
Abstract
Massive placental perivillous fibrinoid deposition in the placenta is thought to be an immune-related condition associated with poor perinatal outcomes, including growth restriction and intrauterine fetal demise, with a high risk of recurrence. Rare cases have been associated with Coxsackievirus infection. We present such a case and review the literature.
Keywords
INTRODUCTION
Massive placental perivillous fibrinoid deposition (MPVFD) and the related entity on the spectrum, maternal floor infarction [1], along with chronic lymphohistiocytic intervillositis and chronic villitis of unknown etiology, are lesions of uncertain etiologies that have been considered of alloimmune origin. In addition to having high rates of recurrence [2,3], they are associated with poor perinatal outcomes, including growth restriction and stillbirth [4]. Recently, we encountered a case with maternal hand-foot-and-mouth disease and strong clinical history suspicious for Coxsackievirus as the cause of fetal demise. The placenta showed MPVFD, and the diagnosis of Coxsackievirus A16 infection was subsequently confirmed. This association between Coxsackievirus and MPVFD has been noted at least twice before in the literature [5,6], and it is possible, in some cases, that MPVFD may have represented unrecognized enterovirus infection.
CASE
This was a 28-week-gestational-age stillborn infant delivered to a mother with no significant prior history who presented with fetal demise. Five days prior to presentation, the mother reported a rash and mouth sores. Her older child's school had had a recent reported case of Coxsackievirus; no further details were available to us. At autopsy, there were no significant gross or microscopic findings of the fetus. The fetus was appropriate for gestational age and there was no fetal or placental evidence of prolonged intrauterine retention. The placenta was markedly abnormal, showing MPVFD. There was also patchy acute and chronic intervillositis, and necrotic or karyorrhectic debris in the maternal space that appeared to be of trophoblast origin (Fig. 1). There was no evidence of trophoblastic proliferation. Immunohistochemistry (IHC) was positive for enterovirus in trophoblast (Fig. 2). Electron microscopic studies found picornavirus particles within syncytiotrophoblasts (Fig. 3). Enterovirus molecular detection and genotyping by reverse transcription–polymerase chain reaction (PCR) and sequencing were performed from formalin-fixed, paraffin-embedded tissue at 2 separate laboratories (R.T., S.Z.), and both confirmed a diagnosis of Coxsackievirus A16 infection. Analysis of the fetal lung tissue was negative for virus by IHC and PCR.
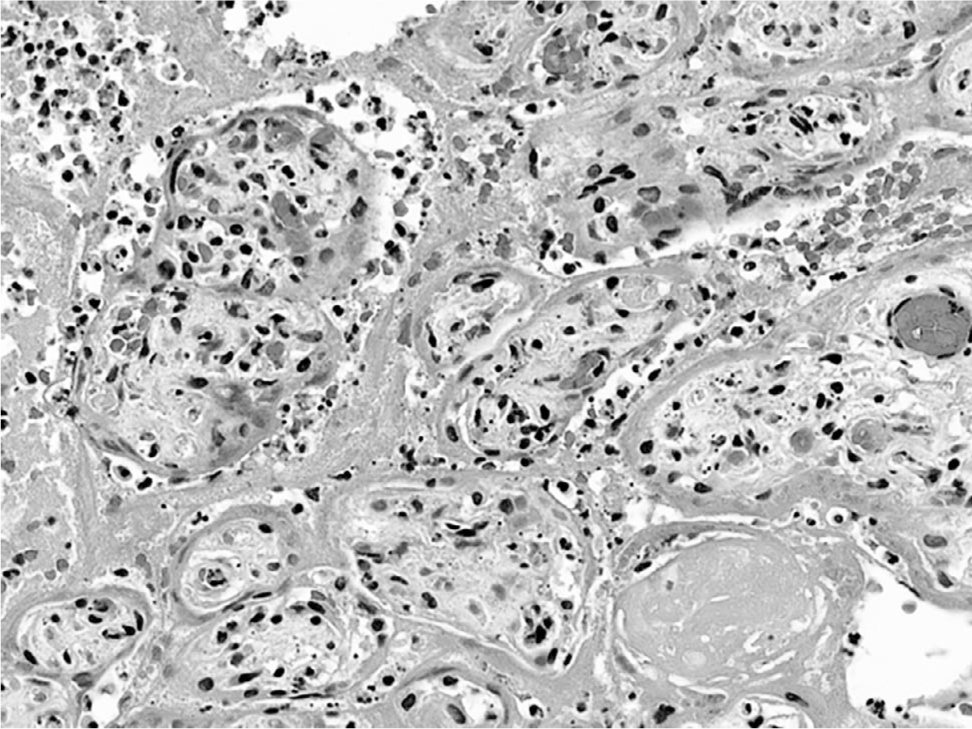
Placenta showing massive perivillous fibrin, intervillositis, and necrotic trophoblasts.
