
Abstract
Coronary artery aneurysms (CAA) remain an important complication of Kawasaki disease (KD), the most common form of pediatric acquired heart disease in developed countries. Potentially life-threatening CAA develop in 25% of untreated children and 5% of children treated with highdose intravenous immunoglobulin during the acute phase of the self-limited vasculitis. Noncoronary artery aneurysms (NCAA) in extraparenchymal, muscular arteries occur in a minority of patients with KD who also have CAA, yet little is understood about their formation and remodeling. We postulated that activation of the transforming growth factor-β (TGF-β) pathway in KD may influence formation and remodeling of aneurysms in iliac, femoral, and axillary arteries, the most common sites for NCAA. We studied a resected axillary artery from one adult and endarterectomy tissue from the femoral artery from a second adult, both with a history of CAA and NCAA following KD in infancy. Histology of the axillary artery aneurysm revealed destruction of the internal elastic lamina and recanalization of organized thrombus, while the endarterectomy specimen showed dense calcification and luminal myofibroblastic proliferation. Immunohistochemistry for molecules in the TGF-β signaling pathway revealed increased expression of TGF-β2, TGF-β receptor 2, and phosphorylated SMAD3. These findings suggest ongoing tissue remodeling of the aneurysms decades after the acute injury and demonstrate the importance of the TGF-β signaling pathway in this process.
INTRODUCTION
Although the epicardial coronary arteries are the most common site of aneurysm formation in patients with Kawasaki disease (KD), a subset of KD patients may also develop aneurysms in noncoronary arteries [1,2]. Autopsy studies from Japan have suggested that certain noncoronary artery locations are more susceptible to aneurysm formation in KD, particularly the iliac and axillary arteries [3,4]. Autopsy studies of coronary artery aneurysms (CAA) reveal characteristic changes, including luminal myofibroblastic proliferation (LMP), thrombosis, recanalization with neovascularization, and dense calcification [3,4]. The mechanism of aneurysm formation remains unclear, but influence of the transforming growth factor (TGF)–β pathway has been proposed [5].
We report on two subjects who developed KD associated with coronary, axillary, and femoral artery aneurysms at ages 1 to 2 months. We performed histological studies on the axillary aneurysm and femoral artery endarterectomy tissue resected from these patients 21 and 30 years after onset of KD, respectively. Based on our studies of the role of the TGF-β signaling pathway in CAA remodeling, we postulated that this signaling pathway also might influence remodeling of aneurysms in the femoral and axillary arteries in KD.
MATERIALS AND METHODS
Subjects and tissue samples
Cases 1 and 2 were, respectively, a 31-year-old male and a 22-year-old female diagnosed with acute KD at 1 to 2 months of age who developed coronary, femoral, and axillary artery aneurysms. Both patients were enrolled as subjects in the San Diego Adult KD Collaborative study, and completed general and cardiovascular health questionnaires. Surgically resected tissues included an endarterectomy specimen from the femoral artery of Case 1 and a completely resected axillary artery aneurysm from Case 2. This study was approved by the Institutional Review Board at the University of California, San Diego (UCSD) and written consent was obtained for the use of all tissues.
Histological examination
Surgical specimens were formalin-fixed and paraffin embedded following surgical resection. Histochemical staining of 5 μM sections with hematoxylin-eosin (H&E), Verhoeff-van Gieson, and Masson's trichrome stains was performed using standard techniques.
Immunohistochemical staining
Tissue sections were baked at 65°C for 60 minutes before deparaffinization and rehydration using standard techniques. Endogenous peroxidase activity was quenched using Peroxidase Block (LSAB+System-HRP; Dako Laboratories, Carpinteria, CA, USA) for 10 minutes. Antigen retrieval was performed in sodium citrate buffer (10 mM sodium citrate, 0.05% Tween 20, pH 6.0) in a microwave oven for 10 minutes. Slides were incubated in blocking solution consisting of 5% normal swine serum (Jackson ImmunoResearch Swine Serum; Jackson ImmunoResearch Laboratories, Inc., West Grove, PA, USA) in 0.01M Tris-HCl with 1% bovine serum albumin (BSA) for 60 minutes at room temperature. Slides then were incubated overnight at 4°C with the following primary antibodies diluted in 0.01M Tris-HCl with 1% BSA: anti-TGF-β2 (sc-90, 1:100 dilution; Santa Cruz Biotechnologies, Inc., Dallas, TX, USA), anti-TGFβR2 (ab-78419, 1:100 dilution; Abcam, Cambridge, UK), anti-pSMAD3 (ab-52903, 1:250 dilution; Abcam), anti-Von Willebrand Factor (VWF; ab-9378, 1:500; Abcam). Antibodies were detected using a biotinstreptavidin immunoperoxidase method (LSAB+System-HRP, Dako) followed by visualization with the AEC substrate kit (Vector Labs, Burlingame, CA, USA) according to manufacturer's instructions. Normal rabbit immunoglobulin G (1:10 000 dilution; Jackson ImmunoResearch Laboratories, Inc.) was used as a negative staining control in each run. A normal axillary artery from the autopsy of a 31-year-old female with history of renal transplantation who died from septic shock was used as a negative tissue control. Nuclear staining was performed using 1:2 diluted hematoxylin. Microscopic images were captured by NanoZoomer 2.0-HT using NanoZoomer Digital Pathology (NDP) v2.1 (Hamamatsu Photonics, Hamamatsu, Japan).
