
Abstract
Vehicle fire fatalities encompass both fire and traffic investigations important for the forensic pathologist. Previous studies have demonstrated the challenges in victim identification, determining cause and manner of death, evaluating the role of collision dynamics, and estimating the excess burden of deaths due to post-collision fire. To address these challenges, the present study analyzed 101 vehicle fire fatalities representing 85 accidents, six suicides, four homicides, two natural deaths and four deaths of undetermined manner. Deliberately set fires in homicides, suicides, and suspicious deaths caused nine deaths. Non-accidental deaths were twice as common in parked vehicles. Of 78 collision fatalities, 46 were occupants of cars, 47 were drivers, and 48 died in collisions involving fixed objects or non-impact rollovers. Occupants of heavy trucks and collisions with light trucks and SUVs had the highest per-collision fatality rates. Frontal and rollover collisions claimed most lives, and rear collisions had the highest fatality rate. Carboxyhemoglobin (COHb) levels were highest in parked cars wherein toxic inhalation occurred prior to fire. In post-collision fires, COHb ranged no higher than 31% saturation and were much lower than in house fires. Potentially survivable blunt force injuries (BFI) and no BFI were present in more than half of charred bodies of post-collision fires. Evidence of inhalation of combustion products correlated imperfectly with severity of BFI, and airway soot deposition was a more sensitive indicator of post-collision viability than COHb. Between 13% and 59% of collision fatalities were due to post-collision fire and not BFI.
Introduction
Vehicle fire fatalities represent a small but important subset of transportation deaths that a forensic pathologist is likely to encounter. Analysis of data in the national Fatal Accident Reporting System (FARS) estimated that approximately 1,370 fatalities occurred in passenger vehicles that experienced fires (1), and national fire statistics attributed 12% of all fire fatalities to motor vehicle fires (2). Medicolegal investigations of vehicles fire deaths encompass both fire fatality and traffic fatality investigations. Major concerns for the forensic pathologist are victim identification and determination of cause and manner of death. Despite established guidelines, there are recognized difficulties interfering with accurate determination of cause of death due to ambiguities in assessing the contributions of fire-related injuries relative to mechanical trauma (3–9). For traffic safety concerns, accurate determination of cause of death is important in assessing the excess burden of deaths due to fire, and previous studies have pointed out the difficulties in estimating the number of vehicle occupants killed who would have survived had it not been for a post-collision fire (1, 10,11). Accurate determination of cause of death is also important from the engineering perspective, in which collision dynamics, ignition and propagation of fire, fuel system integrity, and protection of the occupant are primary concerns (12–17). Furthermore, engineering studies are relevant to forensic investigations by showing where the fire originates influences the thermal and toxic environments experienced by the occupant (17). This is important when evaluating evidence of inhalation of combustion products, airway soot deposition and carboxyhemoglobin (COHb) levels, which are indicators of post-collision viability (3). Clinical studies are fairly limited with respect to scene and circumstantial details but do show that thermal burns sustained in motor vehicle fires have distinctive characteristics that are relevant for treatment, morbidity, and mortality (18, 19). In dealing with the wide range of concerns, the present study was conducted as an attempt to resolve some of the issues relevant to vehicle fire fatality investigation. Specifically, this study addressed the difficulties in certifying cause and manner of death, assessing the role of collision dynamics, interpreting evidence of post-collision viability, and estimating the excess burden of deaths due to post-collision fires.
Methods and Materials
King County Medical Examiner's Office (KCMEO) in Seattle, Washington serves a predominantly urban population of approximately 1.916 million. Geographically, King County covers 2,126 square miles extending from Puget Sound to the Cascade Mountains. Altogether there are 39 incorporated cities and towns, the largest of which is Seattle, connected by two major interstate highways. By state law KCMEO is responsible for investigating and certifying all deaths that occur in the county regardless of place of injury. This includes all deaths occurring at Harborview Medical Center in Seattle, the state's only Level I trauma center and major burn unit, which receives trauma referrals from other Washington counties as well as from Alaska, Idaho, and Montana. For deaths occurring at the scene of the incident, KCMEO medicolegal death investigators conduct scene investigations and file reports summarizing their findings and incorporating information from law enforcement and other agencies. Scene investigations are not performed by KCMEO investigators in hospital deaths, in which information comes from law enforcement reports and medical records. Complete autopsies with toxicology analyses are performed for all scene deaths involving motor vehicles and fires. Autopsies are not performed in all hospital deaths, especially if there is no likelihood of criminal charges and sufficient information is present in the medical records to allow accurate assessment of injuries and death certification. Investigator reports summarizing the scene, circumstances, relevant medical records, as well as demographic and other information regarding the decedent and the incident are maintained in a single computer database (VertiQ Software, Morgan Hill, CA) for all deaths investigated by KCMEO since 1994.
