
Abstract
Children's healthcare has evolved over the years, and the pediatric laboratory has contributed to the clinical understanding of childhood disease through the application of new technology and knowledge. This article highlights the evolution of PCR technology to aid in the diagnosis of pediatric infections, from the discovery of the PCR, through the subsequent years when the clinical need exceeded the capability of the technology, until the current day, when application of the PCR is becoming commonplace.
INTRODUCTION
“I would also plant Mrs. Savage, because I could learn more.”
Little did John know that what he wrote about his garden would demonstrate remarkable insight. Sitting beside John at his college graduation, 15 years after he wrote his essay, the professor apprised us, through a video on YouTube [1], that we are living in exponential times. The amount of technical information is doubling every 2 years, which means for students beginning a 4-year college degree, half of what they learn will be outdated by their third year.
This explosion of technical information and the rate at which it is occurring impacts all of pediatric medicine and especially the laboratory. Pragmatism requires that we be judicious about how we incorporate new technology, discerning about how we interpret what we are implementing, and collaborative in that we work with our clinical colleagues to meet their needs as they care for the child. It is in this “space” that pediatric pathologists and laboratorians reside, focused on the needs of the child while keeping abreast of the latest laboratory testing to treat them. “A pediatric pathologist is expert in the laboratory diagnosis of diseases that occur during fetal growth, infancy, and child development. The practice requires a strong foundation in general pathology and substantial understanding of normal growth and development, along with extensive knowledge of pediatric medicine” [2]. We are bound together by the faces, the stories, and the love and caring that exists in the world of children's health care.

This article is about polymerase chain reaction (PCR) in the setting of children's health, the discovery, struggles, promise, and finally delivery of a technique to help children with infections get better faster. It really is that simple and was such a long journey, as we watched children who desperately needed all that the technology could promise but with a technology that could not meet the need in a way that it should have, until recently.
So having the remarkable opportunity to watch and be part of the evolution of the testing that cares for the child has been a great “ride,” so to speak. It is with this view that I write this article, celebrating the 50th year of the Society for Pediatric Pathology, and in recognition of all the individuals who care for those who are so young. It is also important to recognize our sister society, the Paediatric Pathology Society, which celebrated its 50th anniversary in 2014, and the contributions of many in the European community to the evolution and clinical application of this technology.
THE FOUNDERS
Infectious diseases are as much a part of the pediatric entity as the kids themselves. Day care centers, schools, and the immature pediatric immune system provide an excellent breeding ground for the symbiotic relationship between microorganisms and their little hosts, most of the time with the human host winning the battle, until the organism is passed on to another unwitting victim. Sentinel articles describing the pathology of perinatal infections were published in the sixth volume of Perspectives in Pediatric Pathology [3]. Correlations of pathological anatomy with clinical findings led to a better understanding of the disease processes and afforded diagnoses based on evaluation of the tissue or culture of the organism.
DISCOVERY
To quote Albert Szent-Gorgyi, “Discovery consists of seeing what everyone has seen, and thinking what nobody has thought.”
It was 2 years after the founding of the Pediatric Pathology Club (from which the Society for Pediatric Pathology evolved) that Kary B. Mullis invented a technique called the PCR. Mullis and Faloona [4] published the sentinel paper entitled, Specific synthesis of DNA in vitro via a polymerase-catalyzed chain reaction in 1987. In 1993, Dr. Mullis won the Nobel prize in chemistry for his discovery of PCR methodology.
The mid-1980s left the laboratory community excited about the new method, with an understanding of the promise of technology and a great desire to use PCR to further the ability to diagnose previously elusive infections. The first application of the new PCR technology to the care of the patient was published in Science in 1985, in which Saiki and colleagues [5] were able to amplify the beta-globin gene to diagnose sickle cell disease prenatally. This was followed in 1987 by another Science publication in which the authors were able to use PCR technology to detect minimal residual disease in patients with lymphomas carrying the t(14;18) translocation [6].