Review of published KD peripheral aneurysms cases
To better understand the frequency and presentation of peripheral artery aneurysms in KD, a comprehensive review of the English language literature was performed using PubMed with search keywords “Kawasaki Disease,” “femoral,” “iliac,” “axillary,” “aneurysm,” and “pathology.” Coronary artery status, age of onset, sex, and ethnicity were recorded for all cases.
RESULTS
Case reports
Case 1 clinical course
Case 1 was a 31-year-old white male who first developed acute KD at age 7 weeks, though the diagnosis was initially missed. Echocardiography confirmed large CAA in the right (RCA) and left anterior descending (LAD) coronary arteries, as well as the left main coronary artery (LMCA). The patient also was noted to have bilateral axillary aneurysms. He was treated with dipyridamole and aspirin as this was before the advent of intravenous immunoglobulin (IVIG) therapy. At age 22, he developed right lower extremity claudication. No obvious aneurysms were found by magnetic resonance angiography of the iliac or femoral arteries, though a 2-cm irregularity in the proximal right superficial femoral artery (SFA) was noted. Lower extremity claudication recurred at age 25 and a lower extremity angiogram showed 50% to 60% stenosis in the proximal right SFA and tandem 50% stenoses in the left SFA and popliteal artery. No intervention was undertaken and at age 30 years, the patient sought participation in the San Diego Adult KD Collaborative Study at University of California, San Diego (UCSD). A medical history revealed no risk factors for atherosclerotic disease. Physical examination revealed a body mass index (BMI) of 26.0 kg/m2 (overweight = 25–29.9), blood pressure 124/80 mm Hg, and heart rate 75 beats/min. Cardiac examination was unremarkable. Posterior tibial and dorsalis pedis pulses were not palpable, and a bruit was heard over both femoral arteries. A lipid profile revealed the following values: total cholesterol 220 mg/dl, triglycerides 128 mg/dl, HDL-cholesterol 75 mg/dl, and LDL-cholesterol 119 mg/dl. A transthoracic echocardiogram revealed normal left ventricular size, wall thickness, and systolic function. The CT calcium score was 513 mm3. An abdominal aortogram showed no evidence of atherosclerosis. Both femoral arteries were severely diseased with a 99% ostial right superior femoral artery (SFA) stenosis (Fig. 1). The proximal right SFA had a 70% narrowing with a discrete 95% mid-right SFA stenosis. The left SFA had an 80% to 90% stenosis. The popliteal and tibial peroneal vessels were widely patent bilaterally. Ventricular angiography demonstrated anterior hypokinesis with an estimated left ventricular ejection fraction of 50%. Coronary angiography revealed a patent, smooth LMCA. The LAD was proximally occluded just distal to the origin. The circumflex artery was a moderate-sized vessel with a 4-mm discrete proximal aneurysm. There were left-to-left collaterals supplying the large first diagonal branch. The RCA was a large, dominant vessel with a 6-mm discrete aneurysm distally involving the posterior descending artery. There were right-to-left collaterals filling the LAD. The patient underwent a left femoral endarterectomy with pericardial patch angioplasty (Fig. 2A) and, in a second procedure, a right femoral artery endarterectomy with pericardial angioplasty with stent placement in the right SFA.
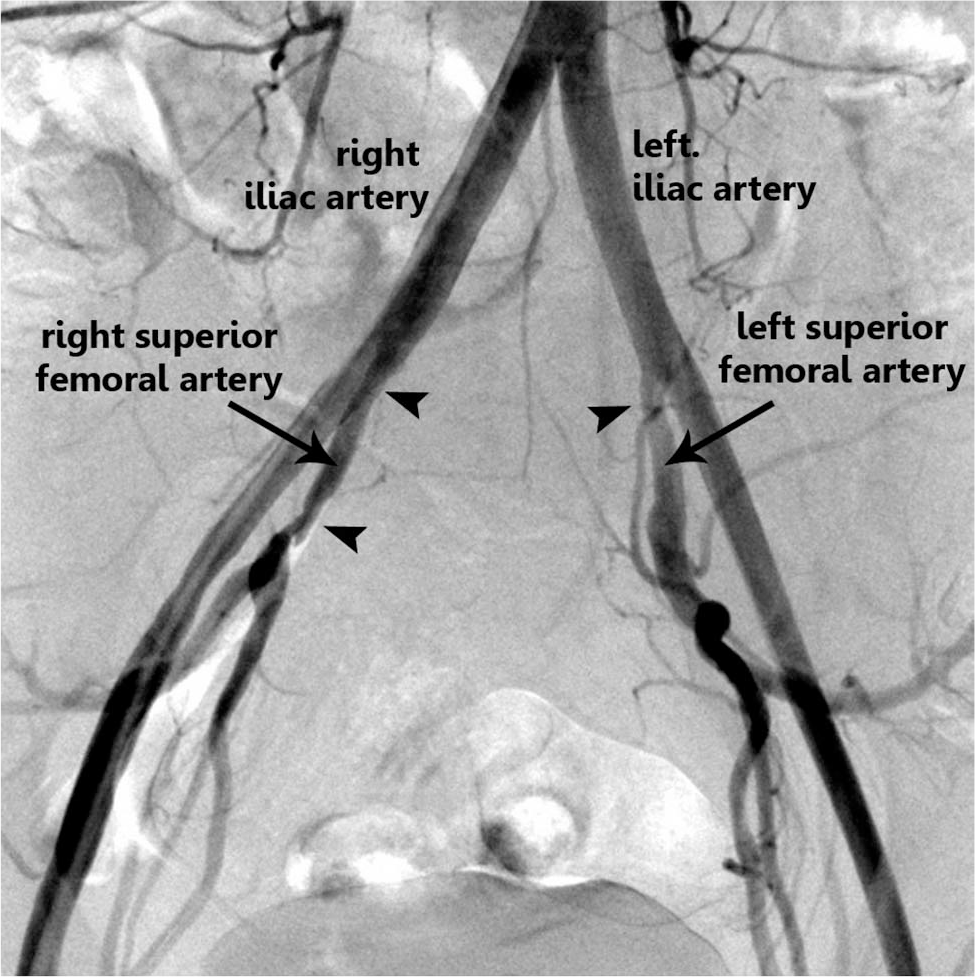
Angiography of the iliac arteries and branches in a 30-year-old man with a history of Kawasaki disease at age 7 weeks who presented with claudication. Severe stenoses were detected of the superior femoral arteries bilaterally (arrowheads).
