture was unsuccessful for 2 of the 154 attempted cytology slides (1.3% of cytopathology slides). Low cellularity of the 2 unsuccessful cytology slides prevented focus calibration for image capture. The instrument normally defines focus points using an automated algorithm; at least 3 focus points must be identified before scanning will proceed. In the 2 unsuccessful slides, insufficient focus points could be created, and attempts to capture these slides using manually created focus points on identifiable cells were also unsuccessful. One slide represented a paucicellular smear from a thyroid fine-needle aspiration; the remaining 9 slides from this case were successfully captured and evaluated by WSI review. The second slide that could not be captured represented a paucicellular cytospin of cerebrospinal fluid and was the only slide available for this case, precluding evaluation and resulting in discordant scoring in our evaluation.
Unsuccessful WSI review of pediatric cytopathology
WSI evaluation of cytopathology cases was challenging, in part owing to technical limitations resulting from the image capture parameters we employed in our attempted validation. In our attempt to reach a 60-case validation set for cytopathology, we identified significant challenges in the first 21 cytopathology cases that we attempted to capture and review by WSI. Image capture of 1 case was unsuccessful, as described earlier. Of the 20 remaining cases that were reviewed by WSI, an additional 4 cases (representing 3 cerebrospinal fluid specimens and 1 pericardial fluid specimen) were unsatisfactory for review because of unacceptable image focus and/or resolution (Table 4). In these cases, the 3-dimensional nature of the material contributed to variable image quality in the single-plane image captured. Additionally, of the 16 cases in which a diagnosis was rendered, a diagnostic discordance that would alter patient care was seen in 2 cases (Table 5). Fungal elements were not identified in one bronchoalveolar lavage specimen (Fig. 3), and lymphoblasts were not identified in a bone marrow aspirate with core biopsy. In total, 7 of the 21 cases attempted (33.3%) were either unsatisfactory for evaluation or showed major diagnostic discrepancies. Minor diagnostic discrepancies were seen in 3 cases: rare bacteria were not identified on WSI review of 2 bronchoalveolar lavage specimens, and a differential cell count could not be confidently completed by WSI review of 1 bone marrow aspirate with core biopsy. Based on the number of major discrepancies in the first 21 cases we attempted, a minimum of 11.7% of cytopathology cases would be discordant once the goal of 60 cases was reached; thus, additional cases were not examined by WSI.
Cytopathology diagnostic differences and concordance

Cytopathology differences by WSI review
CSF indicates cerebrospinal fluid; WSI, whole slide imaging.
Single-plane image capture of cytopathology specimens results in variable focus quality. The fungal elements of this Gomori methenamine silver-stained cytospin can appear similar in glass slides (
DISCUSSION
The CAP-PLQC–recommended guideline statements offer parameters for WSI validation, including a minimum case number for a validation study and a minimum “washout” time between glass slide and WSI review. Notably, the guidelines do not include minimum technical specifications for WSI systems and image capture; instead, they allow laboratories to make individualized decisions about WSI platforms, including hardware, captured image resolution, and image management. We therefore attempted to implement these guidelines with our existing systems, including standard computer monitors, thereby avoiding significant capital investment. This allowed us to simultaneously define the limitations of our current WSI systems, including capture parameters in potential clinical applications, and to prospectively evaluate the recommendations made within the guidelines. We designed validation studies for pediatric surgical pathology and pediatric cytopathology according to the guidelines. The CAP-PLQC guidelines allow individual laboratories to determine specific standards for acceptable concordance. The guideline statements describe concordance as “an agreement in the diagnosis made” without mention of the clinical implications of any differences in diagnoses. We therefore elected to evaluate our results using stringent criteria; any diagnosis in a differing category was considered a major difference and therefore discordant, irrespective of the impact on patient management under current standards. This scoring method differs from previous definitions of concordance that focus on evaluating differences in the context of patient management [31]. Further, we required successful image capture with satisfactory resolution for review for a case to be considered concordant. Although either method would have produced similar results in our study, we elected to employ criteria focused strictly on the diagnosis rendered, as we considered this to be an appropriate and highly stringent measurement of our WSI validation study. Previous studies demonstrated that WSI review and re-evaluation of glass slides results in concordance of approximately 98% [31]. We therefore anticipated that an acceptable concordance for a 60-case validation study would involve, at most, 2 discordant cases (96.7% concordance).