As often happens, the initial applications were not where the field took off, and soon those interested in applying PCR technology to the diagnosis of infections were driving scientific publications and the commercial vendors supplying the reagents for testing. This early adaptation of PCR technology for the diagnosis of infections provided a window to a new and exciting world with the ability to detect pathogens not easily identified in routine clinical laboratory (eg, Epstein-Barr virus [EBV]), to improve the time to identification for slow-growing organisms (eg, cytomegalovirus [CMV]), or to improve the detection rate of pathogens difficult to culture (including viruses in cerebrospinal fluid [CSF] and the Bordetella pertussis bacterium). The next 3 decades focused on discovery, disillusionment, hope, confusion, and finally hope realized with adaptation of the reagents and processes that would allow the dream of using this technology in the clinical laboratory to be realized in full. This article outlines those 30 years of adaptation of a “new” technology, with a specific focus on the care of the fetus, infant, and child and a discussion not only of the utility of the technology to improve pathogen detection but a reflection on the value to the patient and health care system.
The initial focus of the PCR used to aid in the diagnosis of pediatric infections was to detect organisms difficult or impossible to cultivate or identify in the clinical laboratory. The very fact that molecular methods could detect organisms led to a plethora of articles describing the use of the technology for identification of specific pathogens. CMV was amplified from urine specimens of newborns, and the PCR was shown to be as sensitive as culture but with a much quicker time to result [7]. In 10 renal transplant patients [8], detection of CMV by PCR correlated with a positive result for CMV in 37 urine samples by at least 1 of 3 comparator assays, which were enzyme-linked immunosorbent assay (ELISA), culture, or a direct probe assay. One sample was positive by PCR only, but this patient had CMV detected by one of the comparator assays prior to or subsequent to the single positive PCR result, suggesting that the PCR-positive result was a true positive but more sensitive than the other detection systems. The observation of increased analytical sensitivity of the PCR over other methods was only a glimpse into the future, which would at some points celebrate the sensitivity and at other times curse the sensitivity of the new technology.
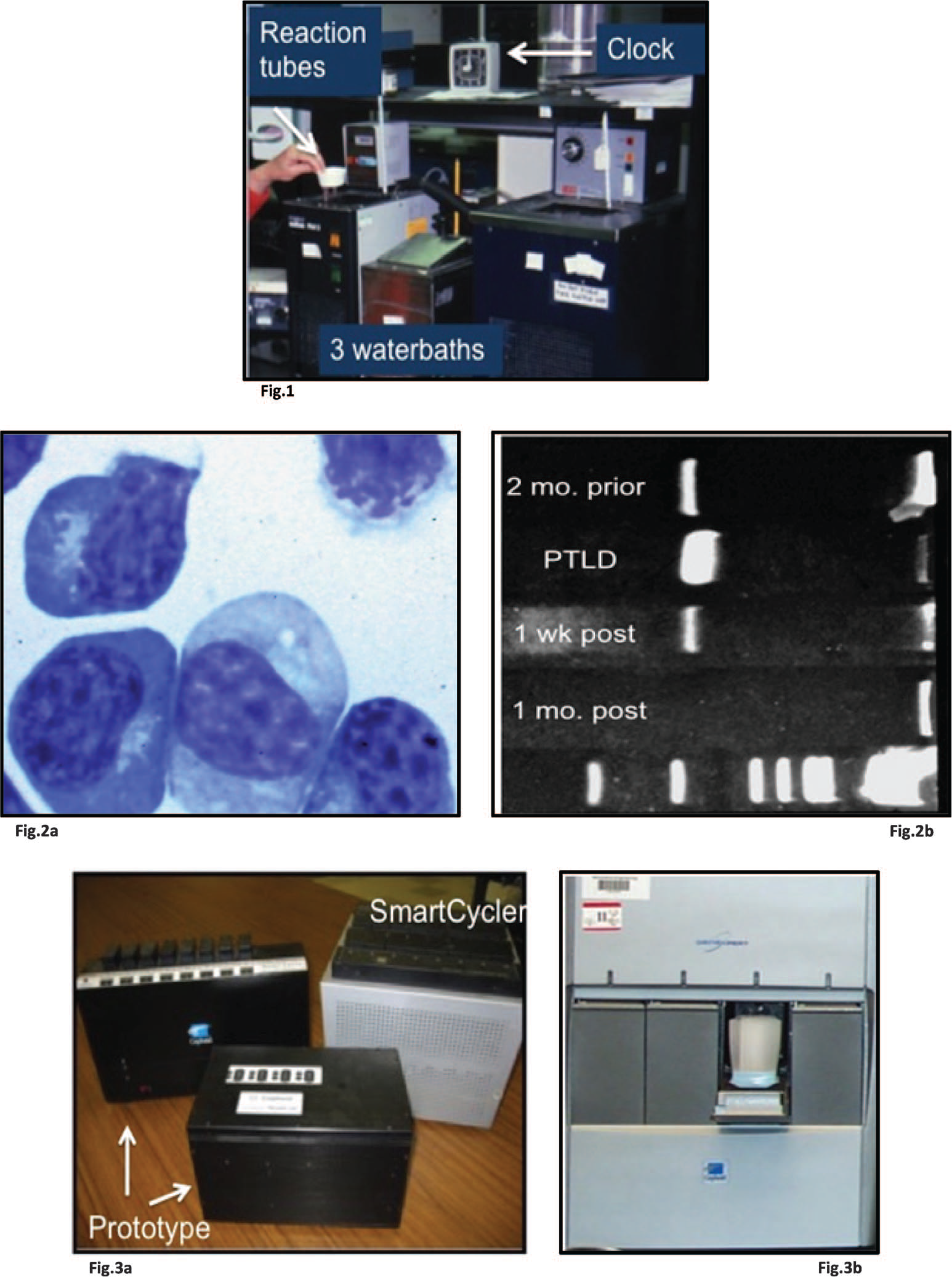