For this study the KCMEO database was searched for all deaths involving motor vehicles fires from 1994 to March 2011. Data were abstracted from the KCMEO database, autopsy reports, and scene and autopsy photographs. A secondary database was constructed containing decedent demographics, circumstances of the fatal incident, type of vehicle(s), seating position, identification methods, cause and manner of death, cause of fire, presence and severity of mechanical and thermal injuries, presence of soot deposition in the airway, and results of carboxyhemoglobin (COHb) analysis. Descriptions of vehicle type used standard terminology (20). The extent of thermal burns entered into the database was graded as follows: none, if there were no thermal burns; minor, if burns involved less than 20% total body surface area (TBSA); moderate, if burns involved between 20 and 50% TBSA; and extensive or charring, if burns involved greater than 50% TBSA. Because it was often difficult or impossible to distinguish extensive antemortem from postmortem thermal burns in scene deaths, the definition of extensive thermal burns was restricted to hospital deaths with burns greater than 50% TBSA. For scene deaths with burns greater than 50% TBSA, which invariably included at least some degree of charring or incineration, the extent of burns was graded as charring. The presence or absence of major blunt force injuries (BFI), for example, fractures or injuries of internal organs was entered into the database for each of three body regions: head/neck, torso, and extremities. The severity of BFI were graded as absent, survivable, or non-survivable based on their description in the autopsy reports, independently of the presence of soot in the airway, COHb saturation, and cause of death listed on the death certificate. Examples of non-survivable blunt force injuries include severe craniocerebral trauma, atlanto-occipital dissociation, cardiac rupture, aortic transection, and major visceral laceration. Unknown was entered into the database if the authors could not agree whether the BFI were survivable or not, or if the degree of incineration made it impossible to assign the severity otherwise. BFI in hospital deaths were entered as either survivable or absent. The cause of death from death certificates was simplified into one of four categories: fire-related only, if only smoke inhalation and/or thermal burns, without major BFI, were responsible for death; BFI only, if BFI alone were responsible for death; combination, if both fire-related injuries and BFI together were responsible for death; and other, if neither fire-related injuries nor BFI contributed to death. This last category included, for example, gunshot wounds, in which fire was subsequent and not directly related to death. COHb analyses on autopsy blood were performed by the Washington State Patrol Forensic Laboratory Services Bureau, Toxicology Laboratory, which provides toxicology services for death investigations throughout Washington. Analyses were performed using a CO-Oximeter (Model IL 682, Instrumentation Laboratory, Bedford, MA), and results were reported as percent saturation of total hemoglobin. Levels reported less than 5% saturation were regarded as negative or physiologically normal; only levels greater than 5% were regarded as elevated.
After all data were entered into the secondary database, normalized to consistent terminology, and verified for accuracy, data analyses were performed using Microsoft® Access and Excel to produce the results described below. For comparison of COHb results in vehicular fire fatalities with those found in house fire fatalities, the same KCMEO database was searched for house fire fatalities, and the corresponding COHb results were tabulated and analyzed in the same way as for the vehicular fire fatalities. Other information included in this study came from KCMEO Annual Reports.
Results
Demographics, Circumstances, Manners of Death, and Causes of Fires
Over the time period of this study, from 1994 to 2011, there were 2,472 motor vehicle fatalities investigated by KCMEO. During this time, there were 101 fatalities of motor vehicle fires included in this study. The deaths occurred in 75 separate incidents, in which 58 collisions were responsible for 83 deaths and 17 non-collision incidents accounted for 18 deaths. Seventy-one deaths occurred at the scene of the incident, and 30 were hospital deaths, delayed from the time of the incident from less than one day up to two months. In addition to the 101 deaths examined by KCMEO, there were seven additional deaths remaining at scenes outside of King County of incidents in which the survivors were transported to Harborview Medical Center where they subsequently died.
