
Abstract
Metachromatic leukodystrophy (MLD) is an autosomal recessive lysosomal storage disease caused by deficient activity of arylsulfatase A, leading to an accumulation of sulfatide in myelinating cells and progressive central and peripheral demyelination. Sulfatide also accumulates in various organs, most notably the gallbladder. Gallbladder mucosal hyperplasia with papillomatosis, in the setting of abdominal pain and hemobilia, is often demonstrated by sonography. We present a histologic and ultrastructural description of these alterations in a 5-year-old girl with MLD who presented with abdominal pain and feeding intolerance. Gross and light microscopic analysis demonstrated diffuse villous hyperplasia of the gallbladder mucosa with intraepithelial and intravillous macrophage accumulations of metachromatic material. Electron microscopic analysis demonstrated this material to comprise numerous membrane-bound inclusions composed of concentrically lamellated, dense material. The rarity of descriptions of this finding prompted this case report.
INTRODUCTION
Metachromatic leukodystrophy (MLD, OMIM number, 250100) is an autosomal recessive lysosomal storage disease caused by deficient activity of arylsulfatase A (ARSA). This enzyme catalyzes the first step in the degradation pathway of the sphingolipid galactosylceramide-3-O-sulfate (sulfatide), normally abundant in myelin and myelinating cells. This leads to massive accumulation of sulfatide in Oligodendroglia and Schwann cells (visualized as cytoplasmic metachromatic pigment), which results in progressive demyelination in the central and peripheral nervous systems [1,2]. Although variable clinically, the most common phenotype is the late-infantile form. Previously normally developing toddlers present with progressive hypotonia and decreased deep tendon reflexes, followed by spasticity and cognitive decline, and later, optic atrophy, seizures, and death [1–3]. Diagnosis requires demonstration of deficient arylsulfatase A activity in peripheral blood leukocytes or cultured fibroblasts and quantification of urine sulfatide. Confirmation is accomplished by sequencing the ARSA gene. Treatment is mainly palliative, although hematopoietic stem cell transplantation, if performed very early, may improve central symptoms in patients with later onset or milder forms of MLD [1–3].
Outside of the nervous system, sulfatide also accumulates in the kidneys, pancreas, liver, lymph nodes, spleen, adrenal glands, and ovaries in patients with MLD. For the most part, such accumulations are not associated with obvious morphologic changes or clinical manifestations [4]. However, gallbladder mucosal hyperplasia with papillomatosis, usually in the setting of abdominal pain and hemobilia is often demonstrated by sonography, occasionally before onset of neurologic symptoms or an MLD diagnosis [5–7]. In a few cases [8,9], life-threatening hematobilia has been reported. Although there are only a few published reports, histopathologic findings in the gallbladder in patients with MLD generally corroborate sonography observations. These findings include diffuse hyperplasia of the gallbladder mucosa typified by a proliferation of thin, delicate, papillary projections; single or multiple, large, polypoid lesions, often occluding the lumen; and large accumulations of macrophages bearing metachromatic material [4,8–16]. Occasionally, findings include significant accumulation of extracellular mucin in Rokitansky-Aschoff sinuses [9,13]. We present a histochemical and electron microscopic analysis of the gallbladder alterations in a 5 year-old girl with MLD.
CASE REPORT
A 4-year-old girl presented with a progressive gait disturbance, cognitive impairment, aggression, and drooling. On exam, she was noted to have hyperreflexia and increased tone in her lower extremities. Magnetic resonance imaging showed a “tigroid” pattern of demyelination in the deep cerebral hemispheric white matter, with extensive involvement of the corpus callosum and partial involvement of the posterior capsules and cerebral peduncles. A diagnosis of MLD was confirmed by significantly reduced ARSA enzyme activity in blood leukocytes and urinary sulfatide excretion. The patient underwent reduced-intensity, allogeneic umbilical cord blood transplant. Her posttransplant course was complicated by episodes of adenoviral infection and giardiasis.