The initial method of carrying out the PCR was fraught with difficulty, requiring water baths arranged in tandem fashion to perform the denaturation, annealing, and extension steps required for the reagents to amplify the DNA (Fig. 1). The process typically took 7 to 8 hours to complete, and each of 35 steps required addition of 0.5 μL of the enzyme, Klenow fragment, because the enzyme was inactivated at 95°C, which was the denaturation step. To avoid evaporation of reagents during the PCR cycles, it was necessary to lay mineral oil on top of the reagents, producing an extremely slippery tube when attempting to add the Klenow fragment with each cycle. There were a few articles published using this method, including the articles by Saiki and colleagues [5] and Lee and colleagues [6], but soon (and thankfully) a polymerase was isolated from the organism Thermus aquaticus, the name highlighting the heat-tolerant nature of the organism and enzyme. Because it was not necessary to add enzyme with each PCR cycle, cycling through the necessary temperatures could be automated. The discovery was so profound that Science named Taq polymerase molecule of the year. Perkin-Elmer, in collaboration with Cetus Corporation, came out with the first instrument which would hold the tubes with reagents and perform the cycling without human intervention. This was the first step toward having this technology in the clinical laboratory.
DISILLUSIONMENT
According to Ray Kurzweil, “If we look at the life cycle of technologies, we see an early period of over-enthusiasm, then a ‘bust’ when disillusionment sets in, followed by the real revolution.”
With technology to simplify the cycling times came the increased use of PCR and the first realization that there was an unsuspected flaw. Amplifying a specific stretch of DNA a million or more fold was the strength of the PCR technology but also the problem. Contamination became rampant; those low-molecular-weight PCR products were everywhere: on clothes and ceilings, up nasal cavities, on pipettes, on gloves. I remember seeing contamination for the first time while working on a PCR assay to amplify herpes simplex virus DNA. We were using control herpes simplex virus (HSV), and our negative controls, which consisted of no DNA in the tube, were coming up positive. We were extracting nucleic acid, preparing reagents, mixing reagents, amplifying the DNA, and running gels to identify amplification in 1 room in the laboratory. I called Cetus Corporation and spoke with Dr. John Sninsky, the head of research and development, who shared the fact that they were finding that 3 separate rooms were needed to do the PCR because contamination was so prevalent. More than the need to find enough space and locations to do the PCR in a clinical laboratory was the simple worry that a false positive result could end in misdiagnosis.