Description of 101 Vehicle Fire Fatalities in Study
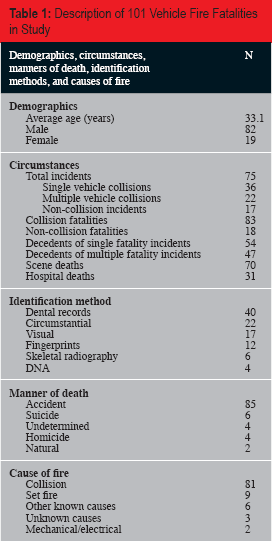
The cause of fire, also shown in
Of the six suicides, two were in fires in parked vehicles in which the decedents had intended suicide by vehicle exhaust. In one, death occurred solely due to carbon monoxide from the exhaust, and in the other, a combination of thermal burns and smoke inhalation from an unintentional fire starting from the exhaust system caused death. Manner of death was undetermined in four cases that were suspicious for suicide. Scene investigations and autopsies demonstrated that two deaths were natural; one was in a minor off-road collision into a ditch with subsequent fire, and the other was in an idling vehicle pulled off to the side of the road, in which fire started in the engine compartment.
Summary of Circumstances, Causes and Manners of Death of 18 Non-Collision Fatalities

Highly elevated COHb saturations indicate inhalation of vehicular exhaust prior to fire.
Analysis of Collision Incidents
Circumstances responsible for 78 collision fatalities certified as accident are analyzed in
Circumstances of 78 Fatalities in Post-Collision Fires

Numbers in this category do not total 78 (100%) because the number of collision partners per fatality ranged from 0 to 7. † Includes one camper truck and one school bus.
Analysis of Decedents’ Vehicles and Collision Partners in 82 Fatalities of 54 Post-Collision Fires *
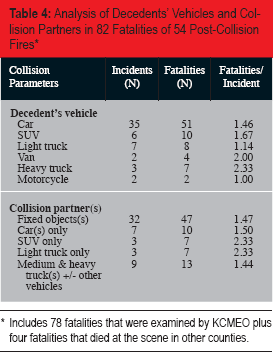
Includes 78 fatalities that were examined by KCMEO plus four fatalities that died at the scene in other counties.
Analysis of Collision Dynamics in 82 Fatalities of 54 Post-Collision Fires *
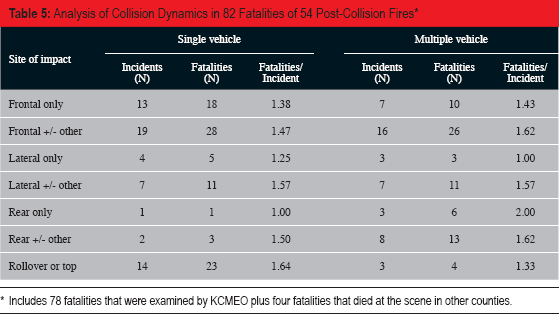
Includes 78 fatalities that were examined by KCMEO plus four fatalities that died at the scene in other counties.
COHb Analysis
Testing for COHb was performed in 65 of the 101 fatalities.
Results of Carboxyhemoglobin (COHb) Testing in 101 Fatalities
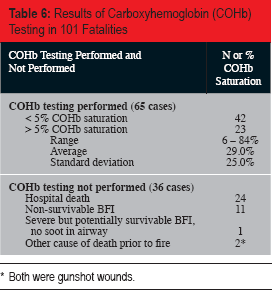
Both were gunshot wounds.
Correlation of BFI, Thermal Burns, and Inhalation of Combustion Products
In 75 collision fatalities certified accident, in which BFI could be reliably assessed, 65 had BFI of at least one of the three body regions; 34 were potentially survivable and 31 were non-survivable. Of 34 with survivable BFI, two had head/neck BFI only, eight had torso BFI only, 17 had both head/neck and torso BFI, and seven had extremity BFI only. Of 31 with non-survivable BFI, two had head/neck BFI only, four had torso BFI only, and 25 had both head/neck and torso BFI.
Correlation of Thermal Burns and BFI Severity in 75 Fatalities of Post-Collision Fires *

Three fatalities, all charred, were excluded from this table because the severity of the BFI could not be determined.
Correlation of Airway Soot Deposition and COHb Saturation with Injuries and Cause of Death in 41 Scene Fatalities of Post-Collision Fires
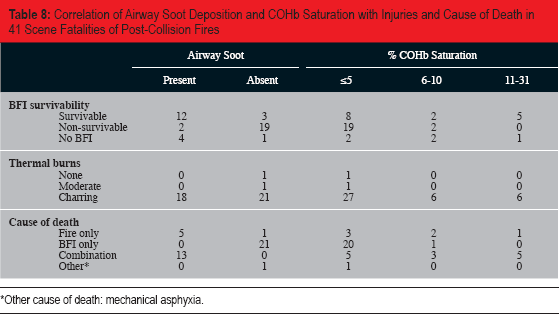
Other cause of death: mechanical asphyxia.