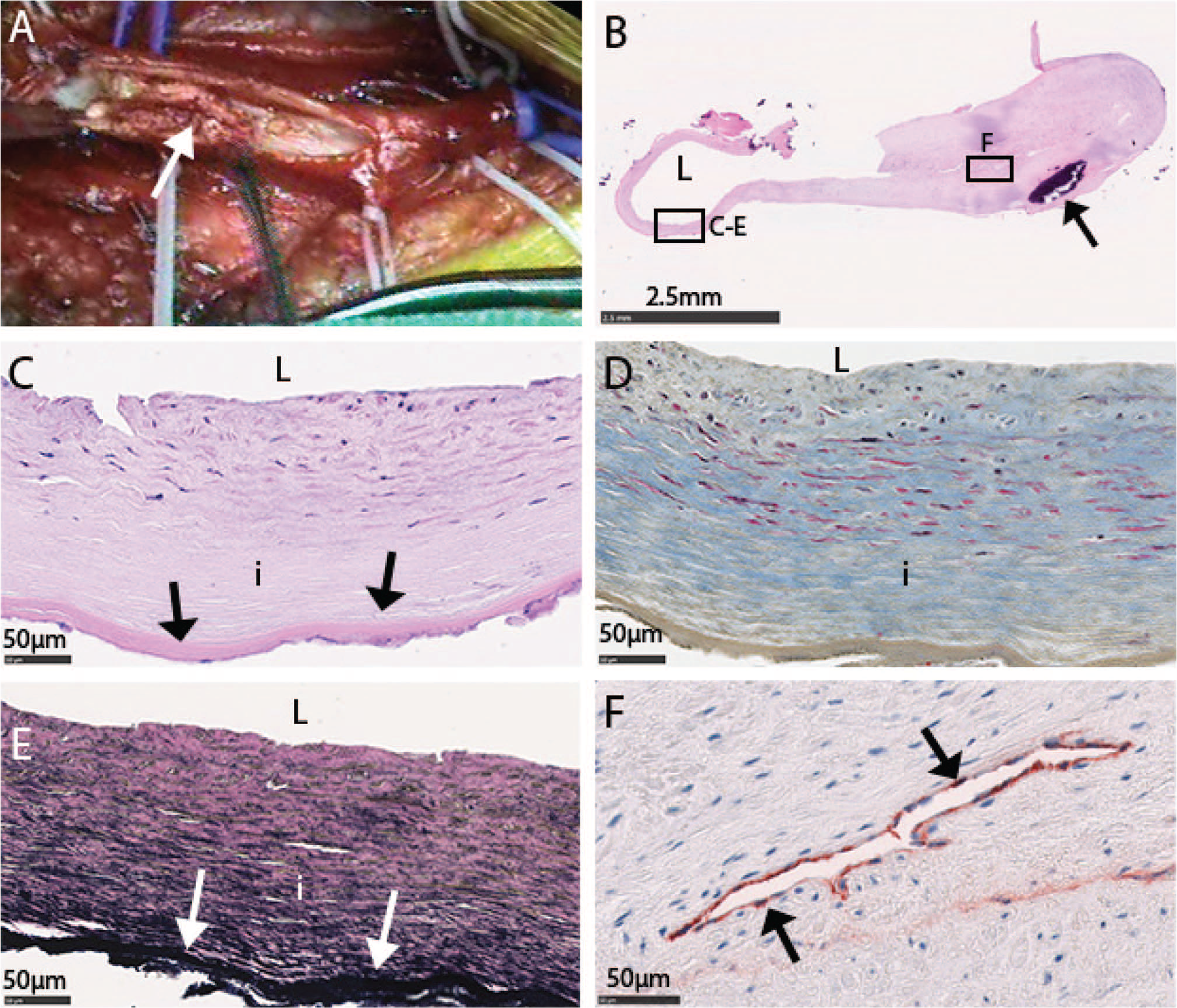
Endarterectomy specimen from left femoral artery. (
Case 1 histologic findings
Intimal tissue removed during left iliac endarterectomy was stained with H&E (Fig. 2B) revealing a thickened intima (Fig. 2C) with diffuse fibrosis (Fig. 2D) and an intact elastic lamina (Fig. 2E, arrows). Many spindle-shaped cells were noted along the luminal side of intima. The organized thrombus contained a large area of calcification (Fig. 2B, black arrow). Several areas of neovascularization in the thrombus were noted with VWF-positive endothelial cells lining the lumen (Fig. 2F, arrow).