Kwok and Higuchi [9] wrote, “A false positive or mistyping may occur when the majority of molecules to be detected arise from exogenous sources rather than from the sample itself (such as infectious pathogens).” The exquisite sensitivity of the PCR meant DNA contamination could ruin an entire experiment. “Tidiness and adherence to a strict set of protocols can avoid disaster” [9]. The authors recommended various precautions to decrease the risk of contamination, including physically separating sample preparation to a separate room from the PCR, using ultraviolet (UV) lights to inactivate carryover DNA, using positive displacement pipettes, using disposable gloves, and so forth. Keeping vigilant about contamination was the best one could do. If we began to see contamination with 1 set of reagents, we would have a back-up from another location of the gene to amplify until contamination died down. We bleached ourselves, put filters in our pipettes, ordered 4 sets of pipettes to have 1 out of circulation at each time, threw away expensive reagents we were concerned were contaminated, and tried not to cry.
The almost exclusive reason that contamination occurred was the opening of the tube that held the product of the PCR, which was required in order to analyze the product, such as running a gel to determine if amplification occurred. Quickly, laboratories moved to separating PCR preparation and analysis into 3 rooms: extraction, preparation of PCR reaction mixture, and amplification and detection of product. The rooms were required to have separate airflow, and the extraction and amplification/detection rooms were optimal if they had negative pressure, whereas the PCR preparation (the clean room) had positive pressure. In addition, movement from one area to the other was in 1 direction only, with new laboratory coats and gloves donned before entry into the next area. Pipettes were separated so there was no entry from one area into another, and bleach cleaning was carried out with vigor for pipettes, countertops, hoods, and other surfaces. Researchers and laboratorians would use uracil-N-glycosylase to degrade contaminating DNA prior to PCR, UV light, autoclaves for sterilization, decreased numbers of PCR cycles, and still contamination would occur [10,11]. It became reasonably clear that the PCR was not “ready for primetime” clinical laboratory application, and testing was usually performed only in academic medical centers or in reference laboratories. The College of American Pathologists developed checklist questions based on contamination containment procedures, and some of these questions remain in the checklist today, although the risk of contamination in the current era is much less than in previous decades due to technological advancements.
HOPE
It was Jonas Salk who said, “Hope lies in dreams, in imagination, and in the courage of those who dare to make dreams into reality.”
Despite the difficulties with using PCR, the need for the patient became so great that the testing was considered useful, even if the time to result was long, the cost was great, and the chance of false positive results often left a lingering doubt in the caregivers' minds about the validity of the result. Some of the initial targets for use of the PCR were HSV, EBV, and CMV, in the immunosuppressed patient, and parvovirus B19.
Culturing CSF for HSV was notoriously unreliable, and this was highlighted in the neonate with fever or seizures, in whom HSV meningitis/encephalitis was on the clinical differential diagnosis. Essentially, if HSV infection was suspected, the neonate was committed to a 21-day course of antiviral agents, requiring hospitalization. A test that was sensitive enough to identify HSV with certainty in the CSF of neonates would drastically reduce the use of antiviral agents and avoid the long hospitalization for the babies.
Rowley and colleagues [12] published their PCR method to detect HSV in the CSF and validated the method in cases of biopsy- or autopsy-proven HSV encephalitis. Simply, 4 of 4 patients with HSV in brain tissue samples were positive in the CSF using the PCR method, and 6 of 6 patients with central nervous system infected by other than HSV were negative for HSV, using the PCR. They stated in their short report, “Enzymatic amplification (using the PCR) offers an advantage over culture because the technique does not require the presence of intact non-antibody-bound viral particles, and may avoid the need for brain biopsy” [12].