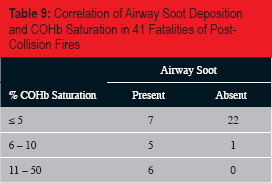
Correlation of Airway Soot Deposition and COHb Saturation in 41 Fatalities of PostCollision Fires
Discussion
The present study offers an examination of details involved in 101 vehicular fire fatalities investigated by KCMEO over a 16 year period. These vehicle fire fatalities represent approximately 4% of all motor vehicle fatalities investigated by KCMEO over the same time period, which is similar to 4.3% of motor vehicle fatalities involving fires estimated in national FARS statistics (1). Similar analyses of FARS data found that 2.4% of all fatal collisions experienced a fire (13). In the present study there were a total of 75 separate incidents, and of the decedents examined by KCMEO, 53% died in single fatality incidents and 47% died in multiple fatality incidents. The manner of death was accident in 84%, and collision was the cause of fire resulting in 80% of deaths. Of 16 non-accidental deaths (homicides, suicides, natural deaths, and deaths of undetermined manner), 69% were in parked cars. Overall, 4% of all deaths were homicides. Deliberately set fires, in homicides or suicides, were responsible for 9% of deaths. Only 2% of deaths were due to electrical or mechanical defects. These results compare with national statistics estimating in 2003-2007 that 58% of vehicle fire fatalities were due to collision, 8% were incendiary or suspicious, and 11% were due to electrical or mechanical failures (2). Furthermore, the results support general observations regarding fire fatalities cautioning that careful investigation is crucial to exclude criminal or intentional activity concealed or obscured by fire (3). As in all fire deaths, identification was a major concern, especially in charred bodies. Dental records were used to identify 65% of the decedents requiring scientific methods. This rate is in the range of 57% to 80% reported in a recent comparative study of transportation fire fatalities, which concluded that the success rate of dental identification varied considerably depending on the nature of the accident, the nationality and country of residence of the victims, the incidence of dental treatment, the availability of dental records, and the degree of dental injuries (5).
In 78 collision fatalities in which the manner of death was certified accident, 59% were in passenger cars, 60% were drivers, and 62% died in collisions with fixed objects or in non-impact rollovers. Analyses of FARS data found that single vehicle collisions were about 30% more likely to result in a fatal fire, compared to multiple vehicle collisions, and that impact with a narrow object (e.g., telephone pole or tree) was more likely to produce a fire than impact with a broad object (13). In the present study the vast majority (91%) of drivers were male, and half of the drivers were young males, less than 30 years of age. The male gender association with traffic collisions has been well-documented, and it appears that the association with vehicle fire fatalities is no different (21). Other cars were the collision partner in 10% of fatalities, while collisions with light trucks or SUVs and collisions with heavy and medium trucks accounted for 18% and 15%, respectively. The overall fatality rate, measured as fatalities per collision, averaged 1.52 and, for specific collision parameters, ranged from 1.00 to 2.33. Collisions involving occupants of heavy trucks and collisions with SUVs or light trucks had the highest fatality rates. These results may be explained by multiple factors including the high energy of collision with more massive vehicles, collision dynamics, entrapment of occupants subsequent to collision, and vehicle design. Data from FARS and Michigan traffic statistics found that post-collision fires were more likely in light trucks and fires subsequent to rollover of heavier weight vehicles were more likely to result in fatalities (13). Furthermore, several studies have shown that frontal collisions accounted for the majority of post-collision fires, while rear impacts, although less common, had the greatest propensity for fire (11–13). In a similar fashion the present study showed that impacts involving the front of vehicles represented the most common collision dynamic, occurring in 65% of 54 collisions, and claimed most lives (66% of 83 decedents). In contrast, purely rear impact collisions were relatively uncommon, accounting for only 7.4% of the collisions and 8.5% of the collision fatalities, but had the highest fatality rate of all collision dynamics. Also consistent with earlier observations (11–13), rollovers were a fairly common collision dynamic, occurring in 31% of collisions and accounting for 33% of collision fatalities.