The right femoral endarterectomy specimen contained an intimal layer with internal elastic laminae, calcification (Fig. 3A), and an area of possible neovascularization (Fig. 3B). Elastin stain (Fig. 3C) showed an internal elastic lamina (Fig. 3C, black arrows) adjacent to the intima, which was thickened and diffusely fibrotic (Fig. 3D). Atherosclerotic plaque was seen in in a thickened intima (Fig. 3E, arrowhead).
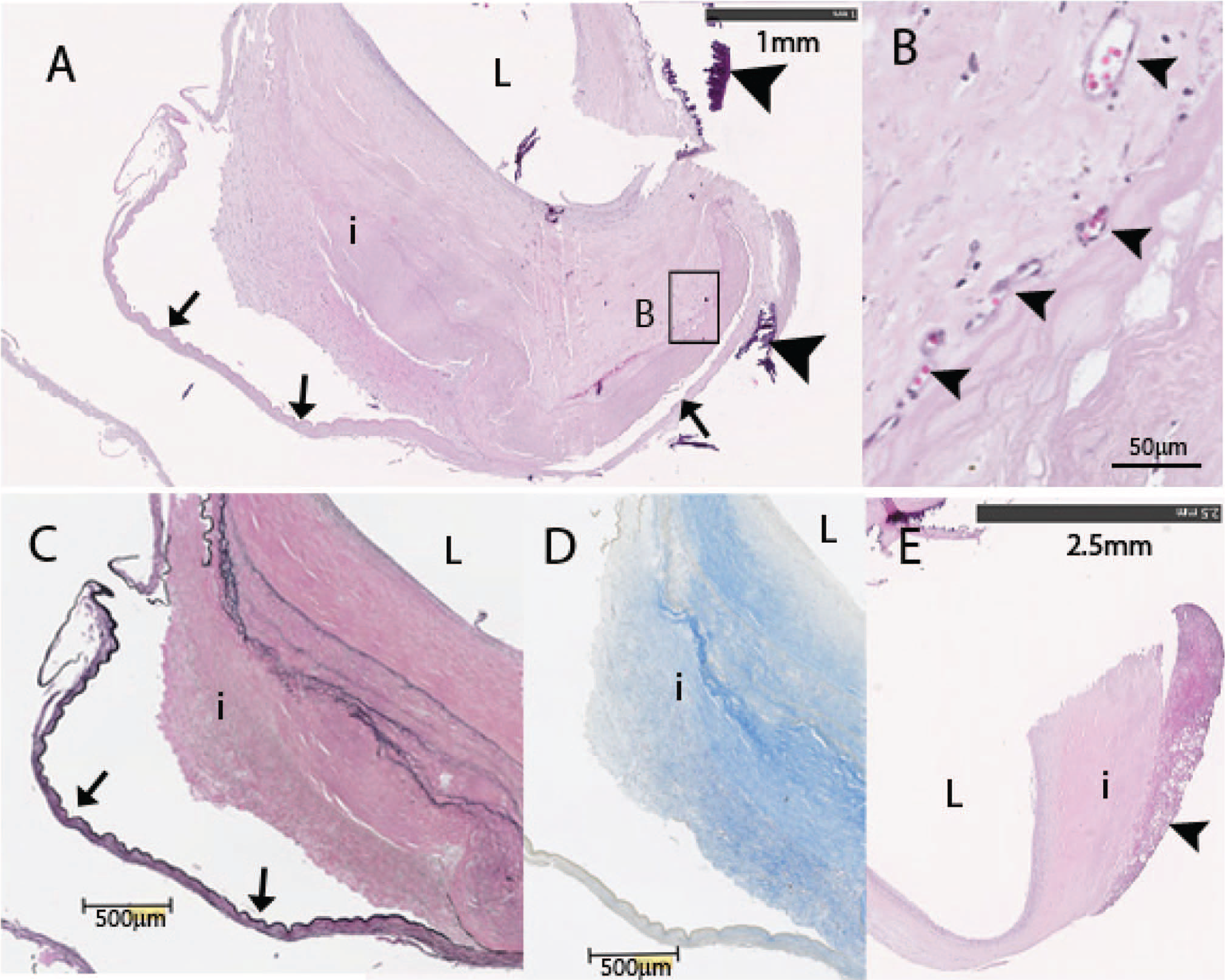
Endarterectomy specimen from right femoral artery. (
Case 2 clinical course
A 21-year-old white female suffered KD at age 1 month, but the diagnosis was initially missed. She was diagnosed retrospectively with KD at age 4 months when she was noted to have giant coronary aneurysms by echocardiography. She was treated with aspirin. At age 18 months, she had a second episode of KD, at which time she was noted also to have bilateral axillary aneurysms. The coronary artery aneurysms remodeled, though the bilateral axillary aneurysms persisted. At age 19, she underwent left axillary artery bypass surgery for symptoms of left arm claudication. At age 21, she enrolled in the San Diego Adult KD Collaborative study. Her chief complaint was chest pain and exercise intolerance. Coronary angiography with intravascular ultrasound demonstrated aneurysms of the LMCA and LAD with no stenosis. The CT calcium score was 100 mm3. There was an 80% to 90% stenosis of the right axillary artery before the aneurysm. The patient underwent surgical resection of the axillary artery aneurysm with a saphenous vein interposition.