We report here successful implementation of the recommended guidelines for pediatric surgical pathology specimens, with greater than 98% diagnostic concordance. Of note, the 1 discordant case, a brain tumor, would not have resulted in a change in patient management under current treatment protocols. However, this dissimilarity resulted in a differing World Health Organization diagnostic category. The differing diagnosis in this case was related to the detection of EGBs (Fig. 1), highlighting an important feature for pathologists to recognize when evaluating WSI. Similarly, many of the differences we classified as minor in our surgical pathology validation are features with refractile eosinophilic cytoplasm (Table 3). Disparities in the detection of these features may relate to differences in the color of these structures in WSI and in the refractile texture of these structures. Color calibration was not utilized in this study and could assist in detecting these structures by making their appearance in WSI more similar to their appearance in glass slides [32]. However, we believe that the refractile qualities of these structures are more likely to play a role in differing detection; this refractile quality cannot be adequately represented in a single-plane image. Eosinophil granules and inflammatory cells are difficult features to identify in WSI review [1,16,28,33], and our data are the first to identify EGBs and nucleated red blood cells as challenging features to identify. Of note, specimens including these features were imaged at ×20/magnification (0.5 μm/pixel), and detection of these features may improve with higher image resolution. Overall, our attempt to execute the CAP-PLQC guidelines for pediatric surgical pathology specimens showed high concordance, demonstrating that evaluation of 60 specimens was sufficient for a broad range of pediatric specimens to identify key features that pathologists should be aware of when evaluating clinical cases using WSI.
Our study of cytopathology specimens identified several challenges in capturing and evaluating cytopathology specimens using the single-plane image-capture parameters we attempted. Cytopathology specimens often result in the distribution of tissue over a greater depth than the 4- to 5-μm thickness of standard surgical pathology sections. Further, cytopathology specimens are often composed of cells dispersed across the slide in varied focal planes. These aspects of cytopathology specimens made automated focus calibration challenging. This problem was compounded in paucicellular specimens, in which wider spacing of cells across the imaged area hindered automated detection of the tissue. In addition to a failed capture, which prevented evaluation of 1 case, our image capture in a single plane resulted in inadequate detail for review of 4 cases. Using a single image-capture plane selected by automated focus calibration resulted in areas of the images with suboptimal focus, similar to those shown in Figure 3. These technical challenges contributed to difficulties in the detection of microorganisms, eosinophils, and lymphoblasts, similar to previous studies of the implementation of WSI review [1,16,28,33]. To mitigate these challenges, WSI review of cytopathology specimens will most likely require capture of multiple-plane images to avoid the challenges we encountered with single-plane images. Overall, the rate of discordant cytopathology specimens in the 21 cases we attempted was sufficient to demonstrate that the method we attempted would be unsuccessful.
Our successful implementation of the CAP-PLQC guidelines for WSI validation demonstrates the feasibility of these guidelines for WSI validation studies. A review of 60 cases of pediatric surgical pathology specimens allowed us to include a range of specimen types, demonstrating high diagnostic concordance and identifying unique features of pediatric specimens with differing appearances in glass slides and WSI. Similarly, the attempt to analyze 21 cytopathology cases easily highlighted any technical challenges that would prohibit diagnostic review within the parameters we selected. Our experience suggests that the recommendations of the CAP-PLQC guidelines, including the numbers of cases selected for review, are adequate to confirm the accuracy of WSI review and to identify diagnostic challenges. Our study indicates that access to pediatric surgical pathology expertise can be further extended by WSI. Features of pediatric specimens that were challenging to evaluate by WSI were generally those with refractile eosinophilic cytoplasm, in agreement with previous studies. Unique to pediatric specimens, we identified EGBs and nucleated red blood cells as challenges to WSI review. This study of exclusively pediatric specimens, the first such study to our knowledge, confirms the feasibility of WSI review and demonstrates key features of which pathologists should be aware when reviewing these specimens by WSI.
Footnotes
ACKNOWLEDGMENT
We thank the Biopathology Imaging Core at Nationwide Children's Hospital, especially Shital Hobensack, for preparation of whole slide images.