Differences in the likelihood of a post-collision fire fatality are at least partly explained by where the fire originates (15–17). Fires following frontal impacts typically start in the engine compartment, are fueled by engine fluids and components, and spread relatively slowly into the occupant compartment. On the other hand, post-collision fires secondary to rear impact are usually ignited by hot components of the exhaust system, are fueled by gasoline leaking from a ruptured fuel tank or fuel line, and spread rapidly into the occupant compartment. Fuel tank placement is an important factor in post-collision fires, and previous studies demonstrated a significant decrease in post-collision fire fatalities after standards in 1976 placed the fuel tank above or forward of the rear axle (12, 22). Additional studies have concluded that interior and exterior plastics now surpass gasoline as the main fire load in most vehicle fires (23).
Determination of cause of death in a vehicle fire fatality requires consideration of the severity of mechanical trauma along with evidence of inhalation of products of combustion (4). The present study attempted to independently assess and correlate BFI severity, COHb level, and airway soot deposition. In 35% of all decedents tested for COHb, levels ranged from 6% to 84% saturation; the remainder had physiologically normal levels of COHb. Those with the highest levels of COHb were in parked cars and were at least partly due to carbon monoxide inhalation prior to the fire. In 41 fatalities in post-collision fires, COHb was elevated in only 29% of cases and ranged no higher than 31% saturation. This distribution was much different from that in house fire fatalities, in which COHb was elevated in 80% of 70 deaths and ranged up to 84% saturation.
The COHb results found in the present study compares with a similar distribution reported in a previous study, in which levels up to 92% saturation were detected in occupants of parked vehicles while levels in decedents of post-collision fires were no higher than 34% saturation (8). Other studies of fire fatalities due to all types of fires previously described show considerable variation in the levels of COHb depending on the type of fire, with higher levels detected in smoldering fires and lower levels in so-called flash fires or when an accelerant had been used (6, 7). One case report described a multivehicle collision in which flash fires from ruptured fuel tanks caused eight deaths exclusively due to thermal trauma with no elevation of COHb (24). Detailed analyses of mass fatality fires found significantly different levels of COHb in victims depending on their exposure to fire and heat relative to toxic gases, with decedents close to the fire source having low COHb levels and those far from the source having high levels (25, 26). Experimental modeling of fire dynamics demonstrated that heat and oxygen depletion were the primary threats to life in close proximity to the fire source while toxic gases, predominantly carbon monoxide, were the major threats further away from the fire (26, 27). Thus, it is reasonable to conclude that the relatively low COHb levels typical of postcollision fire fatalities, even with survivable BFI, are due to the rapid rate of fire generation fueled by accelerants and easily combustible materials as well as the close proximity of occupants to the fire source.
The present study observed, in 21 post-collision fire fatalities with non-survivable BFI, that only 9.5% had elevated COHb, compared with 44% of 16 decedents with potentially survivable BFI and 60% of five with no BFI. There is some question of the accuracy in assessing survivability of physical injuries in which post-collision fire eliminates all possibility of survival. Post-collision fires are more likely in high energy collisions in which severe BFI is expected (13, 14), and anatomic examination of a charred body from a rapidly developing fire is likely to underestimate the severity of mechanical trauma. Despite the likelihood of severe BFI in post-collision fires, it is notable in the present study that survivable and non-survivable BFI were nearly equally likely to be found in charred bodies recovered from the collision scene and that 12% of charred bodies recovered from collision scenes had no measurable BFI. Thus, the relative contributions of BFI and fire-related injuries must be carefully considered in arriving at an accurate cause of death determination. Although it has been suggested that COHb levels less than 20% saturation indicate a cause of death other than fire (8), the results of the present study support the conclusion that low levels of COHb are expected in post-collision fires, even when fire-related causes are the major or sole contributor to death. Rather than toxic asphyxia due to carbon monoxide inhalation, the mechanism of death is likely to be a combination of oxygen depletion, extreme heat, and inhalation of hot gases or fire (17, 27). This concept is further supported by clinical observations in which inhalational injuries are the major cause of hospital deaths resulting from motor vehicle fires (18, 19).