Case 2 histologic findings
The resected axillary artery aneurysm showed diffuse changes in all layers of the arterial wall (Fig. 4). A classic “lotus root” conformation was noted with recanalization and neovascularization in multiple channels of the completely occluded artery (Fig. 4A). Large regions of calcification were seen (purple). Heavy deposits of collagen, suggestive of diffuse fibrosis (Fig. 4B), were evident through several layers of artery. However, there were no changes consistent with atherosclerosis. Endothelial-like cells were clearly seen along the lumen edge (Fig. 4C). The original elastic lamina was destroyed, though a new elastic lamina (Fig. 4D) was seen along the recanalized lumen.
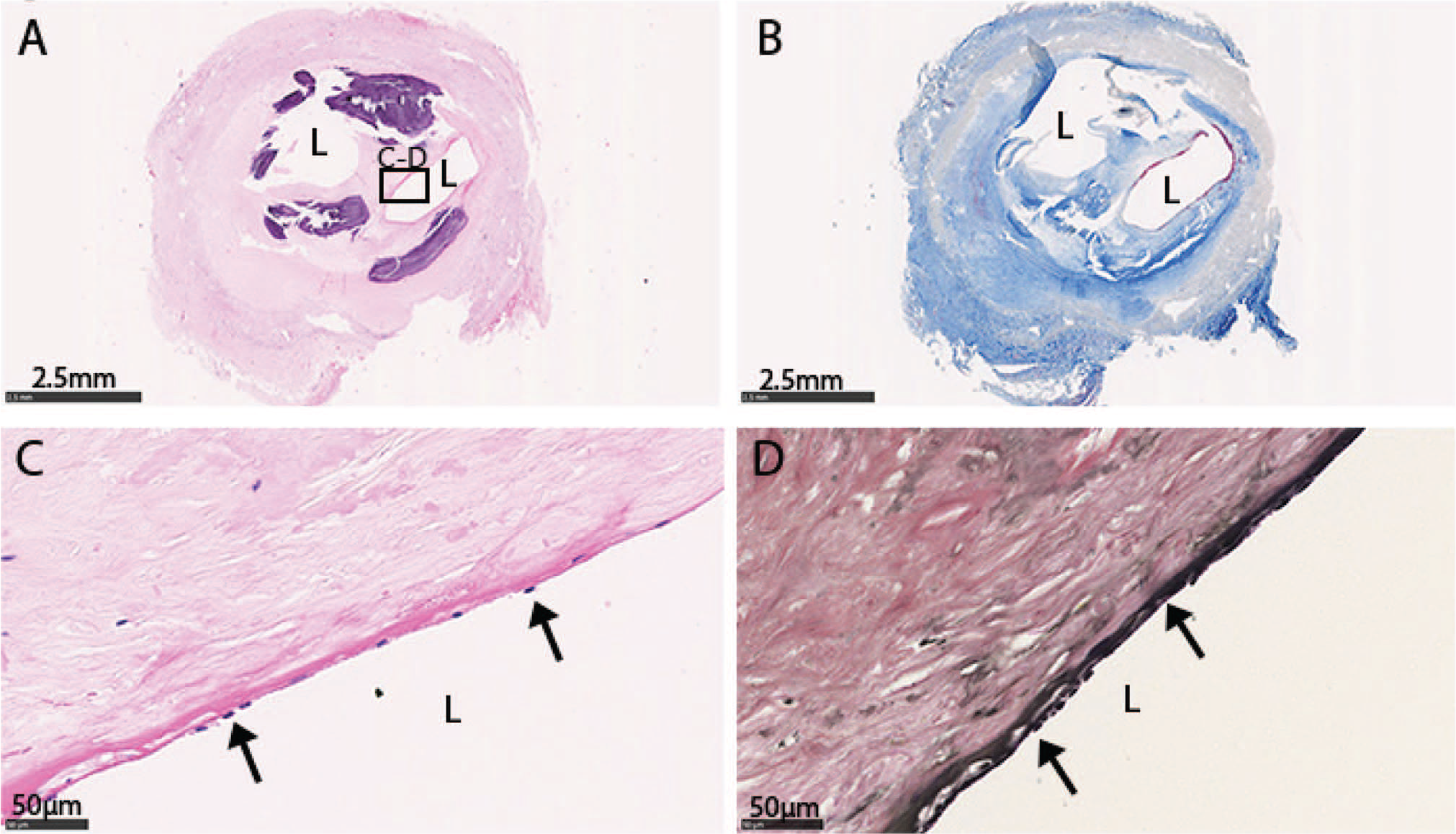
Surgically resected right axillary artery aneurysm. (
Immunohistochemical study of aneurysmal walls for TGFβ pathway molecules
Resected tissues and a normal control axillary artery were stained for the ligand TGF-β2, the receptor TGF-βR2, and the activated signaling molecule pSMAD3 (Fig. 5). Intracytoplasmic staining for TGF-β2 (Fig. 5A–C) was noted in all samples. Positive staining for the TGF-βR2 (Fig. 5E–G) localized to the cell membrane and was noted in spindle-shaped cells in the thickened intima of the tissue samples. Staining for nuclear-localized pSMAD3 (Fig. 5I–K) was detected in the left and right femoral endarterectomy specimen and right axillary artery aneurysm. Control staining with rabbit IgG on patient tissues was negative (Fig. 5M–O). Normal control tissues showed less extensive positive staining for TGF-β2 (Fig. 5D) and TGF-βR2 (Fig. 5H), and no staining for nuclear pSMAD3 and rabbit IgG (Fig. 5L,P).