The early evolution of the PCR method paralleled that of solid organ transplantation becoming commonplace. Pharmacologic immunosuppression of the organ recipient resulted in the inability of the recipient's immune system to respond appropriately to a host of pathogens difficult to identify, but the most devastating pathogen initially seemed to be EBV. Children were particularly at risk because their already naïve immune system was further immunosuppressed and so were more likely to be without innate immunity to EBV, resulting in greater chance of post-transplant lymphoproliferative disorder (PTLD) than adults with transplants. Infection with EBV, if not held in check by the host immune system, results in widespread proliferation of (typically) B-lymphocytes, which may take on a biologically malignant phenotype and cause the death of the patient. Because of the complexity of these patients and the relative nonspecificity of symptoms of EBV infection, there was a great need to identify the virus in patients who had received transplants and particularly those very young patients who were still uninfected with EBV at the time of transplantation.
Serologic diagnosis of EBV infection had been the mainstay for several years. For typical acute infections in the teenage or young adult host, the monospot was, and is, a simple and fast test. However, for children under 5 years of age and those who are monospot-negative, a complete serologic evaluation was performed, and a pattern of 4 antibodies (IgM-VCA, IgG-VCA, EA, and EBNA) was used to determine whether EBV infection had occurred. Unfortunately for the patient with a solid organ transplant, the serologic response to the virus was blunted, and often patients were serologically nonreactive in the face of widespread EBV-infected cells in their blood and organs. Because PCR amplification for EBV was a very sensitive method to detect the virus, this test became the method of choice to determine whether EBV was present in the transplant recipient.
Telenti and colleagues [13] used PCR to identify EBV in DNA extracted from 25 patients with solid organ transplants and 11 seropositive healthy adults. They identified EBV genome in 11 solid organ patients, and 5 of these patients were followed and had multiple samples positive for EBV. The investigators also amplified EBV from tissue samples of patients with PTLD. The DNA extracted from healthy adults was negative for EBV. They concluded, “Further study is necessary to determine the significance of finding EBV sequences in the blood of immunosuppressed patients, particularly in relationship to the development of lymphoproliferative disorders” [13]. During that same year, Gopal and colleagues [14], a group working in the United Kingdom, amplified DNA extracted from peripheral blood mononuclear cells and identified EBV genome in half of the healthy adults studied, in contrast to the findings of Telenti and colleagues [13].
CONFUSION
As Anne Grant observed, “Confusion is the hallmark of a transition.”
Quickly, after pathologists began using EBV PCR testing of peripheral blood to aid in the diagnosis of PTLD, it became clear that PCR analysis might actually be too sensitive in this regard, as many patients who were EBV PCR positive were clinically healthy. Although transplantation increased the chance of identifying EBV by using PCR analysis, even healthy people who were not immunosuppressed could be PCR-positive for EBV. There was concern that interpretation of the assay, which had shown such promise because of its ability to detect that which routine methods could not, might be impossible.
Lack of standardization was apparent, and simple differences in methods resulted in entirely different results. An example are the articles by Telenti and colleagues [13] and Gopal and colleagues [14], noted above, which evoked the following analysis showing that the PCR assay by Gopal and colleagues was designed to be more sensitive than that of Telenti and colleagues. Extraction from a sample enriched for lymphocytes, which contain EBV, and an increased number of PCR cycles made Telenti's PCR assay more sensitive (Table 1).
Comparison of methods and results

EBV indicates Epstein-Barr virus; PCR, polymerase chain reaction; PTLD, posttransplant lymphoproliferative disorder.
Approaching a pediatric liver transplant surgeon in 1992, Dr Walt Andrews, about whether he would be interested in having us develop a PCR test to detect EBV in the blood of his patients, he responded that the technique was too sensitive and that the test was not useful for his patients. Knowing that we could make the assay as sensitive or insensitive as necessary by modifying the conditions of the PCR, we engaged him to join in a study to determine whether the PCR could provide meaningful information for him to predict which of his patients were at risk of developing PTLD and to also follow response to withdrawal of immunosuppression following the diagnosis. Therefore, we developed a test and began to report whether patients were EBV-positive or -negative by PCR, and the test was used to assist in determining which patients might develop PTLD, but it was far from perfect.