The standard measure of viability during a fire is evidence of inhalation of products of combustion. Soot deposition in the airway and/or elevated COHb saturation provide evidence that the victim was alive in the fire and had at least some period of post-collision survival (3, 4). However, neither of these findings constitute proof that the victim would have survived had it not been for the fire. Furthermore, as discussed above, the absence of elevated COHb does not prove that death was not due to fire or that fire was not an important contributor to death. In the present study, COHb levels and airway soot deposition correlated imperfectly with the severity of BFI. Airway soot deposition was found in 80% of decedents with no BFI, in 80% of decedents with survivable BFI, and in 10% of decedents with non-survivable BFI. Compared with this, elevated COHb was present in 60% of decedents with no BFI, 47% of decedents with survivable BFI, and 10% of decedents with non-survivable BFI. In charred bodies, airway soot deposition was present in 46% while elevated COHb was present in 31%. In certifying cause of death, airway soot deposition and/or elevated COHb were used as markers to indicate viability during the fire. In those with either marker, fire related causes (thermal burns and/or smoke inhalation) were regarded as either the sole cause of death, if BFI was absent, or in combination with BFI present. Airway soot deposition appeared to be a more sensitive marker of viability during the fire. In 30 cases in which COHb was not elevated, airway soot was detected in 24%. Although the present study considered COHb saturations greater than 5% as elevated, it has been reported that levels of 10% or more may be seen in heavy smokers (28). Further complicating interpretation of COHb analyses, especially for lower levels of COHb, spectrophotometric determinations do not always correlate with other methodologies (29). The results of the present study demonstrated the importance of considering both markers, elevated COHb and airway soot deposition, together as reliable evidence of viability in post-collision fires.
Previous studies have attempted to demonstrate the excess burden of deaths due to post-collision fires (1, 10,17). In view of the foregoing discussion, it is understandable why it is difficult to estimate the proportion that would have survived had it not been for fire. In previous studies, data from North Carolina indicated that 17% of vehicle fire deaths were due to fire-related causes, compared with data from Texas showing that 32% of the deaths were due to fire (1). The remainder of the deaths were either due to BFI or “undetermined”. When the “undetermined” category was removed from both sets of data, there remained a twofold difference in the estimates between the two sites, leading to the extrapolation that between 274 and 575 deaths occur annually due to fire in post-collision fires in the United States (1). However, models predicting fatalities based on crash severity found that fully 77% of fatalities in vehicle fires were unaccounted for by BFI alone (10, 17). The differences were at least partly due to the way injuries were interpreted and how deaths were certified and reported (17). In the present study, the percentage of deaths in which post-collision fire contributed substantially to death, meaning that the decedent would have survived had it not been for the post-collision fire, was somewhere between 13% and 59%, with the lower percentage based on the number of collision fatalities with no BFI and the higher percentage based on the number of fatalities with no BFI or potentially survivable BFI.
Limitations of the present study include those inherent in any study of fire fatalities. Fire destroys so much evidence that many questions remain unanswerable. Furthermore, it is impossible to control for all the variables of either collisions or fire. Because the study included hospital deaths, scene investigations in many cases were not conducted by KCMEO, leaving certain gaps in the data. As previously mentioned, anatomic assessment of BFI survivability in charred bodies probably leads to overestimating the contribution of fire-related causes. Although an attempt was made to calculate the fatality rates according to different collision parameters and dynamics, this measure suffers from a relatively low sample size. There were no attempts to evaluate particulars of vehicle make, design or age, characteristics of damage, source of ignition, combustion materials, entrapment of occupants, or velocity of collision, all of which are factors in the likelihood of post-collision fire and subsequent fatalities (13, 15,16). Ethanol intoxication was disregarded in the data collection, as it is well known to be an important contributor to vehicular collisions in general (for example, see KCMEO Annual Reports). There were no measurements of the variety of potential pyrolytic toxins generated in fires involving vehicle interiors (30). Several studies have evaluated cyanide and other toxic gases in fire fatalities and generally concluded that their contribution is probably of secondary importance and not independent of carbon monoxide, heat, and oxygen depletion (25–27, 31–33).
Despite the limitations, the results of this study have implications for both medicolegal death investigation and traffic safety. It is imperative that autopsies be performed in vehicle fire fatalities to accurately certify cause and manner of death. It cannot be assumed that a burned body died due to fire. Autopsy findings must be considered in the context of a careful scene investigation to reveal homicides or suicides. Fires in parked vehicles were more likely to be due to intentional acts compared with those in moving vehicles. Airway soot deposition was a more reliable marker than elevated COHb for post-collision fire viability, and considered together they were highly correlated with BFI survivability. The results of this study indicate that death certificates alone are not an accurate measure for estimating excess fatalities due to post-collision fires. Demonstrating inhalation of combustion products is merely evidence that the decedent was alive during the fire but does not prove that the decedent would have survived the physical injuries for any meaningful period of time. Conversely, absence of elevated COHb is not evidence that the occupant died before the fire. Although it is difficult to estimate the excess burden of deaths due to post-collision fires, in the present study somewhere between 41% and 87% of collision fatalities died of mechanical trauma and not fire.
Footnotes
The authors, reviewers, editors and publication staff do not report any relevant conflicts of interest.