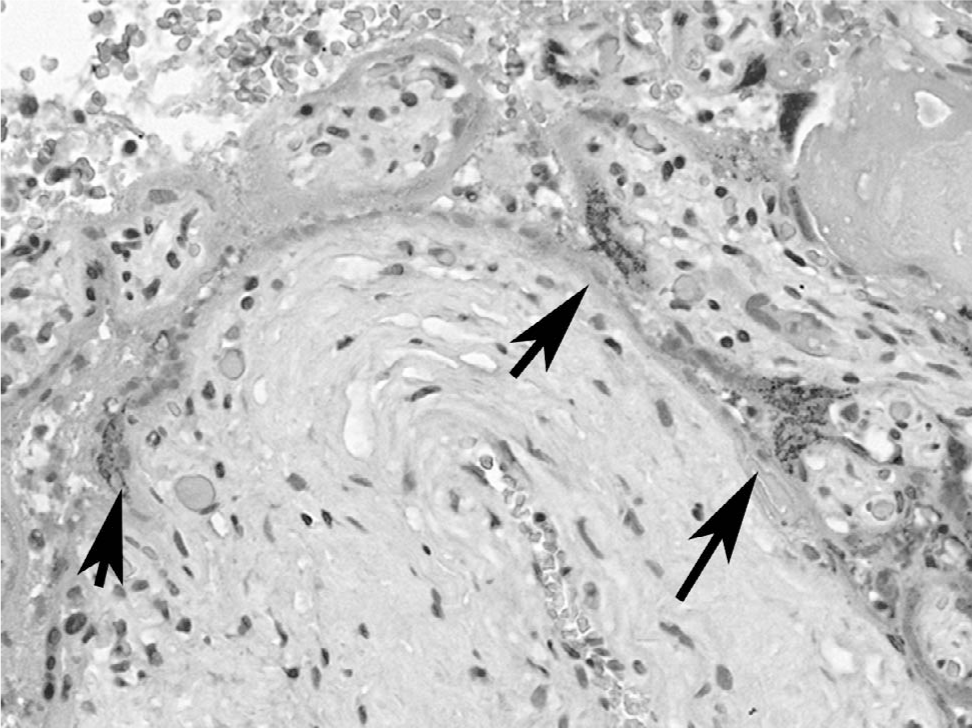
Immunohistochemistry is positive for enterovirus, in a granular cytoplasmic pattern (arrows).
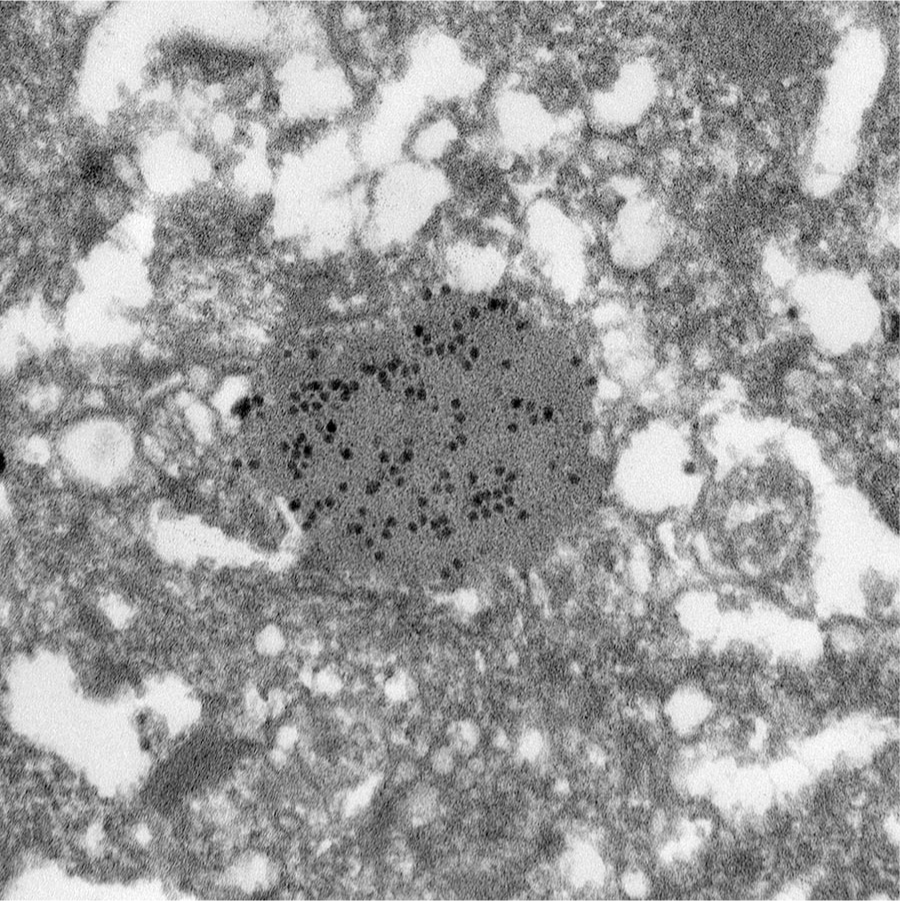
Electron micrograph showing picornavirus particles within a matrix, seen in a syncytiotrophoblast cell.