Approximately 90 days posttransplant, she presented with abdominal pain and inability to tolerate enteral feedings. Hepatobiliary iminodiacetic acid scans showed nonfilling of the gallbladder. Ultrasound showed thickening of the gallbladder wall to approximately 3 mm. No pericholecystic fluid, stones, or polypoid lesions were identified. The patient underwent laparoscopic cholecystectomy. At surgery, the gallbladder was very small and indurated and appeared thickened and inflamed. The cystic duct was also thickened (6 mm) and appeared inflamed. There were several adhesions between the gallbladder and infundibulum and the adjacent duodenum and omentum.
On gross examination, the gallbladder measured 4.9 × 1.8 × 1.1 cm. The outer surface appeared smooth, except for focal, cauterized, fibrous adhesions. No cystic duct was grossly identified. The gallbladder wall measured up to 4 mm thick, and the mucosal surface was diffusely carpeted by villous, papillary projections, which extended into the infundibulum. No gallstones, polypoid masses, or other lesions were grossly identified. On light microscopy, the gallbladder mucosa exhibited marked villous hyperplasia (Fig. 1A). The tips of the projections were frequently expanded by large collections of macrophages; of which, many cells contained metachromatic material (Fig. 1B). The pigment-laden macrophages were stained with Alcian blue (not shown) and colloidal iron (Fig. 1B inset). Colloidal iron–positive material was also observed in epithelial cells (Fig. 1B inset). Scattered, perivascular lymphocytic infiltrates and Rokitansky-Aschoff sinuses were observed in the wall; however, sinuses were not involved by extracellular mucin.
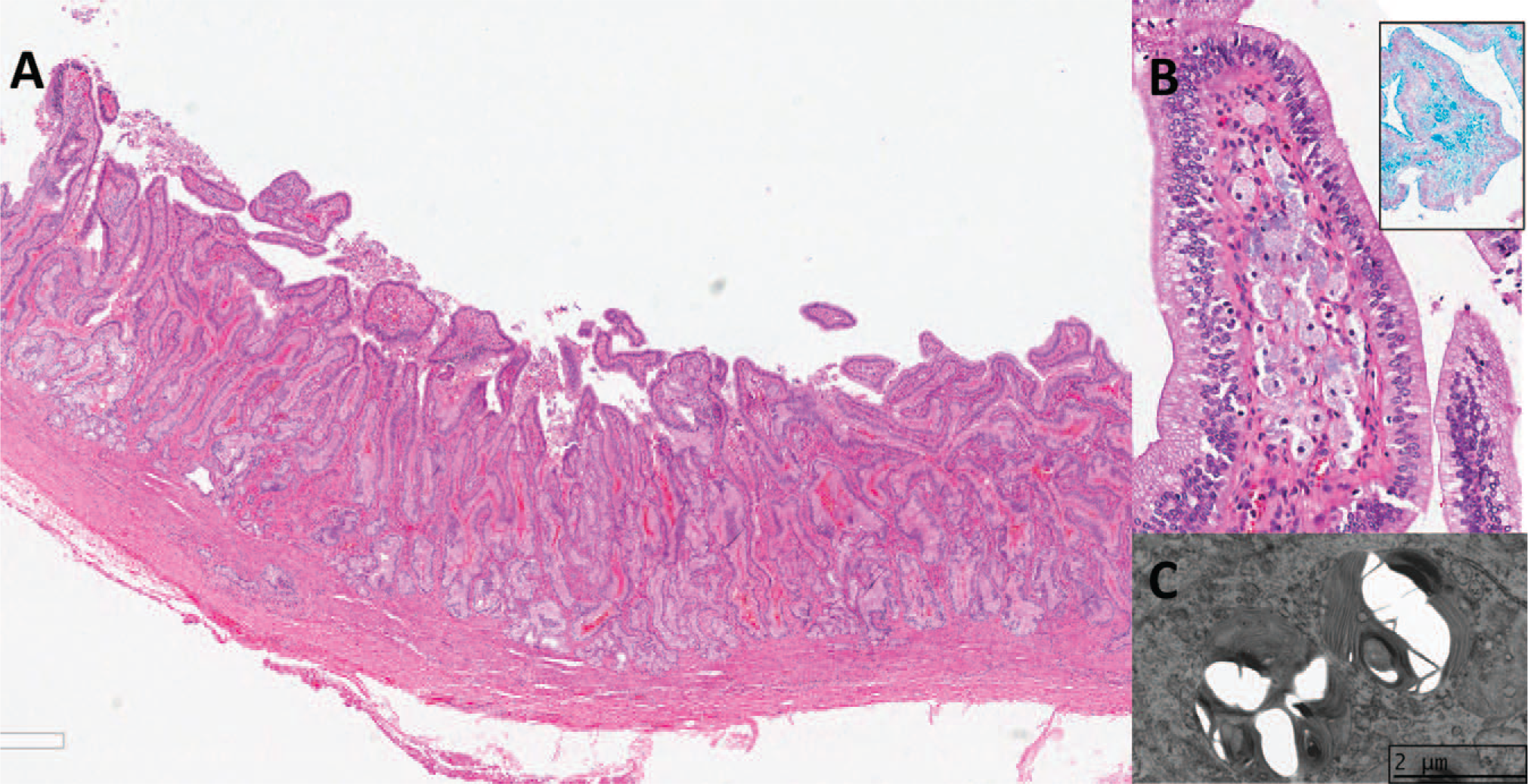
Electron microscopy was performed retrospectively on formalin-fixed tissue. Despite obvious processing artifact, the mucosal epithelial cells demonstrated cytoplasmic expansion associated with supranuclear accumulation of numerous membrane-bound inclusions. The content of these inclusions varied from homogeneously amorphous material to dense, concentrically lamellated bodies resembling the intralysosomal material seen in Oligodendroglia and Schwann cells in MLD (Fig. 1C).
DISCUSSION