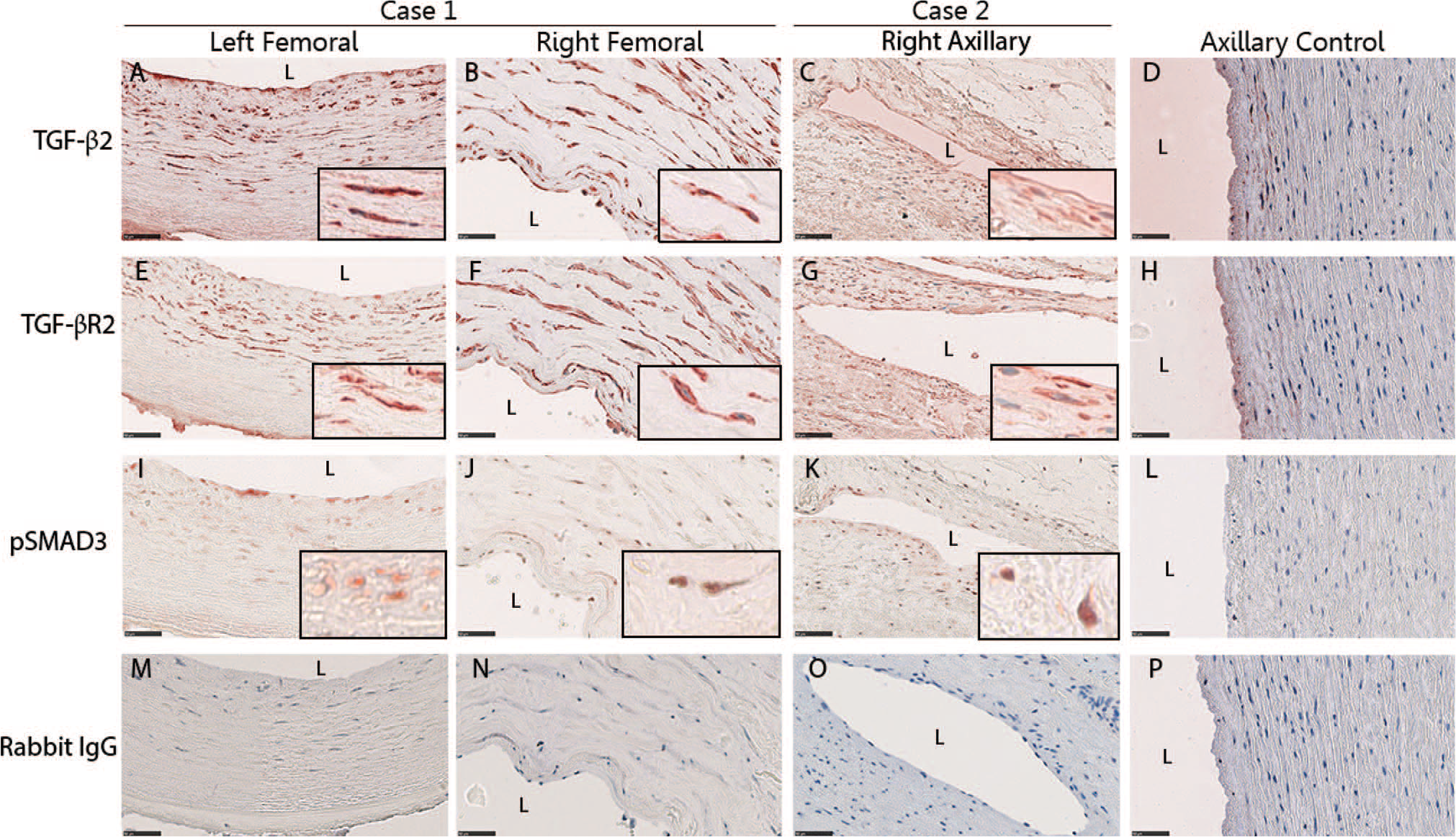
Immunohistochemical staining of transforming growth factor (TGF)-β signaling pathway molecules in femoral endarterectomy specimen and axillary aneurysm. TGF-β2 (
Published reports for KD patients with axillary and iliac aneurysms
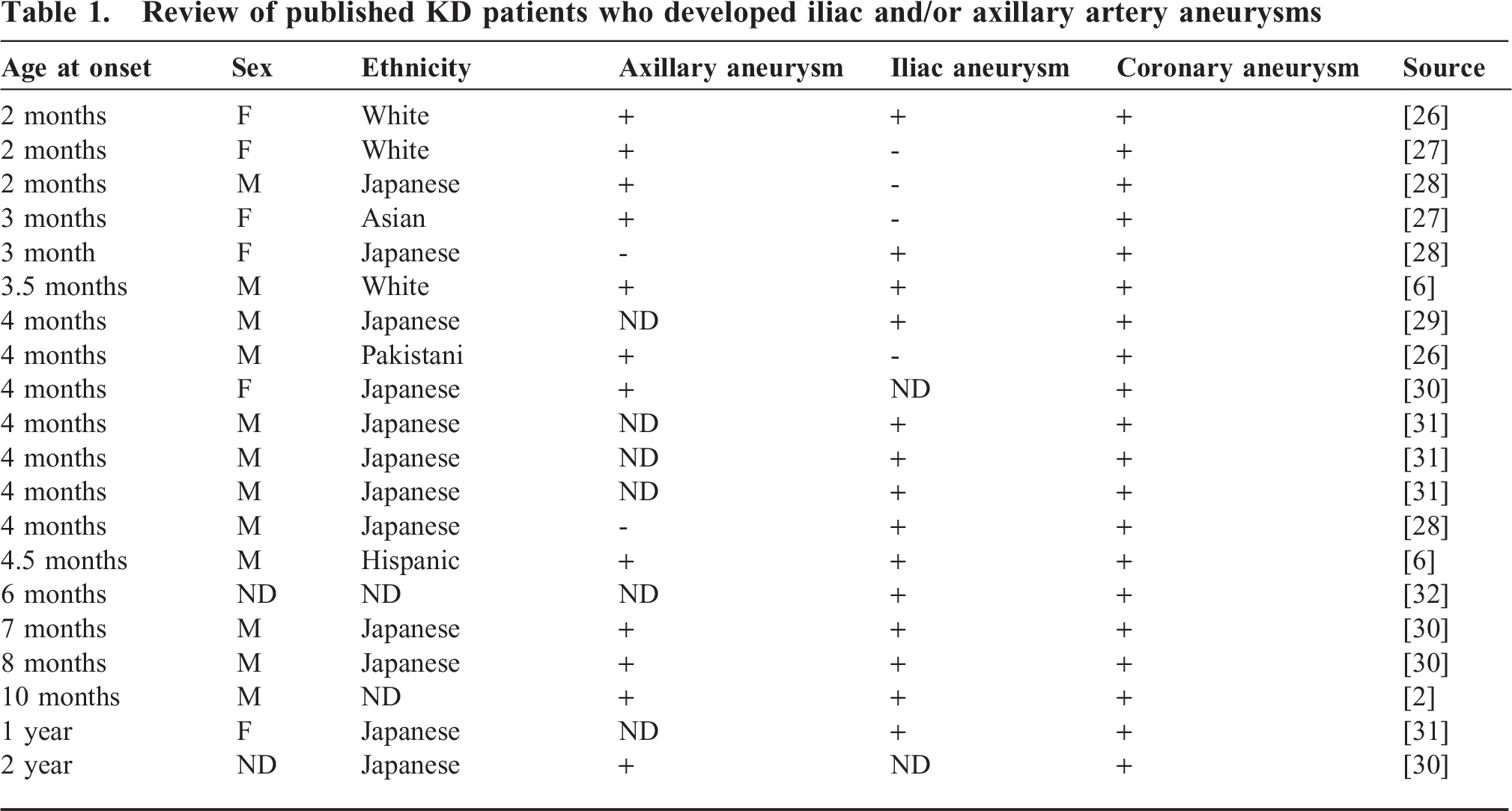
To better understand the characteristics of KD patients with axillary and iliofemoral aneurysms, we reviewed the published literature and found 20 KD patients with aneurysms in the iliac, femoral, and/or axillary arteries (Table 1). All 20 patients had coronary artery aneurysms. Notably, 15 of these 20 KD patients (75%) had their onset of KD at 6 months of age or younger. Six patients had aneurysms in the axillary and iliofemoral arteries.
Review of published KD patients who developed iliac and/or axillary artery aneurysms
DISCUSSION
Severe coronary artery vasculitis associated with acute KD also may be accompanied by pathologic changes in noncoronary extraparenchymal muscular arteries. This complication appears to be most common in infants less than 6 months of age, perhaps due to the immaturity of the immune system and a reduced capacity to localize the inflammation to the coronary arterial bed. The pathologic changes in the resected axillary artery aneurysm reported here appeared similar to structural changes described in the coronary arterial wall from autopsies of convalescent KD patients. Hallmarks of these changes include myofibroblastic luminal proliferation with focal destruction of the internal elastic lamina, recanalization of the thrombosed aneurysm with the classic “lotus root” pattern, fibrosis, and calcification of arterial wall [6,7]. Immunohistochemical analysis revealed increased TGF-β pathway signaling in the aneurysmal wall from the axillary artery and endarterectomy specimen, suggesting a role for TGF-β in the remodeling of aneurysms.
Medium-sized, extraparenchymal, muscular arteries are the target sites of aneurysm formation in KD [8]. Coronary artery aneurysms form in 25% of untreated KD patients and an estimated 2% of KD patients with coronary artery aneurysms also form aneurysms in noncoronary arteries [9], with the iliofemoral and axillary arteries as the most commonly involved sites [3].
