
Abstract
With the expansion of the shipping and cruise ship industries, there is a need for a more complete understanding of the mortality risks at sea. We conducted a retrospective review of shipboard deaths coming under the jurisdiction of the County of Los Angeles Department of Coroner during the years 2000-2011. Sixty-one shipboard deaths were identified, of which 24 (39%) were among crew, and 37 (61%) were among passengers. Among both crew and passengers, there was a prominence of deaths due to cardiovascular disease. Also prevalent were accidents due to blunt trauma, accidents involving ethanol or medications, and suicides. The identification of multiple potentially preventable deaths after onset of symptoms at sea underscores the need for further improvements in maritime telemedicine, crew medical capability and long-distance evacuation.
Introduction
World seaborne trade increased from 5.98 billion tons loaded in 2000, to 8.41 billion tons in 2010 (1). Worldwide, 19.2 million passengers were carried on cruise ships in 2011. This total of passengers carried worldwide is estimated to increase to 22.4 million in 2015 (2). With this expansion of the shipping and cruise ship industries, there is a need for a more complete understanding of the mortality risks at sea, in order to design interventions to reduce those risks in the future.
The Port of Los Angeles is situated on San Pedro Bay, 20 miles south of downtown Los Angeles. As measured by container traffic, it is the busiest port in the United States and the 16th busiest port in the world (3, 4). The Port of Los Angeles is the site of the World Cruise Center, which handled 1.2 million passengers in 2008 (5).
We present the experience of the County of Los Angeles Department of Coroner with shipboard death occurring among passengers and crew.
Materials and Methods
The County of Los Angeles Department of Coroner covers a population of 9.8 million. Between
January 1, 2000 and December 31, 2011, 55,459 autopsies were performed. Cases were identified retrospectively based on the following criteria: (a) the death occurred on board a sea-going ship (cargo ship, oil tanker or cruise ship); (b) the death falls under the jurisdiction of the Los Angeles Department of Coroner. Evaluation of each case included review of investigator's report, autopsy report, toxicology findings, and reports of any additional studies or consultations including histopathology, microbiology, neuropathology and radiology.
Results
A total of 61 shipboard deaths were identified in the 12-year interval from 2000 through 2011. Of these, 24 (39%) were crew, and 37 (61%) were passengers. Full autopsies were performed on 96% of the crew, and 30% of the passengers. There was one stowaway counted with the passengers. Crew and passengers and are treated separately in the subsequent analyses.
Among the crew, 23 (96%) were male, and the mean age was 46 years. The manner of death was natural in a majority (62.5%), with accident being the next most common manner (21%)
Characteristics of Crew Members

Probable ethanol withdrawal and excess water intake as contributing factors
Ruptured appendicitis as a contributing factor
Among the passengers, 22 (59%) were male, and the mean age was 65 years. The manner of death was natural in a majority (84%), with accident being the next most common manner (8%)
Characteristics of Passengers
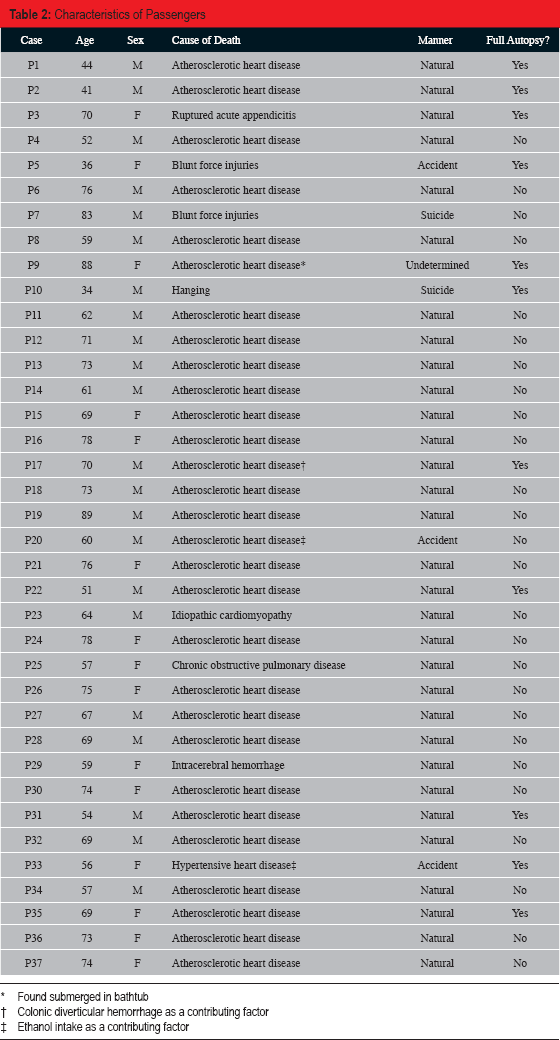
Found submerged in bathtub
Colonic diverticular hemorrhage as a contributing factor
Ethanol intake as a contributing factor
Examining only those 11 passengers on whom full autopsies were performed reveals similar results. Among the fully autopsied passengers, six (55%) were male, and the mean age was 56 years. The manner of death was natural in a majority (64%), with accident being the next most common manner (18%)
In the majority of cases, death was pronounced at sea, with only four (17%) of the crew and two (5%) of the passengers pronounced in port. With the exception of the stowaway on a cargo ship, all passengers died on cruise ships. Among crew, 15 (62%) were on cargo ships, five (21%) were on cruise ships, and four (17%) were on oil tankers.