Does the amount of circulating EBV correlate with PTLD? An answer to this question was suggested as I was evaluating a patient's pleural fluid one day. The fluid was full of atypical lymphocytes, plasmacytoid lymphocytes, and lymphoblasts, characteristic of PTLD (Fig. 2a). Turning to sign out the EBV PCR tests for the day, there was a photograph of a gel that had the results of this patient's peripheral blood EBV PCR test, and it was a large, bright band, indicating that a large amount of virus was present in the sample (Fig. 2b, lane marked PTLD). It was at this point that we began reporting the bands on a gel as being mild, moderate, or strong to provide (although admittedly crude) more information to the clinician about their patient's EBV burden.
The next question regarding the PCR technology was whether there was any benefit to having an assay that was quantitative. In other words, simply finding the organism might be sufficient in some disorders, such as HSV encephalitis, but it seemed there was a need to determine how much organism was present for other viruses that are normally present in minute quantities in the human host.
The early days of developing and performing quantitative assays resulted in, at best, a semiquantitative test. Dilutions of the PCR reaction mixture were made and compared to dilutions of a standard, and the level of organism was calculated from the endpoint. Precision was lacking due to the fact that the precision of the PCR reaction at the endpoint was variable. Due to the sensitivity of the assay, 1 organism can be detected in some assays, but if 1 organism happens not to end up in the pipette tip to be dispensed into the PCR reaction mixture, then the result will be negative. Regardless of the complexity of these assays, they were necessary to provide the clinical information for the care of the immunosuppressed child, and so they were used, typically restricted to academic or larger reference laboratories with highly specialized technical personnel.
Still, associations were made between the quantity of EBV in the peripheral blood and disease, and it became clear that children with PTLD were more likely to have high circulating viral burdens than those without PTLD [15–17].
It was not until the next evolution of technology that true quantitation of organisms using PCR was possible. There was a stretch of approximately 10 years when the techniques were cumbersome and the real-time detection of organisms causing pediatric disease was simply not available. So, the last evolution, development of real-time PCR testing, is the last chapter of this story, and finalizes the implementation of the “new” technology in the clinical laboratory to help treat children 24 hours a day, 7 days a week.
HOPE REALIZED
Like Tyler Perry said, “There are a lot of people who have dreams, goals, and hopes, but there aren't a lot who get to see them realized.”
The next evolution of the PCR technology was sentinel to improving patient care and providing the opportunity for the PCR methodology to be adopted more routinely into the clinical laboratory. This was the invention of real-time PCR testing, which used fluorescence to detect the PCR products to differentiate not only a positive from a negative result, but to be able to quantitate organisms during the growth curve, which provided a much more accurate determination of quantity than the endpoint detection used previously. Real-time PCR testing also had a revolutionary advantage in that the tube with the PCR products did not have to be opened for further analysis, as the analysis was done in the instrument during the PCR. The need for stringent contamination containment was no longer necessary because PCR products were not released into the laboratory from opening the reaction tubes, so the clinical laboratory became a fertile ground for PCR testing. Complexity still existed because extraction of the sample prior to the PCR and the reagent preparation prior to the PCR typically did still require a separate space and ventilation. However, the most difficult problem, that of the floating PCR product, had been solved.
Something else happened around this time to prepare the community for the next leap in molecular testing for infectious diseases. This was the idea that we might be able to develop PCR instruments that could provide random access PCR analysis by including sample extraction in addition to PCR and detection. This would make it possible to have this testing on a 24-hour, 7-day basis, or even at the point of care. Two real-time thermal cyclers became available at the turn of the century, whose companies existed through the next decade and a half to incorporate extraction into the reaction, creating easy-to-use technology without the need for special space considerations or technologist training.
Dr Carl Wittwer, Dr Randy Rasmussen, and Mr Kirk Ririe founded Idaho Technologies in 1990. Dr. Wittwer, professor of pathology at the University of Utah, developed the LightCycler, which was introduced to the market in 2001. The LightCycler was extremely fast, with time to result of some assays as low as 15 minutes [18]. This technology was purchased by Roche and is used in many laboratories today. Idaho Technologies continued to maintain a separate identity and headed down a path to produce packets of reagents to which raw sample could be added and multiple targets could be amplified and detected without opening the instrument; the single-piece flow. Idaho Technologies became BioFire, which was purchased by bioMerieux but retained the founders named above, who continue to push the limits of PCR methodology.