While the genesis of the immune response directed against the coronary arteries in KD is incompletely understood, the location of aneurysms at branch points has been attributed to flow characteristics in these regions with reduced wall sheer stress (WSS) as a contributing factor to aneurysm formation [10,11]. Varying levels of WSS leads to differential expression of genes in endothelial cells [12]. In an analysis of 111 KD patients, 90.3% of CAA formed at branch sites, and branch sites were noted to have significantly reduced WSS [10]. Reduced WSS and increased particle residence time in CAA in KD also have been correlated with thrombus formation [13,14]. The large branch point in the iliac artery, which is associated with reduced WSS, is the most common site for aneurysm formation [11]. The axillary artery also branches into several smaller arteries, which may create regions of reduced WSS. Aneurysm formation may be orchestrated by reduced WSS plus regional upregulation of proteolytic pathways, inflammation, and loss of arterial wall matrix [11].
Several additional factors may contribute to the predilection for aneurysm formation in the iliofemoral and axillary arteries in patients who have KD in the first six months of life. First, the iliac arteries undergo a shift in the distribution of blood flow during the transition from fetal to extrauterine life. In fetuses, the common and internal iliac arteries form a direct continuation of the abdominal aorta to the umbilical arteries. During the first few months of life, flow is redirected to the external iliac arteries and the lower extremities, while the internal iliac artery becomes relatively smaller because, after birth, it only supplies the pelvic viscera and the surrounding tissues. The shift in mechanical load may lead to structural changes in the arterial wall that, in the presence of the inflammation associated with acute KD, lead to weakening of the arterial wall [15].
A contributing factor for the formation of axillary artery aneurysms could be the repetitive positional compression, in which the humeral bone compresses the axillary artery during movements of the upper extremity. This repeated stress may lead to weakening of the arterial wall, which in turn may lead to aneurysm formation [16,17]. While this phenomenon has been invoked to explain axillary aneurysms in professional baseball pitchers and other overhead throwing athletes [17], it is possible that young infants who repeatedly rotate their arms above their heads may produce similar structural stress on their developing axillary arteries. This mechanical stress coupled with the acute vasculitis of KD may contribute to aneurysm formation at this site.
Reduced WSS is associated with upregulation of a number of genes [11], including those in the TGF-β signaling pathway [18]. The TGF-β signaling has an important role in aneurysm formation in other conditions, including giant-cell arteritis as an example of an inflammatory aneurysm syndrome [19,20]. Mutations in fibrillin, a protein that sequesters TGF-β, and in TGF-β receptor2 are associated with increased TGF-β signaling and aneurysm formation in Marfan and Loeys-Dietz syndromes, respectively [21]. Genetic association studies have suggested a role for polymorphisms in genes in the TGF-β signaling pathway in predisposition to CAA formation in KD [22]. The TGF-β has a role in the creation of myofibroblasts via endothelial-to-mesenchymal transition. Cells with a myofibroblast phenotype have been detected in the coronary arterial wall in KD autopsy tissues and likely have a role in recruitment of inflammatory cells into the arterial wall [5]. The TGF-β may have an important role in transformation of myofibroblasts during the acute phase of KD. Increased expression of TGF-β signaling molecules in the endarterectomy specimen and the resected axillary artery aneurysm years after acute phase of KD suggests a role for TGF-β in the remodeling of peripheral artery aneurysms as well. The TGF-β may stimulate myofibroblasts to produce collagen and the combination of TGF-β and elastin degradation products can transform myofibroblasts into osteogenic cells that may participate in the diffuse vascular calcification that is so characteristic of KD aneurysms [23,24]. Although TGF-β is considered to be atheroprotective because of SMAD-dependent inhibition of foam cell formation [25], the right iliac artery from Case 1 had a small atherosclerotic plaque in the thickened intima.
We recognize several strengths and limitations of our study. To our knowledge, this is the first study to describe the detailed clinical course and the histology of peripheral artery aneurysms decades after acute KD in infancy and to provide immunohistochemical analysis of TGF-β signaling in the aneurysm wall. Limitations include the small sample size and the inability to perform electron microscopy to verify the myofibroblast phenotype of the spindle-shaped cells.
In summary, KD patients less than 6 months of age are at increased risk for development of axillary and iliac artery aneurysms that may lead to severe ischemic symptoms in the distal limb in adulthood. The TGF-β signaling pathway may influence remodeling in peripheral artery aneurysms in KD. The TGF-β pathway may be a therapeutic target to interrupt the progression of arterial aneurysms and a clinical trial of atorvastatin, which blocks myofibroblast formation, is in progress in patients with acute KD (clinicaltrials.gov; NCT01431105).
Footnotes
ACKNOWLEDGMENTS
We thank Nissi Varki, MD, and MaryAnn Lawrence at UCSD Histopathology Resources Cancer and Mouse Histopathology. We thank Jennifer Meerloo for imaging support at UCSD Neuroscience Microscopy Shared Facility and DeeAnna Scherrer for technical assistance. We thank Denise Malicki, MD, PhD, and Keith Rapp at Rady Children's Hospital San Diego for the kind gift of control tissues. We thank the Cooperative Human Tissue Network in their efforts to procure control tissues. We thank the patients who donated their tissues for these studies.