In six cases, death may have been prevented had the decedent been able to receive a higher level of care in a timely manner. Of these potentially preventable deaths after onset of symptoms or injury, four (67%) were among crew
Potentially Preventable Deaths

Discussion
We report 61 shipboard deaths coming under the jurisdiction of the County of Los Angeles Department of Coroner during the years 2000-2011. We find a predominance of deaths due to cardiovascular disease. Also prevalent are accidents due to blunt trauma, accidents involving ethanol or medications, and suicides. Although we did not identify deaths due to contagious disease in this study, such deaths (for example, due to ship borne gastroenteritis) would be considered Coroner's cases (written communication, David Kim, MD, October 1996 involving a passenger who had norovirus gastroenteritis diagnosed by a Los Angeles County Medical Examiner/Coroner autopsy). The identification of multiple potentially preventable deaths after the onset of symptoms underscores the need for further improvements in maritime telemedicine, crew medical capability and long-distance evacuation.
Our retrospective study is limited by the availability and quality of data from cases handled up to 12 years previously. While almost all crew cases received full autopsies, only about 30% of passenger cases received full autopsies. Autopsies were less likely to performed on passengers if there was no suspicion of foul play during investigation, and if there was a strong clinical impression of a natural cause of death in some-one older than 60 years. Crew tended to be autopsied regardless of circumstances in part because of the additional regulatory and epidemiologic scrutiny accorded occupational fatalities. This special interest in occupational fatalities, with the attendant unique risks that crew members face, explains why crew and passengers are analyzed separately in this study. As discussed in the results above, the passenger cases with full autopsies showed general characteristics similar to those from the whole passenger group.
The shipboard population presenting to the Port of Los Angeles does not comprise all seafaring groups equally. In particular, the mortality in the fishing industry is not represented in the deaths described in this study.
Our finding that 37.5% of deaths among crew were non-natural is similar to that reported by Oldenburg et al. (6), who found that non-natural deaths comprised 40-50% of all crew deaths in a review of three studies of occupational mortality among European seafarers on merchant ships. The occurrence of three industrial accidents by blunt force injury among the 24 crew deaths in our study speaks to the risks of the occupation, and the need for ongoing vigilance to prevent accidents during movement of heavy objects and during deck activities in heavy seas. Accidents among seafarers are substantially more common when compared to those among other workers, with a relative risk of 24 found in a study of workers in Great Britain (7).
The risk of natural death is also increased among seafarers. A study of over 24,000 Danish merchant seafarers found an increased risk for natural death (standardized mortality ratio (SMR) 1.13, 95% confidence interval (CI): 1.02-1.24) when compared to the general population, with a particularly increased risk among non-officer deck and engine room crew (SMR 1.60, 95% CI: 1.39-1.84), and a notably higher risk of alcoholism among all seafarers (SMR 2.82, 95% CI: 1.77-4.26) (8). The absence of a “healthy worker effect” among seafarers has led to the suggestion that they have generally more risky lifestyles apart from their more hazardous work environment (8–10).
In addition, there is an increased likelihood of suicide among seafarers when compared to the general population, as found in the above-men-tioned study by Hansen et al. (SMR 1.77, 95% CI: 1.41-2.20) (8) and in another study showing an over two-fold increase in the suicide rate among non-officer Finnish crew members (11). Our finding of suicides in three of 24 (12.5%) crew deaths is consistent with the proportion of suicides found among deaths of Polish merchant seafarers (10.2%) (12). Risk factors for suicide that have been identified among seafarers include comorbid mental illness, substance abuse, isolation, work and family stress, and a recent change of ships (11, 12). Reduction in suicide risk may be achievable by psychological screening at the start of voyages to identify and intervene with those found to be at high risk.
The preponderance of death due to cardiovascular causes among both crew and passengers indicates the potential to reduce mortality with improved or novel interventions. Improvement in prevoyage cardiovascular risk assessment and preparation has been suggested both for passengers (13) and crew (14, 15). Sudden changes in the behavior of passengers while on cruises, with respect to alcohol consumption, dietary indulgence and physical activity may place some at particularly high risk (13). On-board interventions to steer passengers away from such behaviors may be appropriate. There is also an opportunity for long-term cardiovascular risk modification among crew while on board, includ-ing dietary changes, smoking cessation, moderation of alcohol intake, increased physical activity (with possible addition of exercise rooms) and blood pressure control (14, 16).
While standards for ship medical facilities and staff have been established for many cruise ships (17), the capabilities on cargo and tanker ships are more limited. Improved maritime telemedicine capabilities hold promise for all ships at sea, but these will not supplant the need for improved medical knowledge and training among seafarers to enable them to handle emergencies when there is no doctor aboard, with or without a telemedicine link (18).
Footnotes
The authors, reviewers, editors and publication staff do not report any relevant conflicts of interest.