At the same time, a group in Sunnyvale, California, was working on a real-time PCR instrument that could handle 1 sample at a time with the ultimate goal of having the PCR instrument at the point of care [19]. Thomas L. Gutshall, Bill McMillan, Dr Kurt Petersen, Dr Greg Kovacs, and Dr Allen Northrup founded Cepheid in 1996, and they had the vision of bringing PCR testing to a level of function where it could be incorporated into routine diagnostics. The founders published a method of nucleic acid extraction which could be performed in a closed system, with the vision of linking this extraction to realtime PCR methodology in a cartridge, which would later be called the GeneXpert. The SmartCycler was a precursor to the GeneXpert and had a unique design in that the instrument was designed to handle a total of 16 samples, but it was possible to perform testing on each of the 16 samples independently, essentially a precursor to the possibility of single-piece flow and point of care capability (Fig. 3a,b).
Following this technological advancement at the beginning of the 21st century, testing using the PCR methodology began to flourish. Reagents were more often available for purchase, US Food and Drug Administration clearance was sought and achieved for many of the tests, and testing children with transplants for EBV and CMV became commonplace. The assays were actionable, and PTLD in children was diagnosed earlier in the course of disease, with marked improvement in patient outcome [20]. BK virus burden was added to the list of routine testing for renal transplant recipients, and adenovirus as well.
Testing for the otherwise healthy child became more common. Initial identification of limited panels of respiratory pathogens in an immunosuppressed patient [21] quickly expanded into testing for a large number of respiratory pathogens, including influenza, parainfluenza, respiratory syncytial virus (RSV), adenovirus, metapneumovirus, rhinovirus, enterovirus, and coronavirus [22]. Luminex developed the first large panel for detection of these viruses, not by using real-time PCR but by detecting the amplified products using a fluid microsphere analysis as the detection step performed after PCR analysis. This was popular, as it was the only methodology that could detect the large number of pathogens identified above. However, the analysis required opening the PCR tubes, taking us back to the time when PCR contamination was a problem. Other manufacturers developed reagents selected for specific pathogens, or small panels, and many laboratorians developed and used their own laboratory-developed tests.
The next technological advancement came about 5 years after the introduction of real-time PCR. Remember that with the current methods, it was necessary to extract nucleic acid prior to the PCR test. This limited the ability of the testing to be done by laboratory personnel who were not highly trained, and also required that a clean room still be present in order to ensure a noncontaminated reaction. Cepheid, which had developed the SmartCycler, was the first on the market with a PCR test contained in a cartridge, with a “walk-away” platform that did not require extraction of the sample and could be done on any bench top in the laboratory. The instrument, called the GeneXpert, was the true vision of the initial group who invented the SmartCycler, and that vision was finally realized. The instrument essentially automated what was an historically laborious procedure and moved quickly into the diagnostic realm of the more commonplace, targeting patient populations such as women in labor (group B streptococcus), children with suspected meningitis (enterovirus) or Clostridium difficile-associated diarrhea. Patel and colleagues [23] noted that the technology “features on-demand availability and a level of simplicity that allows nearly any hospital laboratory to offer a sophisticated test that was once the exclusive domain of reference laboratories.”
Other manufacturers were developing platforms that incorporated extraction, amplification, and detection and included both qualitative and quantitative testing. Transplant viruses were now available in a sample-to-result system. This requires pipetting blood, plasma, or CSF into a small well, closing the instrument, and obtaining a result. There is no extraction necessary. Even more aligned with application to routine clinical laboratory testing around the clock and 7 days a week or the point of care is an instrument developed by Idaho Technologies (later named BioFire), which uses a dilution buffer, hydration buffer, and a pouch to afford a multiplex result for multiple pathogens in approximately 1 hour and includes not only viruses but also pathogenic bacteria [24]. The respiratory panel detects 20 pathogens in an hour and is listed as moderately complex by the Clinical Laboratory Improvement Amendments. Many other manufacturers joined the “technology chorus,” and seeming exponential development of molecular infectious disease testing is at hand.