DISCUSSION
Coxsackievirus A16 belongs to species A within the genus Enterovirus. Enteroviruses constitute a ubiquitous group of viruses that usually cause asymptomatic infection, but they are causal agents of several significant human illnesses, including respiratory tract infections, meningitis or encephalitis, myocarditis, and exanthema/enanthema. Coxsackievirus A16 is a common cause of hand-foot-and-mouth disease and has also been associated with cases of respiratory tract infection and meningitis.
Transplacental infection with enteroviruses is thought to be rare [7]. It is associated with spontaneous abortion [8] and stillbirth as well as congenital or neonatal enterovirus infection with a wide range of clinical disease and organ involvement [9,10]. Most neonatal infections, however, are asymptomatic [9]. Most perinatal infections are caused by Coxsackievirus B and related echoviruses (species B), which can be associated with disseminated neonatal disease (hepatitis, myocarditis, sepsis-like illness). Enteroviruses within species A, such as Coxsackievirus A16 or Echovirus 71, appear to be less associated with perinatal disease [11].
Fetal tissue was morphologically normal and fetal lung tissue was negative by IHC and PCR, suggesting that disseminated fetal disease was not the cause of this stillbirth. Fetal demise was likely due to placental damage/insufficiency, as demonstrated by extensive necrosis/MPVFD. Enterovirus antigen and viral particles were localized to the syncytiotrophoblast, suggesting placental tropism of the virus. Syncytiotrophoblast localization has been demonstrated in echovirus (species B)-associated stillbirth [12], and trophoblast cell lines support coxsackie virus B infection in vitro [13]. Cellular mechanisms of syncytiotrophoblast infection and damage caused by other enteroviruses remain to be determined.
A recent report of the association between Coxsackievirus A16 and massive placental perivillous fibrin/fibrinoid [5] led to the consideration of the same diagnosis in the current case. In a search of the literature, only one similar case has been noted [6]. This older report did not use the term MPVFD, but the figures and description clearly show diffuse placental perivillous fibrinoid in association with intervillositis and necrotic villi, and the authors attributed the stillbirth to placental compromise [6]. Nonspecific placental lesions associated with enterovirus infection include Hofbauer cell hyperplasia [10] and chronic villitis [14]. These can also be found in hematogenously transmitted viral infections such as cytomegalovirus. Here we present what we think is the 3rd reported case of placental CVA infection associated with MPVFD. Until recently, there did not seem to be a reported characteristic placental lesion associated with enterovirus infection. Enterovirus diagnosis is feasible on formalin-fixed, paraffin-embedded tissue [9, current case]. Considering that enterovirus infections are often paucisymptomatic or asymptomatic, it is unknown whether placental infections associated with stillbirth may also be clinically silent. It is unclear at this time whether MPVFD is associated with a few serotypes such as Coxsackie A16 or whether it can be seen with different enteroviruses. It is also unclear whether some previously reported series of cases of MPVFD may have included unsuspected or otherwise clinically silent enterovirus infection. As previously mentioned, MPVFD can be recurrent, and is thought to be alloimmune mediated; these recurrent cases are less likely to be enterovirus associated. To speculate, enterovirus-associated MPVFD may more likely affect an isolated pregnancy, perhaps in women with prior successful pregnancies and subsequent increased exposure to young children and their fomites. In summary, enterovirus infection should be considered in cases of MPVFD in the placenta, particularly if there is associated villitis and villous necrosis and/or a clinically consistent picture of enterovirus infection.