We present a histologic and ultrastructural description of gallbladder mucosal alterations in a 5-year-old girl with MLD. Findings included diffuse villous hyperplasia, metachromatic pigment-laden macrophages, and intraepithelial accumulation of metachromatic material. Frank polyposis, as described in a few reports [eg, 5,6], was not observed; however, the sheer volume of villous papillary projections in the infundibulum could be related to the obstructive features of increased wall thickness and Rokitansky-Aschoff sinuses. The lack of larger lesions in this case may have been due to the patient's hematopoietic stem cell transplantation 3 months prior. Transplant serves to replace patient macrophage and microglial populations with cells expressing a functional hydrolase, with the goal of restoring scavenger function. In the brain and peripheral nervous system, this turnover is known to be slow relative to disease progression. In other organs, however, replacement occurs at a faster rate [17]. This is the likely explanation for the paucity of metachromatic macrophages seen in the gallbladder of this patient, relative to numbers seen in nontransplanted patients.
It is not known how sulfatide accumulation causes morphologic alterations in the gallbladder or related symptoms in patients with MDL. In the nervous system, progressive lysosomal storage of sulfatides is thought to ultimately kill oligodendrocytes and Schwann cells, and presumably, the sulfatide released by the dying cells is subsequently phagocytosed by macrophages. As no appreciable epithelial damage was observed in this case, it is doubtful that sulfatide accumulation is due to similar mechanisms in the gallbladder. It has been postulated [15] that increased sulfatide in the bile may be related to epithelial hyperplasia. Conversely, it is possible that intracellular accumulation triggers this often florid response instead.
Abdominal symptomatology, whether from luminal obstruction or stretching of the gallbladder wall, often precedes clinically appreciable demyelination by months or even years. In these cases, identifying the characteristic histologic changes in the gallbladder may permit earlier diagnosis, ie, when hematopoietic stem cell transplantation may be of greater efficacy. Although an uncommon but well-reported association, the pediatric pathologist needs to be alert to this finding both at the gross bench, where mucosal hyperplasia with thickening of the wall may be apparent as well as histologically as an incidental one, and not mistake the changes of MLD for papillary cholesterolosis.