The easier it is to detect organisms, the more organisms will be detected, and an increased number of clinical applications will be identified. It is now routine to use PCR to test children for viral burdens of EBV, CMV, BK virus, and adenovirus when they are immunosuppressed and to follow the viral burden to predict occurrence of disease or follow response to therapy. The pathogenic causes of meningitis, including enterovirus, HSV, and parechovirus, are tested using PCR. CMV burden predicts hearing loss in symptomatic and cases of asymptomatic congenital CMV infection [25,26]. High viral load for human metapneumovirus correlates with lower respiratory tract involvement in children infected with the virus [27]. Group A streptococcus can be diagnosed with molecular methods at the point of service, replacing the rapid antigen test and culture. Identification of influenza using a rapid multiplex PCR analysis, performed around the clock and 7 days a week, improves throughput in the emergency department and decreases time to treatment [24], and implementation of a rapid respiratory panel decreases length of hospital stay and antibiotic use [28].
THE QUESTIONS
Albert Einstein counseled, “Learn from yesterday, live for today, hope for tomorrow. The important thing is not to stop questioning.”
And so we find ourselves in conversations similar to those carried out over 20 years ago when we struggled with the meaning of a positive EBV PCR result in a child after organ transplantation. Detecting 20 respiratory pathogens around the clock provides answers to the presence or absence of virus, but what does the result actually mean? A matched case control study assessed the clinical correlation of viral pathogens identified by PCR testing [29]. Viruses detected included influenza, adenovirus, bocavirus, coronavirus, enterovirus, human metapneumovirus, rhinovirus, parainfluenza virus, and RSV. The authors concluded that RSV, human metapneumovirus, and parainfluenza virus were identified in children presenting with respiratory illness compared to controls. Bocavirus was associated with severe respiratory disease. However, rhinovirus, adenovirus, coronavirus, and enterovirus were prevalent in controls and in children with respiratory illness, so the authors recommended caution in interpretation of positive results for these viruses. Coinfections were present in 20% of patients with symptoms of respiratory illness but only 5% of control subjects.
BRINGING IT ON HOME
Albert Einstein advised, “Try not to become a man of success but rather a man of value.”
I would be so bold to say that we are better off today than we were 20 years ago in the arena of diagnosing childhood infections. We do not know it all and are not always comfortable, and with each new accomplishment comes a new horizon to strive for, new improvements to make, and more questions about clinical application and actual worth of what we report to the clinicians in the context of the health care system. But we strive for value: to add value, to be valued, and to provide our patients with the best care in our role as pediatric pathologists. So, what is going on these days with PCR testing, which has at this point garnered success as a technology? “Extreme PCR” [30] is on the horizon, invented by and demonstrated in an article by Farrar and Wittwer [30]. The subtitle of the article goes on to state: “Efficient and Specific DNA Amplification in 15–60 Seconds.” Published by clinical laboratorians, the summary sentence states, “We hope that the demonstrated feasibility of extreme PCR will encourage further work on practical implementation that may lead to commercial devices that improve the turnaround time for molecular testing, leading to better patient satisfaction and care” [30]. Better patient satisfaction and care, better value, is where the Institute of Medicine is leading us. We hope to be able to answer the call for value-based care for our patients who, after all, are our future.
Footnotes
ACKNOWLEDGMENTS
I would like to express my appreciation to Drs Milton Finegold and Greg Buffone for the opportunity to learn; Dr Don Singer, who supported a start-up molecular diagnostics lab; Dr Art Weinberg, who said I couldn't quit molecular diagnostic work when I was “done” with it all; Nora (Kristi) Leos, a remarkable scientist and co-inventor; Bill McMillan, for great conversations; Dr Brett Giroir, for having (and funding) the vision; Jim Adams, for administrative partnership and support of the innovative; the Advanced Diagnostics groups at Children's Medical Center Dallas and Children's Healthcare of Atlanta, who are invested in pushing the envelope; Tom, Robert, and John, for wonderful partnerships; and the kids and their families, who give us purpose.